What They Don’t Tell Us About Treating PainExposing the pain industry and the forgotten treatments for painStory At Glance
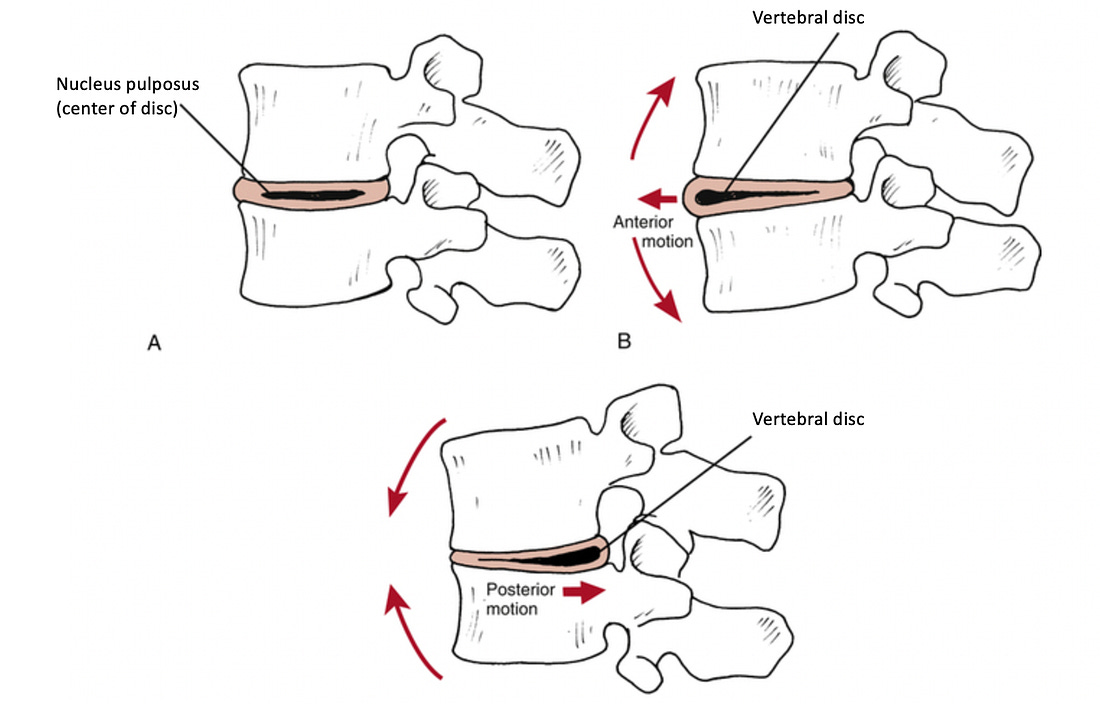
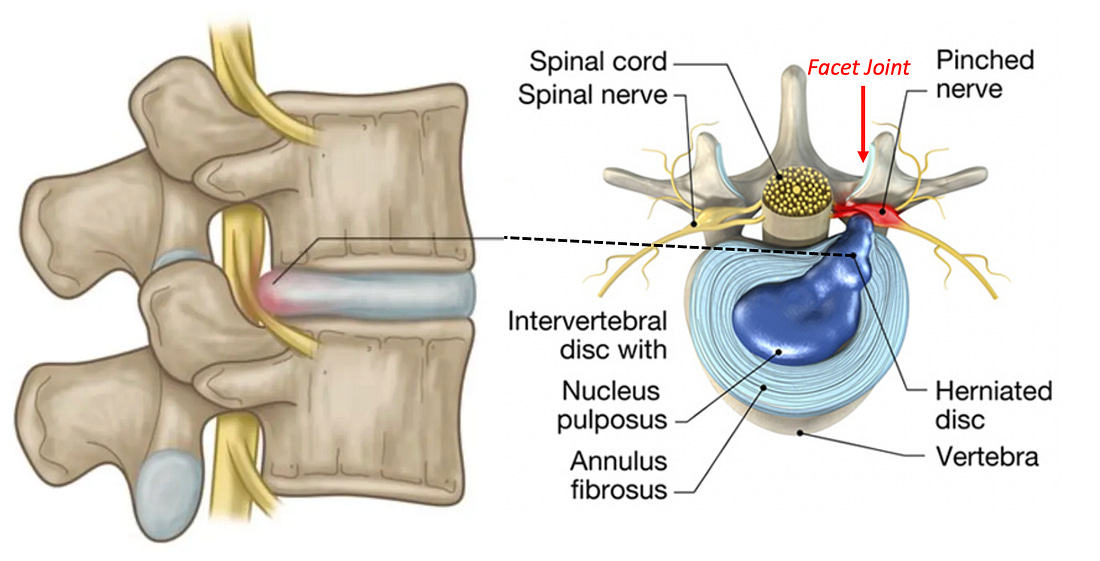
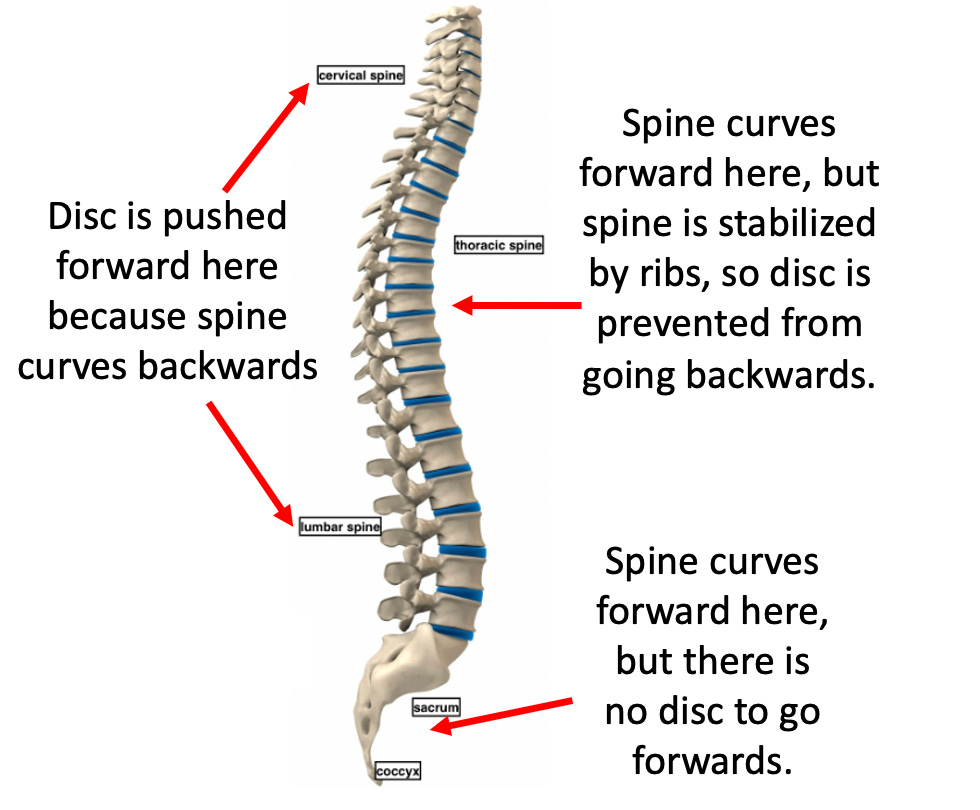
Most patients with chronic pain will typically first be recommended a variety of pain medications and physical therapy, then once those fail, steroid injections, and then a joint surgery. Unfortunately, each step in this process is often ineffective at addressing the patient’s pain or creates a variety of complications that make their situation even more unbearable. For this reason, it is critical to understand the risks of each part of this process and the safer alternatives that can permanently alleviate joint and spinal pain. Note: persistent or recurrent pain after spinal surgery, back pain following spinal surgery is referred to as “Failed Back Surgery Syndrome” and affects between 10-40% of people who receive a spinal surgery. Common Spinal Pain Generators:In most cases, joint pain has a cause that must be identified to treat it. For example, when treating spinal pain, we find it is critical to address:
Additional Pain Generators:
Systemic MedicationsSince joint or spinal pain has multiple causes and diagnosis is time-consuming, physicians typically prescribe pills or refer patients elsewhere rather than address the root causes of their pain. Common medications include NSAIDs, Tylenol, Steroids, Gabapentin (or Lyrica), and Opioids—all with major issues. Note: due to the high rate of addiction which follows opioid prescriptions (and the societal damage that follows), more and more, the government has moved to restrict opioid prescriptions. Because of this, patients in significant pain who will only respond to opioids, despite their best efforts, often cannot get these drugs and instead are given another ineffective option (e.g., NSAIDs), hence making it imperative that effective non-opioid solutions for pain be made available to the public. NSAIDsNSAIDs (e.g., ibuprofen, naproxen) temporarily reduce pain but only partially, leading patients to overuse them—often dangerously, as NSAIDs are toxic at high doses (which frequently occur since NSAIDs are taken for pain and are available over the counter). Many consider NSAIDs among the most hazardous drugs in the U.S. because:
