The Forgotten Dangers of Ultrasound
What no one tells you about having a healthy pregnancy

Story at a Glance:
•The
medical field has had a long history of exposing mothers to
“treatments” that harm their infants. After decades of work to stop the
routine x-raying of fetuses, the “safe and effective” practice of
prenatal ultrasound (US) was adopted in its place.
•While US is thought to be safe, there are decades of research showing it can harm tissues. Initially, this was well recognized, but as the ultrasound industry took off, it became a forgotten side of medicine, and research in this area became almost impossible to conduct.
• There is a large body of evidence showing fetuses are particularly vulnerable to US. Most concerningly, dozens of trials were conducted in China immediately prior to mothers planning to have abortions, which showed giving an US beforehand clearly damaged fetal tissues.
•The harms of US are dose dependent. Unfortunately, in 1992, despite widespread concerns about the safety of prenatal US (e.g., CNN did a program on it) the FDA chose to raise the permissible US levels 8-fold (and often more). Given that the studies showing the dangers of US were conducted at levels far below the original threshold, this increase is quite concerning, and may have played a pivotal role in the outbreak of chronic childhood illnesses that occurred around this time.
•Conversely, the benefits of prenatal US are often vastly overstated, and in many cases put mothers on unnecessary “treatment” plans which harm them and their infants.
•This article, we will review the body of literature on the risks and benefits of prenatal US, alternatives to prenatal US, and the strategies for pregnant mothers we have found are the most helpful to ensure a healthy and vibrant child, along with strategies for preventing common pregnancy issues like miscarriages, pregnancy back pain, swelling and preeclampsia.
One of the human body’s most incredible aspects is its capacity to adapt to many different environments and tasks. Unfortunately, this adaptability has a significant drawback. The earlier in life an input enters one’s system, the more of a long-lasting effect it has on each aspect of one’s being. Psychologically, for example, experiences in early childhood (e.g., abuse or trauma), including those so early on the individual can’t even consciously remember them, can often pattern the rest of the individual’s life (and in many cases their descendants as well).
Tragically, that principle has also been deliberately utilized throughout history to create obedient subjects.
Note: this principle has also been abused throughout history to create lifelong loyalty (e.g., this is the reason why the fast food industry devotes so much marketing to children, and McDonald’s puts such a big focus on Happy Meals).
Similarly, within medicine it’s well recognized that being exposed to a toxin or infection as a fetus (especially in the first two months of life) can be immensely consequential for the rest of their life (e.g., by causing birth defects).
Unfortunately, this principle is frequently ignored (e.g., by pushing the COVID vaccine on pregnant mothers). Many of us believe the wanton disregard of it (e.g., with the bloated childhood vaccine schedule—the harms of which are discussed further herer) is a root cause of many of the chronic illnesses our society now faces.
In this article, I will cover a danger most of our children are exposed to that is seldom recognized.
“Safe and Effective”
One of the foundational axioms (truths) medical students are taught from the very start is that vaccines are “safe and effective” and that the only reason anyone believes otherwise is that they were misled by Andrew Wakefield’s fraudulent autism study (as opposed to say serious concerns about vaccines causing severe neurologic injury existing for over a century).
As such, you see routinely remarkable situations like students being taught about SIDS (sudden infant death syndrome) and being told, “We know it clusters around 2 to 4 months (and always occurs by 6 months),” but “We still don’t know what causes it” while simultaneously wholly ignoring the fact those are the exact same times infant get their largest dose of vaccines, or that for a century physicians and parents have pointed out certain vaccines caused SIDS.
Thus, if you ever question the safe and effective vaccine narrative (particularly since so much of a doctor’s identity is wrapped in the mythology that medicine “saved humanity” with vaccines), it is typically a lost cause and often leads to strict professional reprisals from the majority of your peers.
In turn, despite my willingness to challenge medical dogmas, I was quite hesitant to write this article. This is because:
•While some doctors are open to the idea vaccines can be harmful, almost none feel that way about ultrasound.
•I’ve
noticed doctors are typically much more willing to question the safety
of drugs that are not routinely prescribed within their speciality than
those that are (e.g., I am yet to meet a dermatologist who will
acknowledge Accutane is dangerous, whereas I’ve met many psychiatrists
who have serious reservations about it—as they frequently have to deal
with the psychiatric side effects it creates). In the case of US, I am a
fan of the myriad of things it makes possible, so I am effectively
trapped by a similar bias that leads to a reluctance to question this
practice.
However, as I thought more about it, I realized US’s routine use in obstetrics has several remarkable parallels to childhood vaccination. In both cases, initial serious concerns about the safety of the practice existed throughout the medical profession. Yet, as time went on, the lucrative market the product created pushed those concerns to the wayside. Before long, the government sanctified the safety of the practice, at which point an inexorable proliferation in its use occurred. In time, virtually everyone had forgotten those concerns existed and that the vast proliferation of its use might have consequences or that any ethical reason existed to test its safety.
Most importantly, both of these practices harm the most vulnerable members of society (who cannot speak out for themselves), so what follows needs to be said.
The Medicalization of Childbirth
A
classic way any industry creates profits is to create markets and
monopolies out of thin air. In turn, throughout medicine, we see a
recurring pattern—a previously “normal” condition is medicalized, and
the population is eventually convinced they need to perpetually purchase
products for said condition (a process referred to as “disease
branding”). For example, in this article
I showed how effectively this was done with “depression.” Likewise
throughout this publication, I’ve shown why many of the vaccines we
routinely give our children just really aren’t needed.
Note: the relative risks and benefits of each childhood vaccine are discussed in more detail here.
One of the worst places this has happened is with childbirth, where what was previously seen as a natural process has been transformed into a medical emergency that requires the constant attention of a medical team. As best as I can tell, this began with Harvard’s (influential) first professor of obstetrics, who initiated the push to replace female midwives with male physicians and in 1820 stated:
Women seldom forget a practitioner who has conducted them tenderly and safely through parturition they feel a familiarity with him, a confidence and reliance upon him which is of the most essential mutual advantage. . . . It is principally on this account that the practice of midwifery becomes desirable to physicians. It is this which ensures to them the permanency and security of all their other business.
Since
that time, there has been an increasing medicalization of childbirth,
which while helpful has also created a massive number of highly
consequential complications for both the mother and child (to the point
we advise home birth whenever it is feasible).
Note:
home birthing, the dangers of hospital births, and the issues with fetal
heart rate monitoring (a common part of the hospital birth process)
will be covered in the next part of this series.
In all of this, the key principle to understand is that the earlier something is changed in a human being (and most other living organisms), the more profound and lasting the consequence will be for the human being. As such, we frequently find that the chronic issues patients have, originated during childbirth and in many cases, before they were even born (e.g., due to an emotional shock to the mother). This in turn, helps to explain why harmful obstetric interventions can often be so consequential for a child and why it is such a tragedy our society does not afford the reverence, respect, and support to mothers you see in many other nations (e.g., for a Westerner, it’s remarkable to observe the respect and care China gives to pregnant women).
Note: many modern obstetric practices are done to shield doctors from liability for any complications children experience. Yet, despite being by far the most expensive place to give birth to a child (excluding Japan), 0.56% of American infants do not survive childbirth, resulting in over 50 nations (including every affluent one) having a lower infant mortality rate than the United States. Likewise, the US ranks 65th in the maternal death rate from childbirth—all of which indicates we may be focusing on the wrong things in childbirth.
EMF’s and Childbirth
With electromagnetic fields, we’re told that:
•The
only way electromagnetic radiation can damage the body is by creating
ionizing radiation that breaks apart molecular bonds, creating free
radicals that damage DNA.
•The EMFs we are routinely exposed to (e.g., from cell phones) are far too weak to be ionizing radiation.
•Therefore, any idea that common EMFs can cause issues is highly unscientific and misguided.
Unfortunately, this set of arguments ignores two major points:
•First, many biological structures are incredibly sensitive to EMFs, and as a result, fields far lower than what we are commonly exposed to can create physiologic effects.
•Microwaves (which are utilized by many modern wireless technologies such as cellphones, wifi, and radar) are uniquely suited to be absorbed by biological tissues, and therefore are “toxic” at non-ionizing doses.
Note: in addition to what I (and many others) have witnessed in a large number of EMF-sensitive patients, there is a large body of evidence demonstrating that EMFs can have adverse physiologic effects (e.g., see this book and this book and this article). Much of this was done in Russia as they lacked the commercial interests to censor that research (as acknowledging the harm of EMFs in the West would be very damaging to the military and the wireless industries).
Since little things done to a fetus during gestation can be immensely consequential for the rest of their lives, many have wondered if EMF exposure during pregnancy can affect the child’s long-term health. In turn, there is some supporting evidence for this. For example:
•Researchers at Kaiser Permanente gave pregnant women EMF meters to wear for 24 hours. The children of women whose exposure exceeded 2.5 milliGauss were more than six times as likely to be obese as teenagers than the children of mothers whose exposure was lower than that amount.
•Suspecting there might be a link between EMF exposure and neurological disorders, Dietrich Klinghart (a renowned integrative medicine physician) conducted a study where he compared the prenatal EMF exposures of 10 neurologically impaired children (8 of whom were autistic) with 5 controls. He found high prenatal EMF exposures dramatically increased the risk of neurological disabilities:
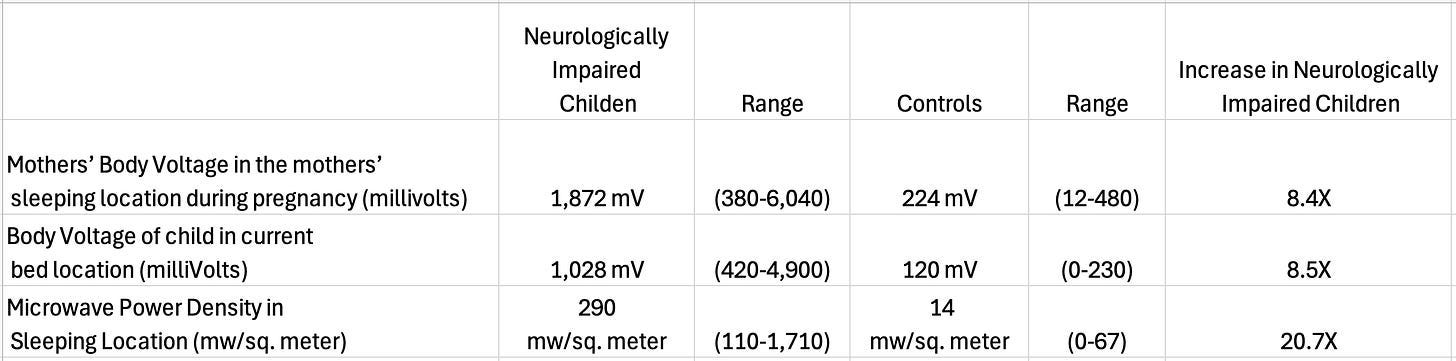
Note: Klinghart has also repeatedly highlighted a study conducted by Wolfgang Maes that found EMFs were 20 times stronger inside the womb than outside it. If this is true (I have not been able to find the study), it would confirm many ancient beliefs about pregnancy, and also suggest US is particularly dangerous to things within the womb.
Medical Imaging and Childbirth
Most imaging technologies (MRIs and radioactive tracers being the major exceptions) work by sending a wave of energy through the body and then assessing how that wave was altered when it comes out to determine what was passed through (e.g., bone absorbs more X-rays than fat and hence causes x-rays that pass through it to look distinctly different on a photographic plate).
During their medical training, each student is taught that every form of medical imaging has pros and cons (e.g., that a theoretical risk exists from x-rays), but that US is entirely safe and that its cons are due to the images it produces being dependent on the skill of the US operator (whereas other imaging modalities produce much more consistent results). Because of how those axioms frame the topic, it leads every medical student to unconsciously assume US must be 100% safe.
In turn, a significant aspect of the medicalization of childbirth has been assessing the fetus throughout the pregnancy (e.g., with medical imaging). Since minute things done to a fetus during gestation can become immensely consequential to them throughout the rest of their lives (e.g., consider the EMF example), it hence becomes critical to ensure those waves are indeed safe.
Unfortunately, this concept was not initially recognized by the medical field. After the benefits of routinely x-raying pregnant women (e.g., to know how the fetus’s position was changing) were presented at a 1923 conference and published in 1924, the practice became widely adopted.
Over the course of the next few decades, more and more concerns arose about the safety of this practice:
Murphy (1929 and 1931) reported an increased rate of severe abnormalities, including microcephaly and developmental delays, in neonates of women irradiated after conception compared with those irradiated prior to conception.
On the basis of animal studies, Russell and Russell (1952) concluded that the embryo is likely highly susceptible to developing malformations if exposed to radiation, even at low doses, particularly during the critical early development period from 4 to 8 weeks gestation. High doses could cause miscarriage.
By 1975, strong evidence had been compiled proving that radiation exposure during pregnancy causes miscarriage, leads to serious harmful effects to the fetus, including increased risk of leukemia and other malignancies, and alters the newborn sex ratio.
Despite these warnings (and many others), for decades x-rays continued to be used for a variety of routine obstetric assessments and treatments. It was only around 1975 that the obstetric field shifted away from the practice, in part due to the mounting evidence against it, but also largely because US had emerged as a viable prenatal imaging technology (which was arguably superior to X-rays since they could detect many potential birth defects and because the obstetrician could instantly do them in any setting and be reimbursed for their skill in performing the US).
Before we go further, I would like to review an important (forgotten) interview about US with Robert S. Mendelsohn, a courageous physician and one of the most influential dissident physicians in history (e.g., he paved the way for much of what people like me do now).
Note: one of the doctors Mendelsohn mentored shared with me that Mendelsohn told him that he decided to take the tough road of becoming a medical dissident during his appointment as Medical Director of Project Head Start’s Medical Consultation Service in 1968 after being horrified by the discussions held privately in the White House. They (e.g., with his medical colleagues) were openly discussing how they could control the population of the poor by promoting infant formula, vaccinations, sadistic hospital birthing practices, deficient government schools, and neighborhood abortion clinics—all of which was just too much of an assault on Mendelsohn’s strong Jewish faith and his Hippocratic oath.
“Safe” Levels of Ultrasound
Very few physicians know that for decades, there was extensive debate over the safety of US, particularly for children in the womb, especially early in gestation (e.g., in 1980, one leading researcher stated “the possibility of hazard should be kept under constant review”). Sadly, this 1979 quote encapsulates much of what followed:
Present day ultrasonic diagnostic machines use such small levels of energy that they would appear to be safe, but the possibility must never be lost sight of that there may be safety threshold levels possibly different for different tissues, and that with the development of more powerful and sophisticated apparatus these may yet be transgressed.
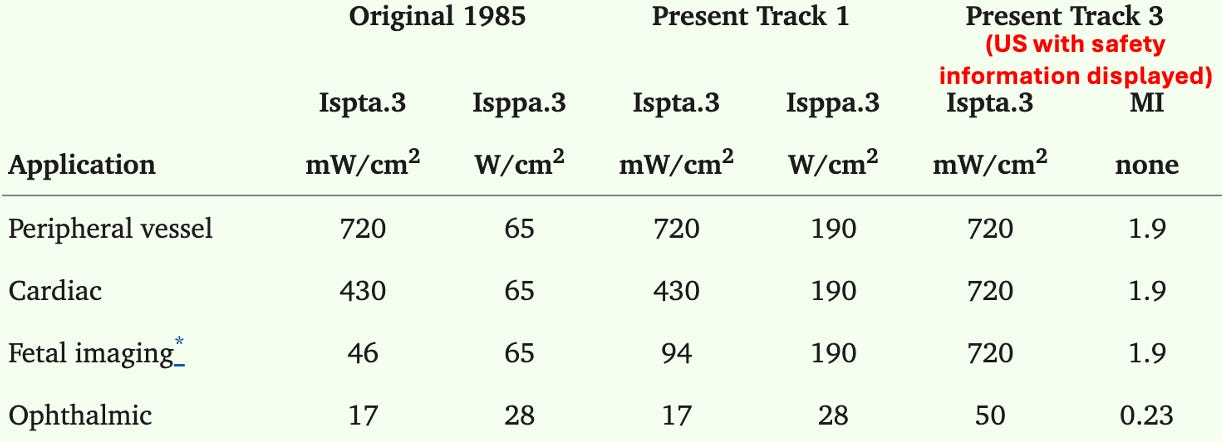
Much
of this amnesia was a result of the FDA in 1992, owing to divided
opinions over safety in the US field deciding to raise the maximum
allowable US strength from 94 mW/cm2 to 720 mW/cm2 so that higher quality imaging could be developed, at which point US effectively became “safe and effective.”
The rationale for this increase was two fold. First, the FDA wanted to have the standards be uniform (except for the eyes):
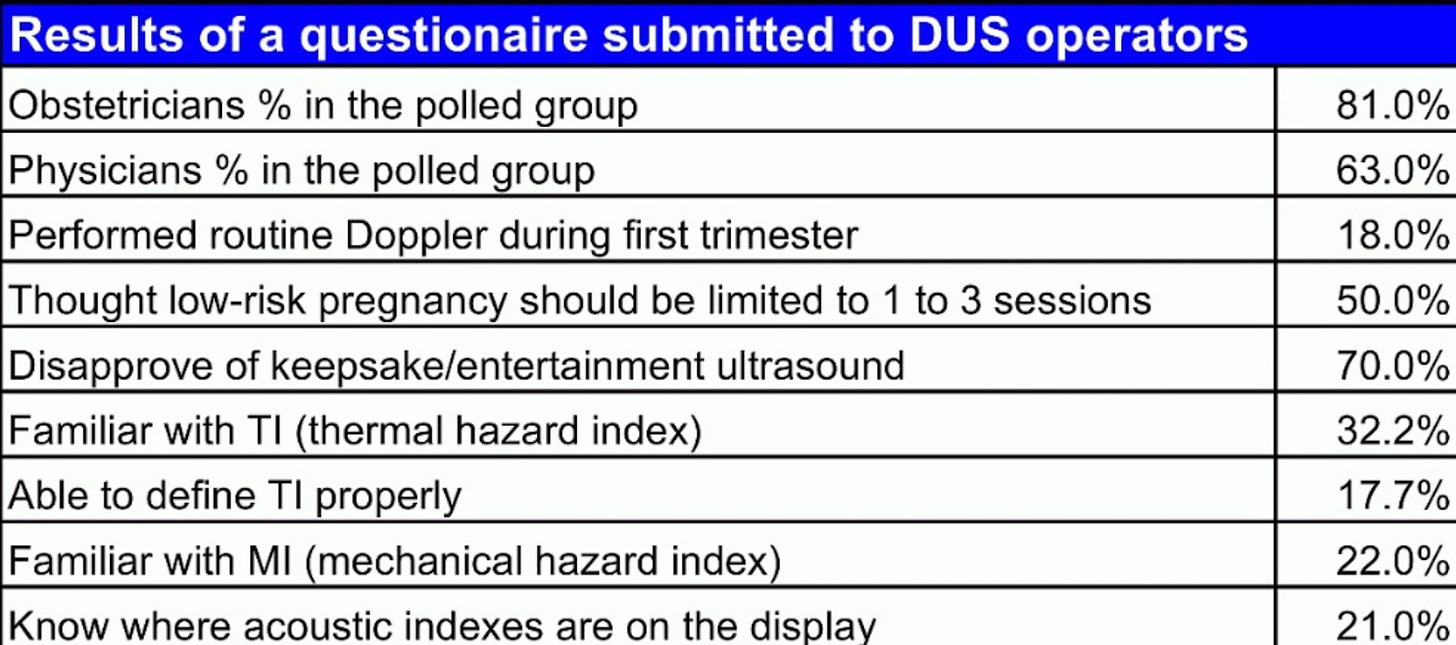
Second, they decided it was acceptable if the machines provided information on the current US strength so the operator could moment by moment decide if that risk justified the potential diagnostic benefit—which was absurd as almost no one was ever trained in the dangers of US (e.g., this 2007 survey highlights that lack of training):
Consider for a moment this forgotten 1993 CNN program on the dangers of the US and the fact it proved the FDA was fully aware that proven dangers of US existed, but had nonetheless chosen to raise the acceptable levels for it significantly.
Note: in contrast, Japan for example makes the limit for diagnostic ultrasound 10 mW/cm2.
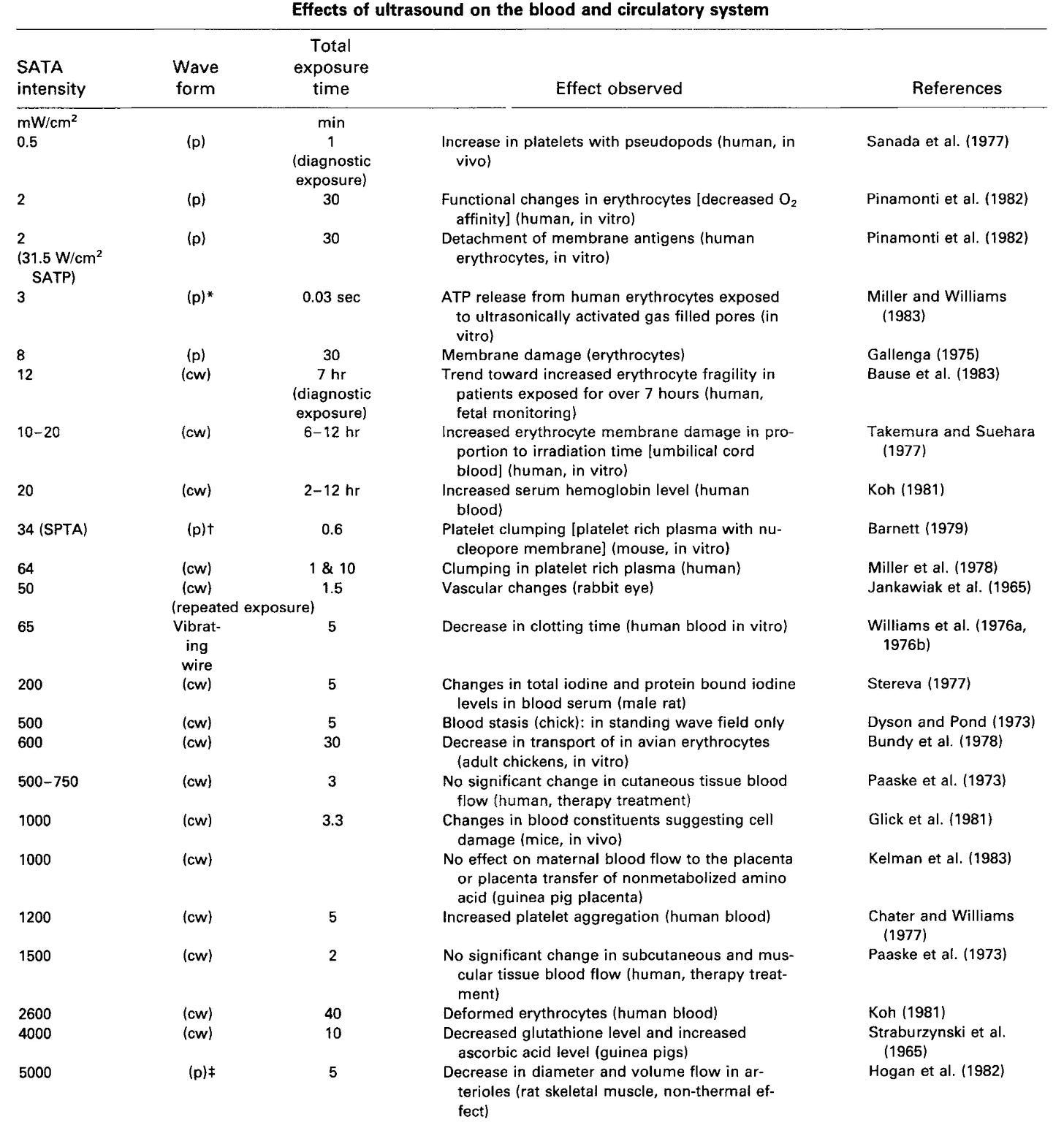
Most importantly, as we will show throughout this article, a large volume of literature already existed that showed:
•US had toxic biological effects.
•Those effects were dose dependent and started well below 94 mW/cm2
•All of the research (showing the dangers of US) had been conducted with far lower US intensities than the limit the FDA set.

It is unclear to me if the FDA raised the limit in 1991 or 1992, as sources argue for both (although 1992 is more commonly cited).