Unfortunately, NSAIDs remain amongst the most commonly prescribed drugs, and are frequently given for musculoskeletal injuries. Note: the dangers of NSAIDs are discussed further here. TylenolTylenol (acetaminophen) is one of the few over-the-counter alternatives to NSAIDs and is generally considered safer, though often ineffective for severe pain. Still, it carries serious risks:
Gabapentin and PregabalinGabapentin (Neurontin) was originally approved to treat epilepsy—a small market. After approval, Pfizer aggressively pushed it for unapproved uses, especially neuropathic pain, despite limited evidence. The federal government fined Pfizer nearly $1 billion for illegal promotion. While less toxic than NSAIDs, side effects for these drugs are common and include: lethargy, dizziness, sedation, and cognitive impairment, as well as rarer but serious reactions like respiratory depression and hypersensitivity. Gabapentin can also be habit forming. Note: since gabapentin and pregabalin (Lyrica) only work for specific types of pain (e.g., neuropathic pain), they typically do very little for most patients’ pain. However, they are widely prescribed because they lack many of the severe risks associated with other pain reducing drugs, and as a result, many are placed on inappropriate prescriptions for them. CorticosteroidsInitially hailed as a wonder drug, corticosteroids like prednisone and hydrocortisone gradually were discovered to have significant side effects (e.g., weight gain, adrenal suppression, heart attacks, diabetes, insomnia, and psychiatric effects). Since corticosteroids trigger tissue breakdown, they also often greatly weaken the body's structural integrity, impair wound healing and weaken collagen synthesis. Furthermore, corticosteroids double one's risk of fracture (especially vertebrae), with 12% of users reporting fractures. Steroids cause 5-15% bone loss yearly, and 37% of long-term users experience vertebral fractures. High doses increase vertebral fracture risk fivefold. Higher doses also cause avascular necrosis in 6.7% of users. Likewise, they greatly impair wound healing, collagen Note: the primary drugs used to treat Osteoporosis (bisphosphonates) have severe side effects have severe side effects including making the bones more likely to break. In turn, one of the few approved uses for bisphosphonates is steroid-induced bone loss. Since both collagen, ligaments (which are composed of collagen) and bones are weakened by steroids, chronic use leads to joint weakening and chronic pain. Because of this, we frequently encounter patients who achieved a temporary alleviation of joint pain (e.g., in the spine or knee) who then have their condition worsen and require surgery. Unfortunately, this side effect is rarely disclosed to patients, leading to many surgeries that could have been prevented. Note: in many cases, if joint pain is instead treated by strengthening the ligaments (e.g., with nutritional supplementation or prolotherapy), the pain will resolve and future surgeries can be prevented. The Surgery FunnelSurgeries often have risks that patients don't learn about until after complications occur, which is problematic since you can't "undo" surgery. For this reason, patients should seek unbiased second opinions from doctors who aren’t being paid to do a proposed surgery. Unbearable pain (e.g., in a joint) is one of the strongest motivators for surgery, and spinal surgeries are the most common elective surgery I'm consulted about. Unfortunately, since spinal surgeries are one of the most profitable areas in medicine, there's reluctance to consider if risks outweigh benefits or if safer and more effective alternative exist, and over the years I’ve become increasingly skeptical of them, as while some are necessary and help patients, many are not. Likewise, despite trillions spent on spinal pain (e.g., in 2016, 134.4 billion dollars was spent on neck and low back pain in the USA), most patients remain stuck with chronic pain and experience significant side effects from treatments. Note: there have been numerous newspaper investigations of spinal surgeons who recklessly performed large volumes of unnecessary surgeries, killing or injuring many of their patients who were nonetheless protected by their hospitals because of how much revenue they generated. DMSO: A Safer AlternativeOver the last seven months, I have been working to spread awareness of dimethyl sulfoxide to the world, a natural compound which provides dramatic benefit for a variety of challenging conditions (e.g., autoimmunity, strokes, paralysis, antibiotic resistant infections, cancers, vision loss and tinnitus). DMSO
also increases blood circulation to tissue, reduces inflammation,
interrupts pain transmission, relaxes muscles, and decreases activity of
the sympathetic nervous system. Because of this, DMSO is highly
effective at: For example, in this article,
I summarized dozens of studies (comprising thousands of patients) which
consistently showed DMSO improved the majority of musculoskeletal