Furthermore, this 2011 review (which to my knowledge is the most comprehensive review that has been written on the harms of ultrasound) highlighted that there is some variability in both machine outputs and in how ultrasound strength is calculated (which can lead to stronger than permitted ultrasound emissions—e.g., due to machines underestimating the heat they generate), and that there are significant variations in the maximum strengths allowed. Additionally, the FDA does not consider the total time of ultrasound exposure when making these guidelines:

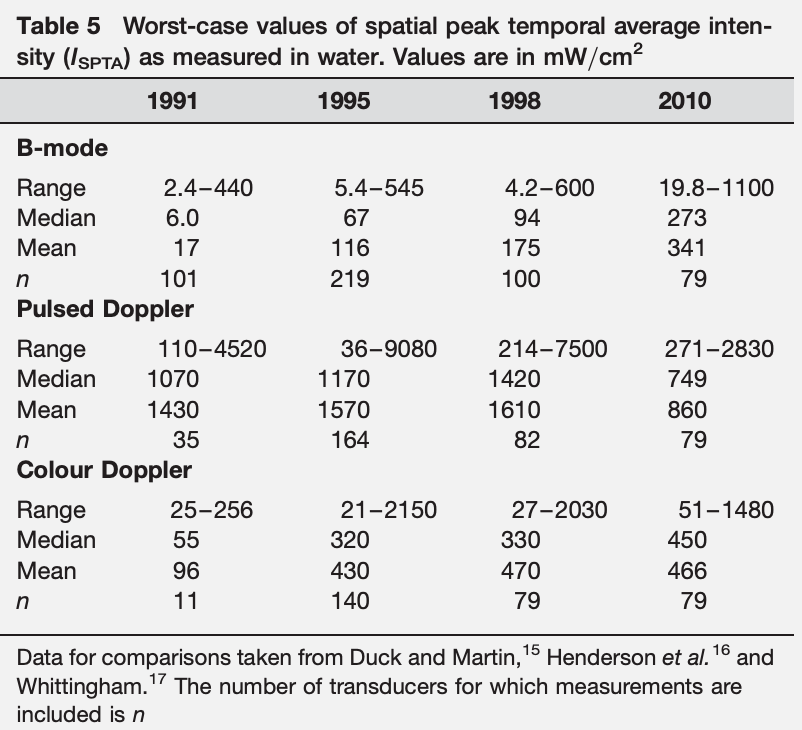
Similarly, consider this 2010 assessment of how high US values can go:
Note: the political push to make pregnant mothers hesitant to abort their babies by showing the pictures of the fetus in the womb (e.g., many states require this prior to abortion) also played a key role in the FDA’s acceptance of ultrasound widespread normalization of ultrasound (which I strongly suspect was a result of US industry lobbyists targeting pro-life legislators).
The Aftermath
Sadly, once the FDA declared US levels below 720 mW/cm2 were “safe and effective,” that quickly resulted in:
•The previous research on the dangers of US becoming forgotten.
•Medical societies gradually shifting their guidelines to increasingly downplay the dangers of US.
•A massive increase in the use of US (not unlike what happened after the 1986 Vaccine Act gave vaccines legal immunity).
•US
technicians not being trained in the dangers of US, and hence not being
mindful of how to avoid damage to the fetus. For example, the higher
intensity used in US, the “clearer” the image is, so technicians (who
were primarily assessed on their ability to get clearer images) will
frequently use much higher US intensities (or expose the fetus to
excessively long ultrasound sessions)—situations which would both be
avoided if they knew US was not “100% safe and effective.”
•Very lax oversight of the US output of commercially available US models, allowing many to have far higher outputs.
In recent decades, much of RFK Jr’s work has revolved around figuring out why our children have suddenly become significantly sicker. A key reason he founded the Children’s Health Defense was that the EPA had identified 1989 as the inflection point where this modern epidemic had started (particularly for autism). However, there is still no agreed upon explanation for why this shifted. In turn, many (myself included) believe that the primary culprit was Congress removing all liability from vaccine manufacturers in 1986, as this led to a rapid expansion of the vaccine schedule and eliminated any motivation to make those products safe.

However, this was not the only change that occurred. Beyond the 1992 ultrasound change, a similar argument could also be made that the proliferation of cellular phones (in the 1990s and early 2000s) or the use of glyphosate (which began in 1992 and greatly accelerated in 1996) are the actually responsible culprits. Similarly, some evidence links autism to US (e.g., a 2018 study found prenatal US increased the risk of children developing autism if they had a pre-existing genetic vulnerability).
In essence, we have a similar axiomatic trap to the situation with “non-ionizing” EMFs, which are assumed to be harmless despite large volumes of data showing otherwise. More remarkably, we’re told “non-ionizing” US cannot harm human tissues. Yet, many procedures exist (e.g., lithotripsy where high-powered US is used to break kidney stones apart, or high-intensity focused US, where targeted US is used by neurosurgeons to open the blood-brain barrier or to destroy brain tissue in a non-invasive manner) where it clearly is biologically active.
Consider this 1995 speech that was given to the British Royal Medical Society
The casual observer might be forgiven for wondering why the medical profession is now involved in the wholesale examination of pregnant patients with machines emanating vastly different powers of an energy which is not proven to be harmless to obtain information which is not proven to be of any clinical value by operators who are not certified as competent to perform examinations.
Fetal Reactivity
Because
vaccines are “safe and effective” healthcare workers assume the
negative reactions children have to vaccinations (e.g., uncontrollable
fevers and crying after an injection or becoming terrified of the
needles and anyone they associate with an injection) are baseless and
simply due to the children psyching themselves out (e.g., a common line
is “don’t worry, by the time he notices the needle was injected it will
already be out”).
As a result, one of the most
challenging parts of medical training (especially once I started
recognizing the more subtle signs of vaccine injuries such as the characteristic microstrokes they cause)
was having to repeatedly watch children be injured by vaccines while
simultaneously having every healthcare worker dismiss their concerns and
forcefully restrain the terrified child to administer the injections.
While I “got” this was the way things were, it just continually
astounded me (almost) that no one else could see this, and cemented
within me a deep conviction I needed to find a way to give a voice to
children who were being injured (as unlike adults who are vaccine
injured they could not effectively advocate from themselves).
One of the key things that made me suspicious of US was noticing that once US was applied, fetuses would react to it, and often seem as though they were trying to get away from it as the probe was directed towards them—which suggested, contrary to what we were told, US was not inert. Likewise, when I had (diagnostic) US applied to my own body, I noticed I could feel it and hear it (when it was applied to the head)—all of which again argued against it being silent and inert, especially since it did not feel “good” to me when it was applied to the heart.
After some digging I discovered:
•Most midwives (and a few physicians) I’d spoken to had made a similar observation to me and thought the babies withdrawing from US was a sign it could be dangerous.
•Scientific research showed that US caused increased fetal movement.
•A hydrophone inside the uterus determined that ultrasound registers at 100-120 decibels there (which is equivalent to a subway entering a train station).
Note: since many machines can emit ultrasound (which can adversely affect workers) OSHA limits the ultrasound workplace exposure to between 105-115 decibels. Likewise, a 1999 study
examined the white blood cells of workers exposed to ultrasound and
found that compared to those not exposed, their cells were more likely
to have developed micronuclei (a change associated with cancer).
•One researcher had identified a compelling anecdote of a two and a half year old child remembering their prenatal ultrasound:
Mikaela, remember the other day when you met Miss Laura and she asked you what it was like when you were in mommy’s belly?
Yeah?
Do you remember what you told her? I was up in the sky in the clouds.
You were up in the sky in the clouds? Uhm Hum
What was that like?I had to get out from the thunder. It was scary. And then the thunder went away.
And then the thunder went away?Yeah.
Fetal Demise
Early in my medical training, I saw a despondent mother in the emergency room having a miscarriage who kept saying, “I don’t understand what happened, we saw our gynecologist earlier today, she looked at my baby, and said he was in great health.” As the team counseled the mother, a simple thought kept running through my head, “Could the US have induced the miscarriage?”
Note: I was never able to verify if she had also received an influenza vaccination at her visit. As I showed here, numerous datasets show infants whose mothers are not vaccinated during pregnancy fair better than those who are. Additionally, it has been hypothesized that since US makes bacterial cells almost 100x more vulnerable to antibiotics (e.g., by breaking open biofilms), and other cells more vulnerable to certain cytotoxic drugs, it may synergistically enhance the toxicity of vaccines.
As I looked into this, I began to come across sporadic other reports of mothers (e.g., this one) with similar experiences:
As I will show throughout this article, (e.g., with this study, this study, this study, and this study) data supports the contention US can cause miscarriages or premature labor.
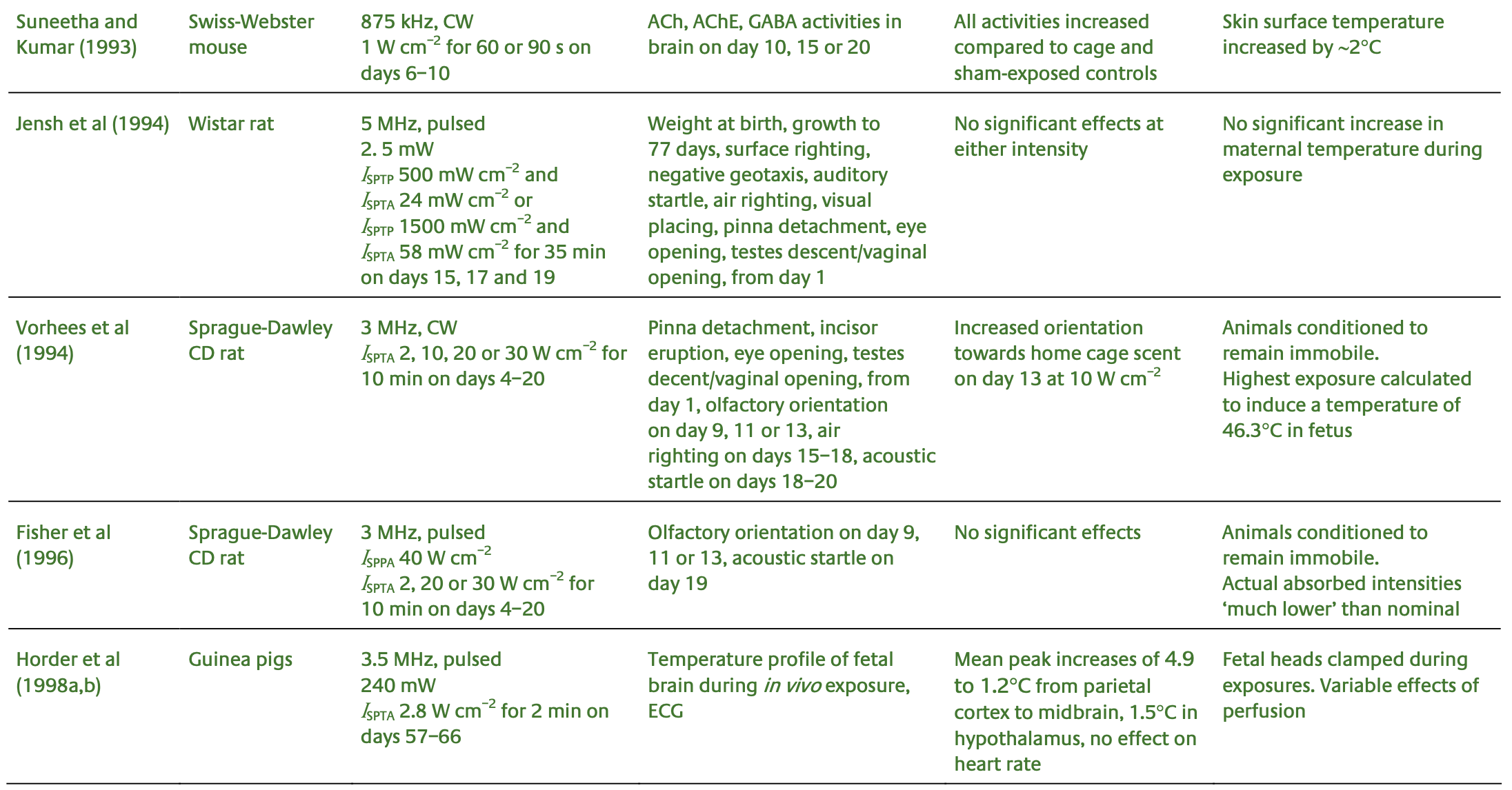
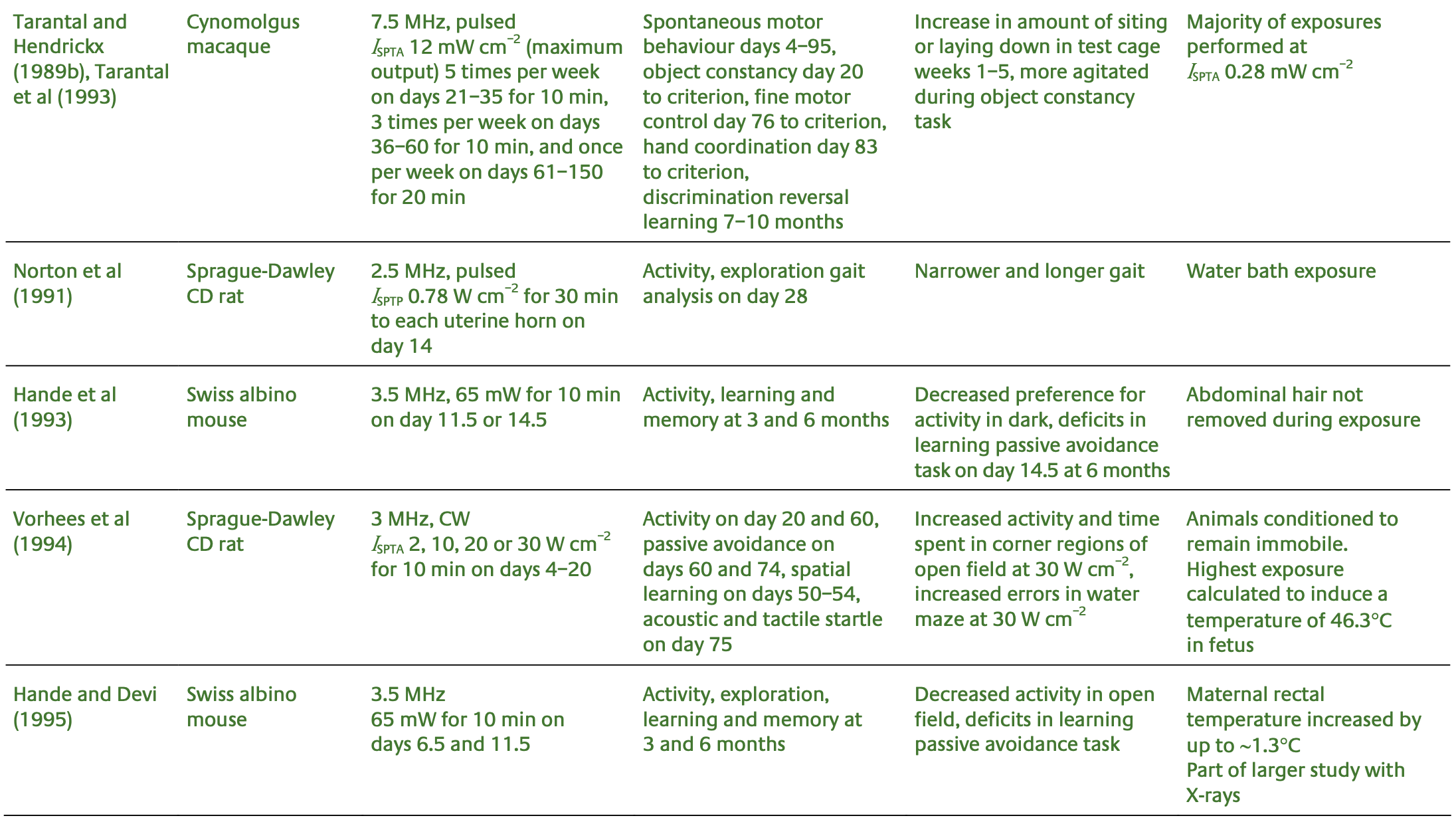
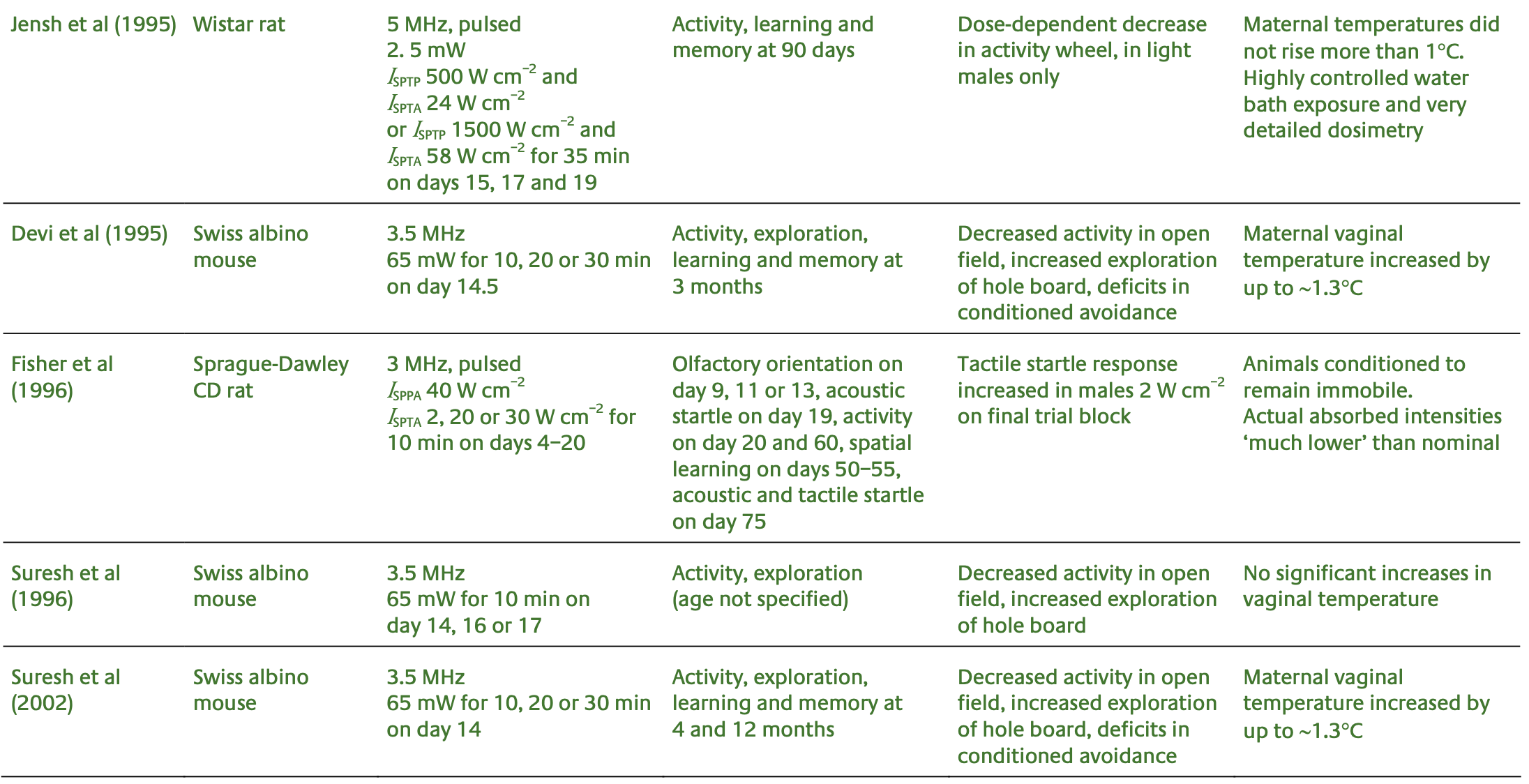
Research on Ultrasound Dangers
Over the decades, hundreds of studies have accumulated showing US and particularly prenatal US is dangerous. As some of you may have noticed, most of what I published over the last two weeks were revised versions of older articles, which was primarily because I felt it was important to track all of these studies down and accurately represent them (which was very time-consuming, especially with the Chinese ones).
The key points to take away from these papers is that there has been a continuous stream of research showing ultrasound is not safe, but each time a study came up which should have led to a global reevaluation of prenatal US, each was ignored. Instead, as the years went by, fewer and fewer studies were done (as it became impossible to get funding for them), and each group producing guidelines gradually relaxed all of their cautions on ultrasound.
Note: these US studies also show the same types of issues occurring in a wide range of tissues and species.
Animal and Plant Studies
A 1929 study found that US could cause the heart rate to accelerate, weaken the force of their contractions, and also cause other muscles to contract.
A 1949 study found US induced chromosomal and nuclear aberrations in daffodils. Likewise, this 1973 study found US (8.0 mW/cm2) created gross chromosomal abnormalities in fava beans.
A 1963 study found that giving hamsters US on the 6th or 9th day of gestation created gross abnormalities in the embryos or killed them.
A 1966 study of fruit flies concluded that US was more likely than X-rays to cause genetic mutations.
A 1972 study found that pulsed diagnostic ultrasound inhibited the growth rate in chick embryos.
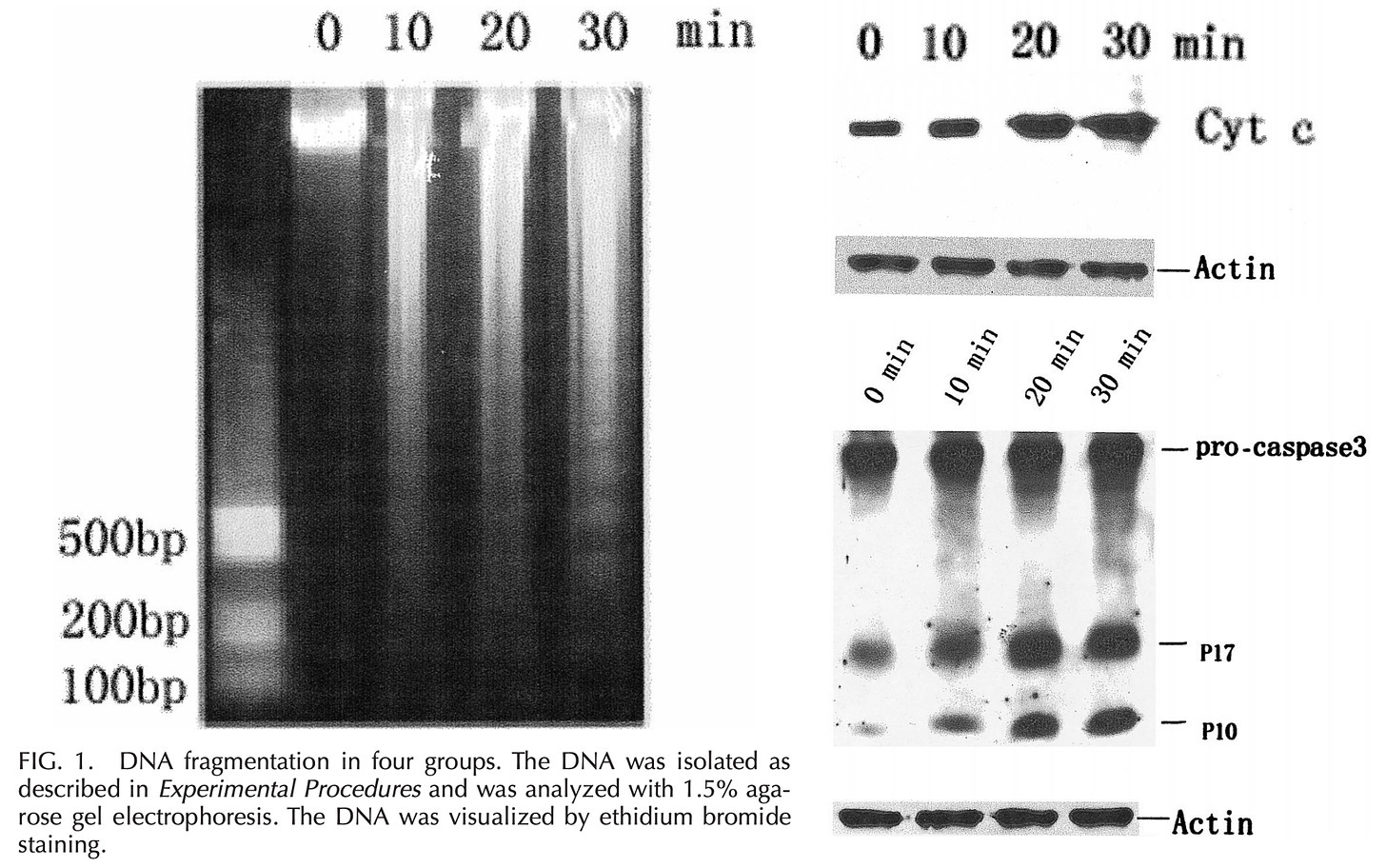
A 1975 study found that lower doses of US (20mW/cm2) for 30 minutes caused no damage to cell DNA, but at higher doses (200mW/cm2)
within 15 minutes caused very marked DNA fragmentation. What is
noteworthy about this study is that at the time it was conducted,
dramatically lower US doses (e.g., 20mW/cm2 ) were used than are used now.