conditions it was tested on (e.g., one of 38 patients with lumbar and disc herniations that found DMSO made them recover twice as quickly). Likewise, I have now received thousands of remarkable testimonials from readers who used DMSO, most of which were of a significant improvement in pain or rapid healing of an injury. In parallel, many doctors such as James Miller MD have been inspired to use in their practice and seen similar remarkable results for a variety of challenging conditions. Note: in about 10-15% of people of people DMSO does not help their chronic pain. Typically this is either due to it being a chronic issue (where it can often take up to six weeks to get a response), too low of a dose being used, or the pain being psychiatric in nature (as from the earliest days of DMSO research, Merck noted that type of pain had a poorer response to DMSO). For musculoskeletal injuries (e.g., pain or injuries), in most instances where a steroid or NSAID would be used, we find DMSO: •Is more effective at addressing the immediate issues. As such, for years, we’ve found that in most cases where drugs like NSAIDs are widely used, much better and far safer results could be obtained from DMSO. Unfortunately, while this was recognized in the past (e.g., many professional athletes in the 1960s and 1970s found DMSO dramatically improved their ability to recover from injuries and facilitated rapid returns to the field), all of that has now been largely forgotten. Consider for example, this 1980 60 Minutes episode: Lastly
one of DMSO’s key properties is that it can potentiate other substances
and carry them inside the body (thereby making it possible to
administer IV medications topically). As an almost infinite number of
substances can be combined (e.g., I’m familiar with hundreds that have
been successfully enhanced with DMSO combinations), this area still
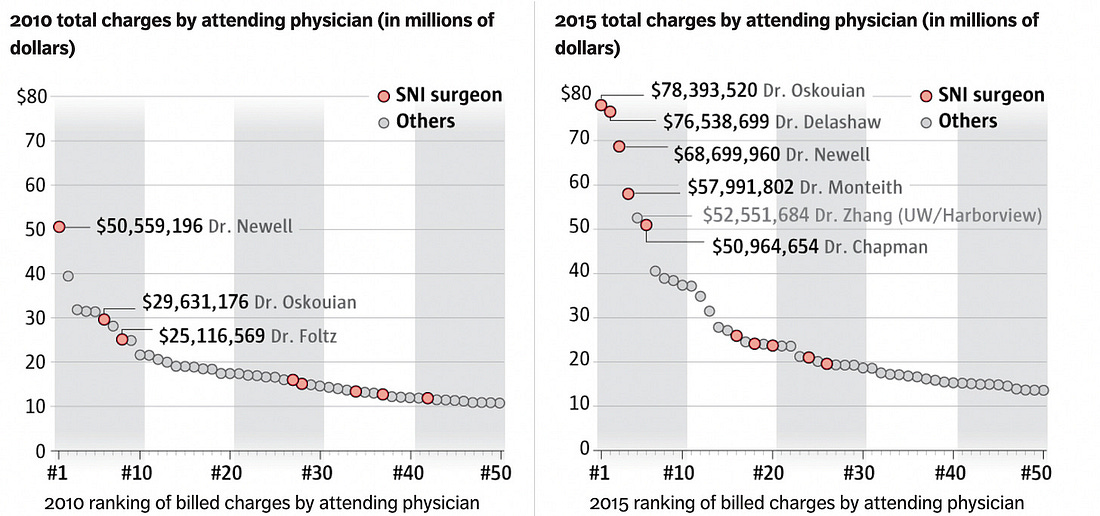
remains greatly understudied. ConclusionThe medical business model revolves around maximizing sales, either by perpetually selling a patient medications or by funneling them into high ticket items, and as I’ve tried to show here, pain management exemplifies this business model. For instance, spinal surgeries (the last step for many patients whose pain was improperly managed), can make a hospital well over 100,000 each. In turn, as an investigation of numerous botched neurosurgeries showed, ambitious neurosurgeons (e.g., those who wanted to do so many surgeries they would often have multiple operating rooms running concurrently) will make enough money to sustain a hospital:
Similarly, as this article showed, patients with chronic pain are often put onto lifelong prescriptions of pain medications which fail to address much of their pain, have significant (and sometimes life-threatening) side effects, and frequently force them down the sales funnel to the lucrative joint and spine surgeries. That predatory business model in turn, was exemplified by Purdue Pharma, which bribed an FDA reviewer to claim their proprietary opioid (OxyContin) was not addictive. In 1995, the drug was then marketed with that claim and having the American Pain Society declare “pain was the 5th vital sign,” compelling doctors to routinely assess for it and treat any existing pain with opioids (as otherwise they faced malpractice investigations from state medical boards). This, in turn, created the modern opioid crisis (as many opioid users develop permanent addictions after brief courses of these “non-addictive” drugs) which eventually affected so many communities doctors lost much of their ability to prescribe opioids to patients with crippling pain nothing else worked on. In my eyes, the root cause of all of this is that since pain is an ideal market, there is very little interest in looking at either the shortcomings of existing treatments or looking into actual treatments for pain which destroy that perpetual revenue stream. Fortunately, the need to reduce wasteful spending (e.g., for costly and unnecessary surgery) MAHA moment is at last giving us a chance to change things and begin looking at the actual causes and treatments for these conditions rather than costly ones that do neither. Author's note: This is an abridged version of a longer article
that goes into more detail on dangers of common pail killers like
NSAIDs and safe alternatives for treating neck and spine pain (which can
be read here), along with a companion article on how DMSO can treat pain injury and arthritis (which can be read here), an article on the dangers of corticosteroids (which can be read here) and an article on the many dangers of spinal surgery (which can be read here). To learn how other readers have benefitted from this publication and the community it has created, their feedback can be viewed here. Additionally, an index of all the articles published in the Forgotten Side of Medicine can be viewed here. You're currently a free subscriber to The Forgotten Side of Medicine. For the full experience, upgrade your subscription.
|
No comments:
Post a Comment