Note: this 1973 study also detected genetic damage from ultrasound.
A 1978 study reported 1.5 mW/cm2 ultrasound when given for 2.5 minutes to rat embryos or for 5 minutes to fruit flies (in the larval and pupal stages), in some cases was lethal, in some cases inhibited growth, and in other cases produced no detectable effect, with the differences depending on what stage of development the embryo was at when exposed to US.
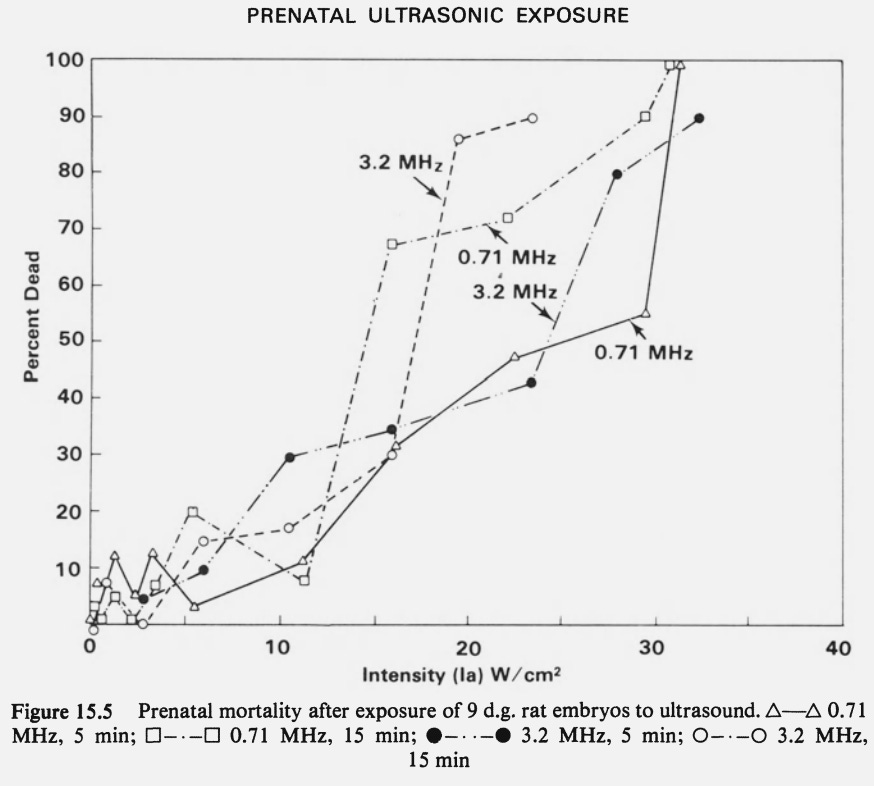
A 1979 publication reported that in rats, US induced fetal malformations and brain defects resembling those previously associated with x-rays (with issues being seen in the forebrain if the US occurred earlier in gestation).
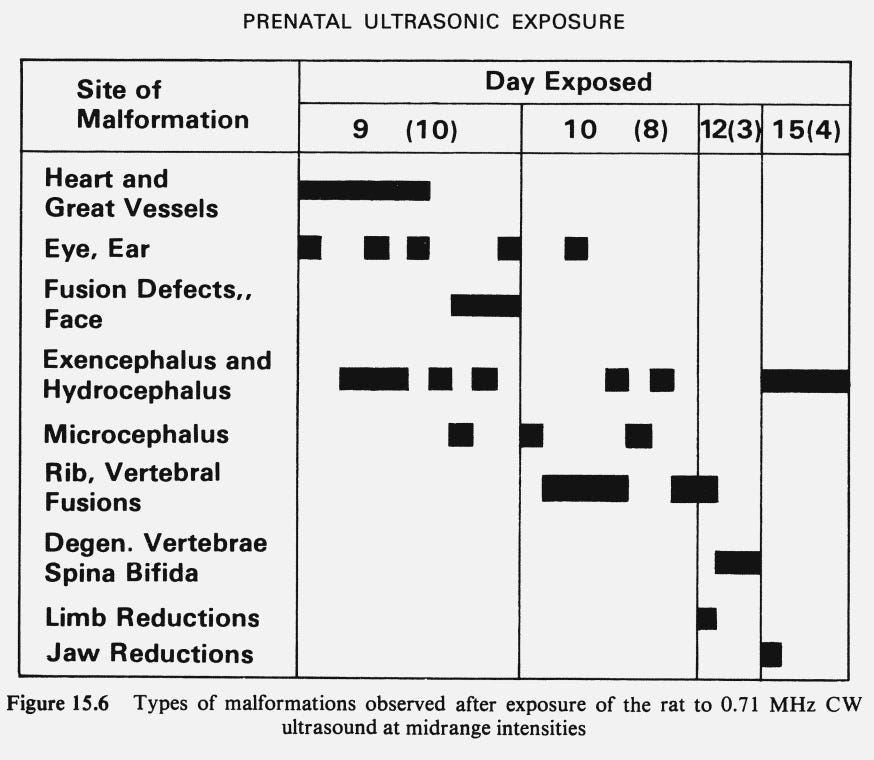
Additionally, they also that as the strength of the ultrasound increased, the rats were more likely to die, and that of the 89 that survived, 5 (5.7%) had significant developmental abnormalities (with the exception of one fetus with unilateral degeneration of the eye, the abnormal fetuses had multiple malformations including cleft lip and palate, a brain outside the skull, missing eyes, multiple anomalies of the face, unilateral absence of the kidney, and septal defect of the heart).
It also found that ultrasound could cause thinned ventricular walls (with enlargement of the lumen (the cavity inside each chamber) or thickened ventricular walls. Microscopic examination of these hearts demonstrated that the fibers were disarrayed in a number of areas, and there were focal areas of necrosis (tissue death), and that the incidence of fetuses with other cardiac abnormalities such as septal defects also increased at higher intensities.
Curiously, as this graph (and this study) show, the incidence of heart defects rose in tandem with the adoption of prenatal X-rays and then prenatal ultrasounds (particularly after the FDA allowed stronger ones to be used and most of the population began receiving them):
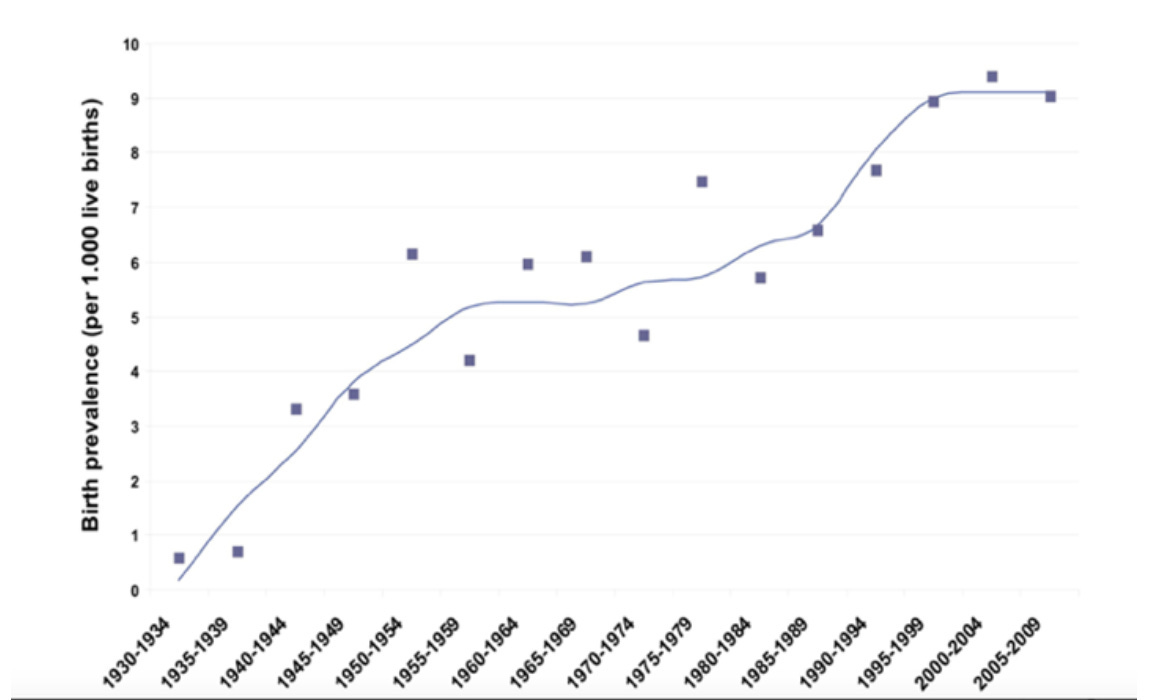
Note: one of the primary benefits of prenatal US is that it can identify a heart defect (which now affect almost 1% of pregnancies) and allow it to get surgical care either inside the womb or at the birth. Critical heart defects (which typically require surgery) currently affect 0.18% of births. Typically, prenatal US is able to identify about half of these defects, while a series of other measures (e.g., listening to a newborn’s heart or checking their blood oxygenation) typically identifies almost all of them. Overall, the one year survival for infants with critical heart defects improved from about 67% during 1979-1993 to about 83% during 1994-2005—a benefit which may in part have come from increased prenatal ultrasounds, but more likely was predominantly due to improved infant screening and surgical approaches. Based on all of this (e.g., US potentially causing heart defects), I am unsure how valuable prenatal US is in preventing death from a heart defect, and as I will discuss later, large studies show prenatal US does not improve the survival of infants.
A 1982 rat study showed US slowed the removal of colloidal particles from the blood.
A 1987 study found 0.135mW/cm2 US (which is fairly low) damaged the myelin of the dorsal nerve roots of rat pups. Sadly, this study, initially given a high quality rating by the NIH, was ignored and then denied funding for a follow up.
A 1993 monkey study
found that US transiently decreased white blood cell counts in
newborns. Additionally in this study, 2 of the 11 monkey fetuses exposed
to US spontaneously aborted.
Note: one of my friends and colleagues was the ultrasound technician for this study.
A 1995 study gave X-rays or US (240 mW/cm2) to mice at two points in their gestation. It was found that while X-rays adversely affected mice, the US was more harmful, and when given at both times, in addition to growth restriction, there was a higher perinatal mortality, at 3 and 6 months of age, there was a significant change in the locomotor activity with a reduction in the total activity, and a latency in learning (which means they were developmentally delayed).
A 1999 study found that US would induce hemorrhages in mice (of varying ages of gestation) near the bones, particularly the skull.
Note: there is currently a significant amount of evidence that standard ultrasound doses can cause lung hemorrhages in animals, but this has not been corroborated in humans.
A 2001 study found that 15 minutes of external US caused mouse intestinal cells to have a 22% reduction in the numbers of mitotic (dividing) figures 4.5 hours later, and the number of cells that were apoptotic (entering cell death) increased by 153-160% 1-4.5 hours post-treatment.
A 2006 study of 335 embryonic mice found that US for 30 minutes caused a small but statistically significant number of neurons to fail to acquire their proper position and remain scattered within inappropriate cortical layers or in the subjacent white matter. This increased with the duration of US exposure.
Note: following this compelling study, Nature (in 2010) reported that a $3,000,000 grant was given for a similar study in monkeys. Ultimately, nothing was heard about that study, which suggests its data demonstrated US was unsafe, which hence led to it being buried. This is analogous to how after 1991, only 4 Western studies (one in 2001, 2006, 2011, and 2012) assessed the dose-response relationship of modern ultrasound, or how studies showing the dangers of vaccination never get published (e.g., I recently published a widely seen thread on Twitter about a Yale COVID-19 vaccine study which is being blocked from publication).
A 2007 study found that pulsed US could cause hemorrhages in fetal rat bones exposed to it.
A 2012 study concluded that rat fetuses exposed to US suffered from bioeffects similar to X-ray exposure and had substantial alterations in gene expression (including those implicated in important developmental signaling pathways).
Cell Studies
As early as 1939, researchers knew that US could damage the chromosomes and DNA of cells (e.g., see this 1949 study which found this genetic damage was dose dependent and similar in character to what mustard gas or certain types of electromagnetic energy caused).
A 1970 study found significant chromosomal aberrations were observed when human blood cell cultures were exposed to an ultrasonic fetal heart detector for 1-2 hours (with its intensity not exceeding 30 mW/cm2).
A 1972 study reported that in human white blood cells, exposing them to US for an hour caused chromosomal aberrations once it was at least 8.2 mW/cm2 in strength and that it increased in a dose dependent manner (e.g., at 200 mW/cm2 it caused DNA shearing).
A 1979 study found exposing white blood cells to diagnostic strength US for 30 minutes caused an increase in sister chromatid exchanges (which meant DNA alterations were occurring). This 1981 study and this 1981 study had similar results, as did this 1984 study (which also found that the exchanges increased with increasing ultrasound strength).
A 1979 study found that 30 seconds of ultrasound significantly reduced cellular attachment (which is necessary to create tissue), especially in amniotic cells from a developing fetus.
A 1979 study found ultrasound exposure caused HeLa cells (another cell line commonly used in cancer research) to develop numerous signs of DNA damage and to cause 5 out of 6 mice injected with those cells to develop rapidly growing sarcomas at the injection site.
Note: DMSO has been shown to prevent apoptotic cellular death (or abnormal pathologies like fibrosis) from both radiation exposure and ultrasonic shock waves, and has also been found to cause cancerous cells to transform back to a non-cancerous state. Conversely, vitamin C (which can prevent the free radical DNA damage caused by x-rays and photo-oxidative damage—something DMSO also addresses) was unable to prevent ultrasound induced DNA damage.
A 1981 study exposed 3T3 cells (known for being susceptible to transforming into cancers in the presence of carcinogens) to X-rays and ultrasounds. It found in controls, a transformation frequency of 4.5*10-5 was observed, in those receiving 30 minutes of ultrasound, 82.5*10-5, in those receiving 300 rads of radiation, 210*10-5, and in those receiving both ultrasound and radiation 336*10-5. In a second experiment, controls were 6.5*10-5, ultrasound was 33.5*10-5, and x-rays alone were 108.1*10-5. Additionally, in the cells that did not transform, after 3 days, 66% were observed to develop abnormal microvilli, a figure that increased to 72% after 37 days. In short, the same mutagenesis caused by X-rays was caused by ultrasound, and this was worsened when both were combined.
Note: a 1987 study found that exposing cell free human amniotic fluid to ultrasound at 15 mW/cm2 created an equivalent amount of damage to what would be expected from 300 rads of radiation.
A 1981 study found 2.5-8mW/cm2 US damaged cell microtubules after 10 seconds of exposure.
A 1982 study that exposed 3T3 cells and normal rat peritoneal cells to US, found abnormal motility was detected 10 generations after exposure and that x-rays and UV light caused similar effects.
A 1984 study found low doses of US (0.6–1.0 W/cm2) caused small but consistent effects on the DNA of human lymphocytes.
A 2007 study showed US created free radicals and caused DNA damage.
A 2011 study
used low intensity US to eliminate nasopharyngeal carcinoma cells in
proportion to the total treatment time. In this study, it was observed
that after 12 seconds, damage to the nucleus and mitochondria was
observed (which initiated mitochondrial autophagy and cellular apoptosis
[death]), and that a change in mitochondrial morphology (e.g.,
swelling) alongside a collapse in mitochondrial membrane potential was
observed.
Note: these results alongside the fact that infant nervous systems appear to react to US suggest the possibility ultrasound can trigger the cell danger response.
A 2010 study exposed human hepatocarcinoma cells to US and found one minute of low intensity US (3.0 W/cm2) induced early apoptosis (cell death) in a significant number of the cells.
A 2017 study found that US can cause genome sized DNA breaks.
Human Pregnancy Studies
A 1990 RCT published in the Lancet gave 4691 women throughout Helsinki US at 16-20 weeks gestation and compared them to with 4619 who did not receive it. In the US group, there were 20 miscarriages and 11 elective abortions (due to diagnosed birth defects), whereas in the control groups, there were none of either. There was a subsequent 49.2% lower perinatal mortality death rate which was attributed primarily to infants with major malformations being aborted, and a high rate of twins being detected (US identified all whereas 36.7% were missed in those who were not examined with US). Additionally, after delivery, it was determined that there were 4 cases of placenta previa in each group, however, US detected 250 cases (meaning 246 were false positives)
Note: a major argument for US is that it can detect placenta previas (which affect roughly 1 in 200 pregnancies) prior to labor (as if they are observed in the cervix at the start of a vaginal labor, a transition to a c-section is then required). As this study shows however, this diagnosis is typically inaccurate (e.g., because the placenta will frequently move away from the opening of the uterus).
•A 1992 RCT
published in the Lancet took 2,600 pregnant women with singleton
pregnancies (no twins) and of the 2,475 women who delivered in hospital
after 20 weeks gestation, 1,246 received routine Doppler examinations
starting at 19-22 weeks gestation, and thereafter examinations were
monthly if the pregnancy was considered high risk (192) or once at 32
weeks if considered low risk (1054), while 1,229 controls did not. This
treatment increased the perinatal death rate by 2.4 times (17 vs. 7) and
increased the total pregnancy loss by 1.67 times (22 vs. 13). The US
group also had a 17% increase in emergency C-sections, a 48% increase in
Apgar scores <7 (a way to measure a baby’s health at birth) and a 6%
increase in the need for resuscitations at birth.
Note: Doppler USs are stronger than typical US but still are frequently used in pregnancy.
A 1993 RCT compared 1,415 women with singleton pregnancies who received US imaging and continuous-wave US Doppler flow studies at 18, 24, 28, 34, and 38 weeks gestation to 1,419 who only received a single US imaging at 18 weeks. Those who received the intense ultrasound regimen were 35% more likely to have an intrauterine growth restriction (being under the 10th percentile) and 65% more likely to have a low birth weight (under the 3rd percentile).
A 1998 US study
of 2,378 singleton pregnancies found only 58 of 183 (31.7%) growth
restricted babies were diagnosed before birth, whereas 45 were wrongly
diagnosed as being growth restricted (43.7% were false positives). Those
diagnosed as growth restricted were much more likely to be delivered by
a c-section (44.3% vs. 17.4%), five times as likely to have premature
deliveries (with the average pregnancy being 2-3 weeks shorter), and
their ICU admission rate was 2-3 times higher. The authors hence
concluded there was no benefit from this routine ultrasound screening.
Note:
a variety of issues exist for both the mother and child with C-sections
(something as this study shows, US significantly increases the
frequency of).
A 2012 study from a large healthcare database found that children of mothers who had US during pregnancy, 1.25% had a urologic disorder (e.g., a urinary obstruction), whereas only 0.66% of infants who did not get a prenatal ultrasound had that diagnosis. In the study, it was unclear how much of that increase was due to increased diagnoses made possible by ultrasound, and how much was due to US causing the urinary issue.
Developmental Delay
One of the major debates with prenatal US has been if it’s a contributing factor to the autism epidemic as the safe limits of US were raised around the same time the spike in autism happened. The only study I know that directly looked at this, in 2018, found prenatal ultrasounds increased the risk of children developing autism if they had a pre-existing genetic vulnerability. As mentioned before, in the same way US can enhance the potency of antibiotics, it may also make fetuses more vulnerable to vaccinations and hence increase the likelihood that vaccines (especially during pregnancy) will cause autism, but this has not been studied. However, there is significant evidence US can cause physical and cognitive developmental delay.
•A 1984 study found US was associated with a higher risk of dyslexia.
•A 1986 rat study found US exposure caused a variety of developmental defects (including many in the brain), which varied depending on when in gestation the US was applied.
•A 1993 study of 2428 pregnancies found US was associated with a 32% increase in not being right handed, while a 1998 study found a 33% increase, but only in boys, while a 2001 study of 6,858 men found US exposure in utero was associated with a 32% increase in left handedness.
Note: left handedness is one of the symptoms that has long been associated with childhood vaccine injuries (prior to ultrasound entering the market) and autism, disproportionately affecting men.
•A 1993 case control study evaluated 72 children who had been diagnosed with delayed speech of unknown cause. It found they were 2.8 times as likely to have received US in the uterus.
Note: one organization has been contacted by dozens of mothers who felt (sometimes massive) US exposure during pregnancy caused speech and other problems in their children.
•A 1996 RCT of 2743 women (who received either frequent ultrasounds or a single one at 18 weeks along with additional ones as indicated) found that the high ultrasound group children had reduced growth which was primarily within the skeletal system rather than the soft tissue.
A 2007 analysis of 13,212 children who received prenatal US found boys became 58% more likely to become schizophrenic and girls 26% (however this study had some potential confounders).
Finally, a 2008 analysis of 2482 children who received US in the womb (11–35 mW/cm2) found that boys who received prenatal US later had lower physical education scores, were 17% more likely to have poor school performance and 35% more likely to not qualify for secondary school.
Note: studies also found that US caused baby monkeys to sit or lie around at the bottom of their cages rather than conducting typical behaviors (e.g., climbing up the bars of their cages).
Lastly, in conjunction with stronger US being permitted, there has also been a significant drop in the average birth weight and length of pregnancy. To quote the Washington Post:
Babies born in the United States weigh less than they used to, with the average birth weight dropping 2.4 ounces (0.15 pounds) — from 7.31 pounds to 7.16 pounds — from 1990 to 2013, according to a new analysis using data from more than 23 million births. In that time, births were also less likely to occur after the 40th week of pregnancy, often considered the official due date (18 percent in 2013 vs. 29 percent in 1990) and more likely to occur in weeks 37 to 39 (49 percent in 2013 vs. 38 percent in 1990). Researchers attributed the drop in birth weight primarily to shorter pregnancies and earlier births because of increased scheduling of Caesarean sections and induced labor before week 40. The percentage of births by C-section grew from 25 percent in 1990 to 31 percent in 2013, and deliveries that involved induced labor went from 12 percent to 29 percent.
Note: another thing which made us suspicious of US was that we’d periodically come across cases of parents who continually used US throughout their pregnancy to monitor their developing child (e.g., Tom Cruise attracted national controversy in 2005 for getting a home US unit to do this), and gradually noticed that those babies tended to be more sickly.
Nerve, Eye, Ovary and Testicle Damage
•Numerous studies (the first in 1938), have shown that ultrasound can cause a variety of injuries to the eyes and prolonged exposures can create cataracts.
•A 1951 study found using 35 W/cm2 US on the lumbar plexus at room temperature caused hind limb paralysis was observed at room temperature after a 4.3 seconds, and at near freezing, instead took 7.3 seconds. Additionally, a microscopic analysis showed neuronal and myelin destruction in the spinal cord, and axonal degeneration, chromatolysis, pyknosis with intact mesenchymal structures, and clumping of myelin in the peripheral nerves and cauda equina.
A 1958 study found that US to the lumbar spine caused immediate motor impairment in the hind legs, and that within 10-15 minutes, lesions could be found within the spinal cord.
A 1980 study found high doses of whole body US (1 W/cm2) given to pregnant rats after 80-200 seconds resulted in hind-leg dysfunction and a distended bladder syndrome (which was often associated with flaccid large intestine and compacted fecal material).
A 1982 study found that applying US to the ovaries during the late follicular phase triggered premature ovulation in 5 out of 23 women and then 8 out of 19 women.
A 2006 study inadvertently found that applying 700 mW/cm2 ultrasound to the brain opened the blood brain barrier and caused a contrast agent to leak into the frontoparietal area. A 2017 study used this property to direct chemotherapy agents into the brain.
Note: many other studies like this 2014 one have also explored ultrasounds’s ability to open the blood brain barries.
US (at high doses) has also been shown to damage the testicles, while at lower doses to decrease both the sperm count and sperm motility It has been tested in monkeys as a contraceptive and in a more limited setting in humans (discussed in this review paper). About ten years ago, ultrasounding the testicles was viewed as a promising male contraceptive and as a non-invasive way to conduct vasectomies but it ultimately never reached mainstream use.
Note:
the two tissues in the body which have been shown to be the most
vulnerable to microwaves are the testicles and the heart. As such, some men find they are only able to have a child once they stop carrying a cell phone in their pocket.
Workplace Exposures
•A 1990 case-control study evaluated all physical therapists who had been pregnant in Finland between 1973-1983. It found those who used US at work were more likely to have spontaneous abortions, with a 10% increase being seen in those who did it 1-9 hours a week, a 20% increase seen in those who did it 10-19 hours a week, and a 240% increase seen in those who did it over 20 hours a week.
•A 2000 study of medical personnel working in a cardiology unit who regularly gave Doppler ultrasounds had consistent increases in chromosomal abnormalities of their white blood cells.
Note: while ultrasound safety research has largely stopped, this Israeli researcher has published a few more recent studies.
The China Studies
Note: a significant portion of this article (e.g., the charts), in particular this section, came from Jim West, a journalist who put a great deal of work into this subject (and has written detailed books and an extensive article on it). While the research in this section is quite compelling, given its nature, it will likely be quite difficult for many of you to read.
Due to an unusual confluence of historical and cultural factors (e.g., a 1984 state plan), in the late 1980s, China, was eager to utilize its newfound scientific apparatus (which, unlike now, had not yet been captured by conflicts of interest). In turn, a series of studies were conducted that would never be done in the West, which provided the definitive proof US is not safe during pregnancy.
Essentially, they took large numbers of women planning to have abortions (which due to the One Child policy—a tragic period I wrote much more about here—were frequently done to both willing and unwilling mothers), gave US to half of them, and then dissected the aborted fetuses to assess if US had damaged them. To quote one of the lead investigators:
In view of the favorable conditions of China's basic national policy of family planning, Gong Yan and others from Xi'an Medical University took the lead in completing the first clinical study in China.
In my eyes, it is tragic both that these studies happened and that this knowledge has been completely forgotten. As you read these, it’s important to keep in mind that they used dramatically lower US doses than what the FDA now permits.
Overviews
Starting in 1986, professor Rou Feng began publishing studies raising concerns about the urgency of determining the safety of US in pregnancy.
In 1998 Rou Feng published a paper (which can be read here) that highlights the dangers of US (e.g., heat damage, cavitations, sound pressure, acoustic radiation forces):
This issue has become very important and eye-catching since the 1980s. One of the backgrounds is the rapid expansion of the application scope of diagnostic ultrasound in obstetrics and the other is that the transient sound intensity output by diagnostic ultrasound equipment may sometimes be as high as 1000w/cm2 or more. Such high sound intensity is enough to produce cavitation in organisms containing cavitation nuclei.
Once cavitation occurs, as Professor Carstensen pointed out: "... the effect caused by cavitation may be very local, damaging only a few cells around it. For most organs or biological fluids in the human body, damaging a small number of cells will not affect health , but the only exception is when it involves human reproductive cells. Or embryos or fetuses in a sensitive period of development, in this case, even if a few cells are damaged, the public will find the consequences of this unacceptable.Internationally, research on the safety threshold dose of diagnostic ultrasound is mainly carried out through two channels: experimental animals and epidemiological research. The research is extensive, sometimes even cross-border, and a lot of research data has been accumulated. A small number of quantitative laws have also been summarized, but at best it can only serve as a reference for clinical safety diagnosis, and it is impossible to provide specific guidance standards.
To be precise, establishing the safety threshold dose standard for diagnostic ultrasound should be based on a large number of scientific studies on obstetric clinical ultrasound diagnosis, which is a gap in international research. This is a major shortcoming!
Note: Rou Feng has also published studies (e.g., this one) about high powered US being used to eliminate tissue (e.g., uterine lining) that can be viewed in English databases.
This 2001 review paper provides a detailed overview of the harms of prenatal US and includes a focus on the appropriate dosing of ultrasound.
This 2005 review paper identified 130 English and 35 Chinese articles published between January 1998 to January 2004 on US and apoptosis (cell death). Collectively they showed US had dose dependent biological effects such as inducing apoptosis and that there was inadequate research to ensure its safety for humans.
This 2010 review paper
focuses on the biological effects of pregnancy US in humans and animals
(e.g., changes and injuries to organs, tissues, cellular
ultrastructures, and cytokines), highlighting a dose-response
relationship, the sensitivity of tissues and cells to US, and that both
acute reversible and irreversible apoptotic processes are initiated by
US.
Note: apoptosis describes the programmed death
processes many cells go through after facing hostile environments or
signals from the body, while apoptotic proteins denote those that
facilitate the process.
Chorionic Villus
Note: the chorionic villi are projections from the placenta that contain the same genetic material as the fetus, and hence are frequently sampled to get the fetus’s genetic information without gouging out part of the developing baby. In theory, this represents the best way to evaluate the effects of US on fetuses, as those cells can be obtained and dissected without aborting the baby. However, in some of these chorionic villi studies, it specified an abortion was performed shortly after.
A 1992 study of 55 early pregnant women US found that 20 minutes or more of US caused lipid peroxidation, increased malondialdehyde levels and decreased glutathione peroxidase levels, and that these changes were dose dependent.
A 1992 study of 15 healthy women at 6 to 8 weeks of gestation found that US caused pyknosis (shrinkage), disintegration, and increased vacuolization of the syntrophoblast (ST) cells and necrosis in part of the villi (with slight changes being observed after 10 minutes and significant ones after 30 minutes).
A 1994 study (which is in Pubmed) found that US for 5, 10, or 30 minutes (at 6-8 weeks of gestation) caused cellular changes including hyperreaction of lipid peroxides; increased activities of some lysosomal enzymes; reduced SOD activity; and vesiculation and aberration of some mitochondrion, also transformation or disappearance of some microvilli in ultrastructure, and that these effects were increased with US exposure time.
A 1995 study of 9 early pregnancy women found 10 but not 5 minutes of transvaginal US caused breaking, loss and disorganization of the microvilli and expansion of rough endoplasmic reticulum.
A 1995 study
of 40 embryos (with the US in B-mode) found that at 5 minutes of US
caused subtle changes, whereas at 10, 20 and then 30 minutes, increasing
cellular damage was seen (e.g., swelling, degenerating and necrotic
cells). The authors concluded that US should ideally be limited to 1
minute or less.
Note: the authors also advocated for
mothers to have a full bladder during the procedure as this increases
the distance between the mother and the fetus and that multiple US examinations should be avoided if at all possible.
A 1995 study gave US to 27 healthy women at 40-60 days gestation who received 0-15 minutes of US and then evaluated the villus 7 days later. It found 10 but not 5 minutes of US, in a dose dependent manner, caused injury and deformation of the plasma membrane, the deformation, shrinkage and breaking of microvilli, shrinking or swelling of components of the cells, and focal necrosis or karyolysis. It also found that broad bandwidth US was more damaging than single frequency US and that US was less damaging later in pregnancy.
A 1996 study (which is in Pubmed) found that after 30 minutes, compared to controls, 0.7mW/cm2 of either B-mode or color Doppler US caused expansion of perinuclear space in cytotrophoblasts [CTs] and [STs], enlargement of rough endoplasmic reticulum, and vacuolization in the cytoplasm.
A 1998 study gave 125 early pregnancy women 0, 10, 20 or 30 minutes of US and then analyzed the CV 7-10 days later. At 20 minutes, malondialdehyde (a reactive molecule that damages cells) was increased and GSH px (an enzyme that protects cells from oxidants) was decreased, while at 30 minutes, DNA content was decreased. After 7-10 days, these figures normalized.
A 1999 study (which can also be viewed on PubMed) gave 80 women, no US, 10 minutes of US through the abdomen, 3 minutes of US through the vagina, or 10 minutes through the vagina (a stronger route of fetal US exposure). An hour later, embryo villi were obtained through abortions and 10 minutes of transvaginal ultrasound was found to cause the microvilli to become broken, lost, and disarranged, and the rough endoplasmic reticulum of trophoblasts became expanded. Additionally, their malondialdehyde levels increased and the superoxide dismutase (SOD) decreased.
A 2001 study found US decreased the activity of SOD (a key antioxidant enzyme of the body).
A 2001 study
exposed 24 first trimester women to varying amounts of Doppler US then
after 24 hours, their trophoblasts were removed and analyzed for their
rates of apoptosis. In controls, the apoptotic rate was 44.56% [±13.24]
in the syncytiotrophoblasts (STs) and [43.14] ± 11.76, in 20 minutes in
the cytotrophoblasts (CTs) while after 30 minutes, 59.64% [±11.85] in
the STs and 61.43% [±10.13] in the CTs.
Note: no increase
from controls was observed in the 10 minute US group, but an increase
was observed in the 20 minute group (which was greater in the 30 minute
one).
A 2001 study found US significantly lowered nitric oxide (an important molecule for health) and the enyzme that synthesizes it.
A 2001 study used electron microscopy and flow cytometry to assess how US induced apoptosis. Control cells had spheroid nucleus with unstained and dispersed chromatin and abundant cytoplasm. US caused the nucleus to shrink, for patches of condensed chromatin to line the nuclear membrane, and in time the nuclear membrane to become stuck to the nucleus causing it to clump (and also increased the ratio of apoptotic cells).
A 2002 study exposed 24 first trimester women to varying amounts of Doppler US, then after 24 hours, their trophoblasts were removed and analyzed for their Fas/FasL mRNA expression (a receptor that triggers the cell death process). In controls (0 minutes US), there was a 58% [±5] rate of Fas expression in the STs and 52% [±5] in the CTs and for FasL, 63% [±6] in the STs and 62% [±12] in the CTs. No significant difference was seen with 10 minutes of US, however, a significant increase was seen with 20 minutes (e.g., FasL expression reached 74% [±10] in the STs and 72% [±12] CTs) and at 30 minutes (e.g., Fas expression reached 70% [±6] in the STs and 65% [±9] CTs).
A 2002 study of 15 women at 6-8 weeks gestation found that 20 but not 10 minutes (or less) of US caused enlargement of endoplasmic reticulum and mitochondrial intracristal space in syntrophoblast cells.
A 2002 study (which is in PubMed) found that 20 minutes but not 10 minutes of 13mW/cm2 transvaginal US in 4 hours activated caspase-3 (which induces apoptosis), released cytochrome C from the mitochondria (indicating mitochondrial damage) and fragmented DNA.
A 2005 study gave US to 24 first trimester women and found that 10 minutes created no changes in Capase 3 and 8 protein expression, but after 20 minutes (and 30 minutes) both apoptotic proteins increased.
A 2006 study of 66 early pregnant women found that 5 minutes or more of transabdominal US significantly increased the expression of mRNA for Caspase-3 (which plays a key role in apoptosis). Additionally, the authors suspected a smaller amount of time with transvaginal US could trigger these changes.
A 2006 study exposed 27 healthy pregnant women (at 40-60 days gestation) to either 0, 5, 10 or 15 minutes of US, and found that those who’d received 10 or more minutes of US had varying degrees of dose-dependent damage the syntrophoblast and trophoblast cells such as injury and deformation of the plasma membrane, shrinking or swelling of the cell, focal necrosis, and karyolysis. Additionally, they found that broad bandwidth US caused more damage, and that this damage decreased evidently after 7 days.
A 2006 study of 10 first trimester women transvaginal US, and found that compared to 5 controls (who rarely underwent apoptosis—something also observed in many of the other studies I’ve listed), it caused apoptosis in a dose dependent manner which gradually returned to normal after 72 hours.
A 2006 study of 35 early pregnancy women found that at least 15 but not 5 minutes of transabdominal US caused immediate and significant cellular damage, and that at least 10 minutes of US caused increased RNA expression for Caspase-3 (an apoptotic protein) and Livin-α (a protein that is overexpressed in many cancers).
A 2008 first trimester study found that US caused apotosis in a dose dependent manner for 72 hours after US that was not present in controls.
A 2008 study gave transvaginal US to 60 healthy first trimester women. It found that 3 minutes decreased the expression of Bcl-2 (a protein that prevents apoptosis), at least 5 minutes (but not 3), when assessed 24 hours later, caused apoptosis of chorionic villi, and that 10 minutes further increased the apoptosis and also increased the expression of Bax (another protein that facilitates apoptosis). Like many other of these studies, it emphasized that caution should be given with pregnancy and US, that the probe should not be held in the same position for a prolonged period and that US should be under 3 minutes in total.
A 2009 study gave US to 65 first-trimester women, and then assessed their chorionic villi TNF-α and p55 TNF receptor expression 24 hours later (they are key mediators of inflammation and apoptosis). In controls, they were 54.26% [±6.48] and 61.56% [±9.23] respectively, after 10 minutes, 55.54% [±2.82] and 62.75% [±11.84], after 20 minutes 61.94% [±6.34] and 67.38% [±8.77], after 30 minutes 65.39% [±5.96] and 74.63% [±7.38].
A 2010 study of 50 pregnant women found that approximately 10 minutes of transvaginal US caused cellular damage to the villi, whereas 5 minutes of exposure resulted in it being “basically normal.”
Brain
A 1998 study (archive link)
of 28 pregnant women found 30 minutes but not 10 minutes of US caused
the fetal pituitary gland to have paravessel tissue edema, the space
between the cells there to increase, its cells to have rarefaction of
their nuclear chromosomes, and its mitochondria to vacuolize.
Note:
we suspect widespread pituitary gland dysfunction (possibly due to US
or vaccine induced microstrokes) is a key culprit in the obesity and
diabetes epidemic.
A 2002 study of 8 women at 18-25 weeks (4 of whom were controls) gave 4 of them 10 minutes of 124.1mW/cm2 B-mode US (directed at the fetus’s brain) 30 minutes prior to abortion. Compared to controls, this caused the brain’s neurons to have irregularly distributed chromatins (which became condensed or marginated), depleted glycogen (few particles were in cytoplasm), frequent secondary lysosomes, and some of the mitochondria to be swollen slightly or even vacuolated.
A 2005 study of 10 pregnant women (at 18-25 weeks gestation) found giving 10 minutes of B-mode US 30 minutes prior to abortion harmed the brain’s glial cells. Specifically, glial cell membranes, subcellular organelles such as mitochondria, Golgi complex, and endoplasmic reticulum appeared damaged, the perinuclear space was widened, chromatins were distributed irregularly, markedly condensed, and agglomerated (which is a characteristic of apoptosis).
Eyes
A 1997 study of 80 pregnant women found that 5 minutes of US resulted in local edema of the fetus’s cornea and after 20 minutes (but not 10 minutes), resulted in the antioxidant activity (SOD and GSH-Px) of the villous cells decreasing
A 2001 study of 90 pregnant women (with controls) found that 3 minutes of US caused local edema of the fetal cornea and after for 20 mins resulted in corneal SDH (a mitochondrial enzyme) values decreasing.
Immune Function
A 1994 study found that giving women of any trimester US (at 7.6mW/cm2) for 30 minutes resulted in the newborns red blood cell C3b receptors being decreased and the formation red blood cells rosette immune complexes was increased.
Kidney
A 2002 study found that exposing second trimester fetuses to 10 minutes of US immediately prior to abortion did not affect the kidneys. However, 30 minutes of US resulted in the kidneys (48 hours later) caused an irregular distribution of nuclear chromosomes of the cells of the renal glomerulus and renal tubule, the mitochondria to swell and expand, the mitochondrial crest to disappear and vacuolated and the rough endoplasm reticulum to slightly expand.
Liver
A 2004 study (archive link) of 36 women near the middle of their pregnancy gave US 48 hours prior to abortion. It found 30 minutes of US but not 10 minutes caused the liver mitochondria to swell and have blurred cristae.
Reproductive Organs
A 1996 study
of 36 pregnant mothers (at 20-28 weeks gestation) found 30 minutes but
not 10 minutes of US caused the cells of the testicles that produce
sperm (the spermatogonia) to become swollen, have a rarefaction of
nuclear chromosomes and to have damaged mitochondria.
Note: identical results were obtained from another 1995 study.
A 1997 study of approximately 70 aborted fetuses at 16-28 weeks gestation found that 30 minutes but not 10 minutes of US harmed their ovaries. Specifically, the eggs became swollen with rarefaction of the nuclear chromosome and the mitochondria became swollen, vacuolized and their cristae disappeared.
Lastly, in addition to these studies, I also identified 24 other Chinese publications demonstrating the dangers of US during pregnancy (which are listed here). These include 8 review papers, 2 on US triggering mutagenesis, 8 on its effect on the chorionic villus, 2 on its effects on the eyes, 2 on the immune system (one for the decidua, and one for the neonate shortly after birth), and 2 on the testicles. Since I could not provide a link to them, I did not list them here, but if anyone can, that would be greatly appreciated, and they will be added to this article.
Ultrasound Reviews
Note: as there are so many studies highlighting the dangers of US, to make this article shorter, I am quoting significant portions of two large reports which compiled many of those other studies. It should be noted that none of these reviews were aware of the Chinese Studies.
In 1973, Thacker warned about the potential genetic hazard of US.
A 1980 review highlighted the known dose dependent adverse effects of US and concluded that there was still not enough data to know what constituted the correct US dose.
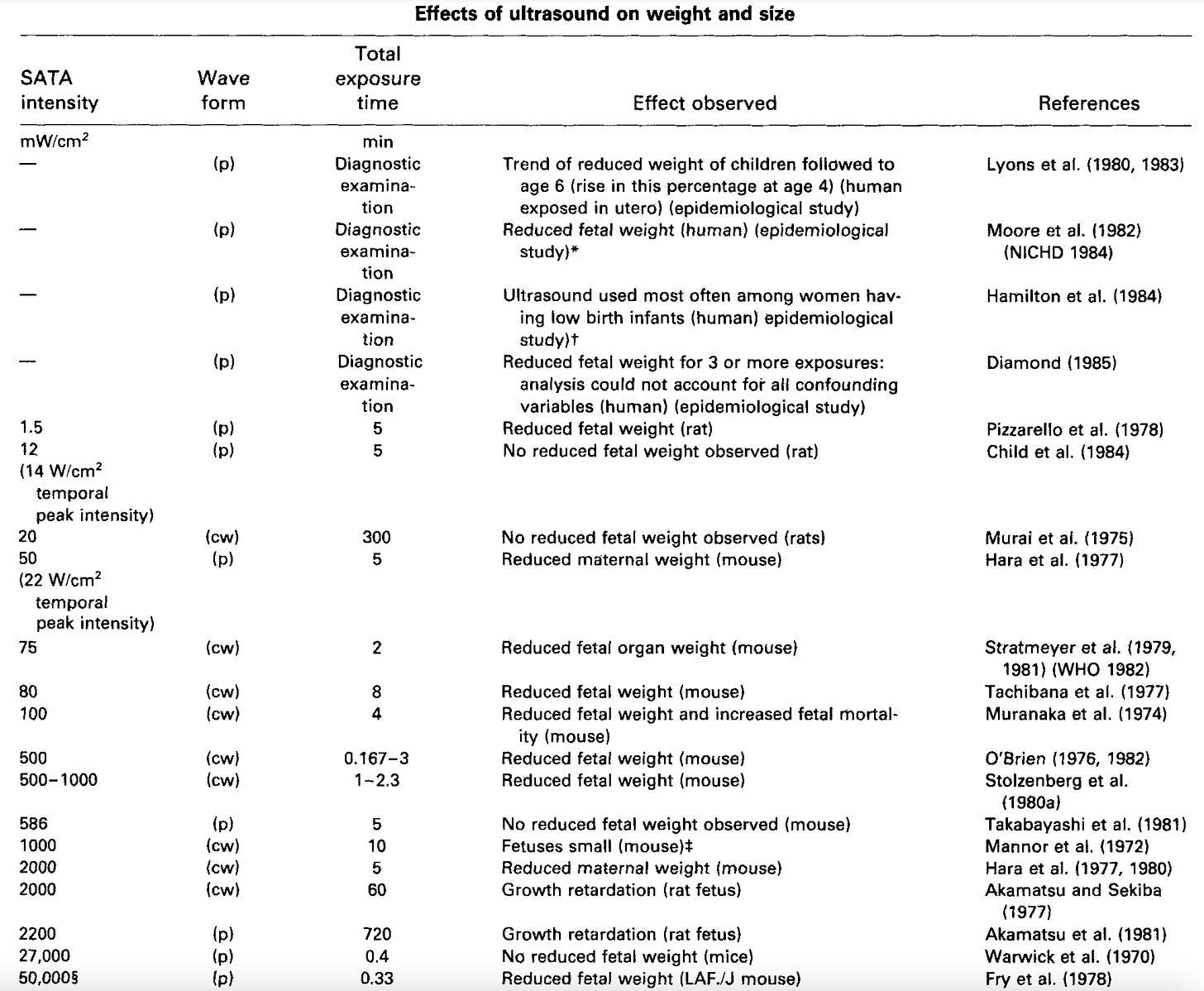
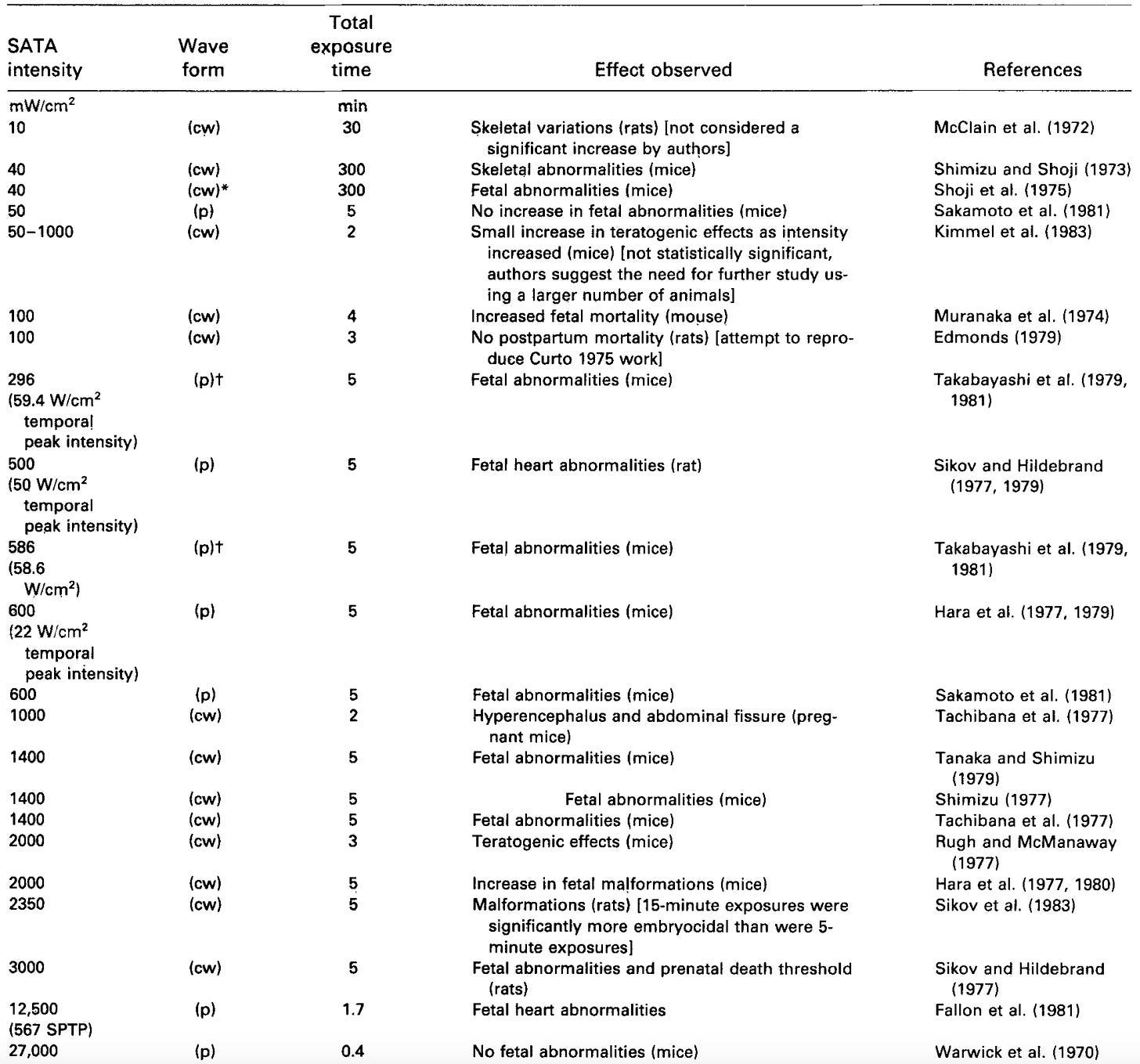
A 1985 review on the harms of US identified numerous studies that demonstrated that US caused a wide range of abnormalities and that they became more frequent as they increased in intensity. These changes included:
Significant changes to embryos (e.g., disruptions of embryogenesis, malformations, and impaired growth).
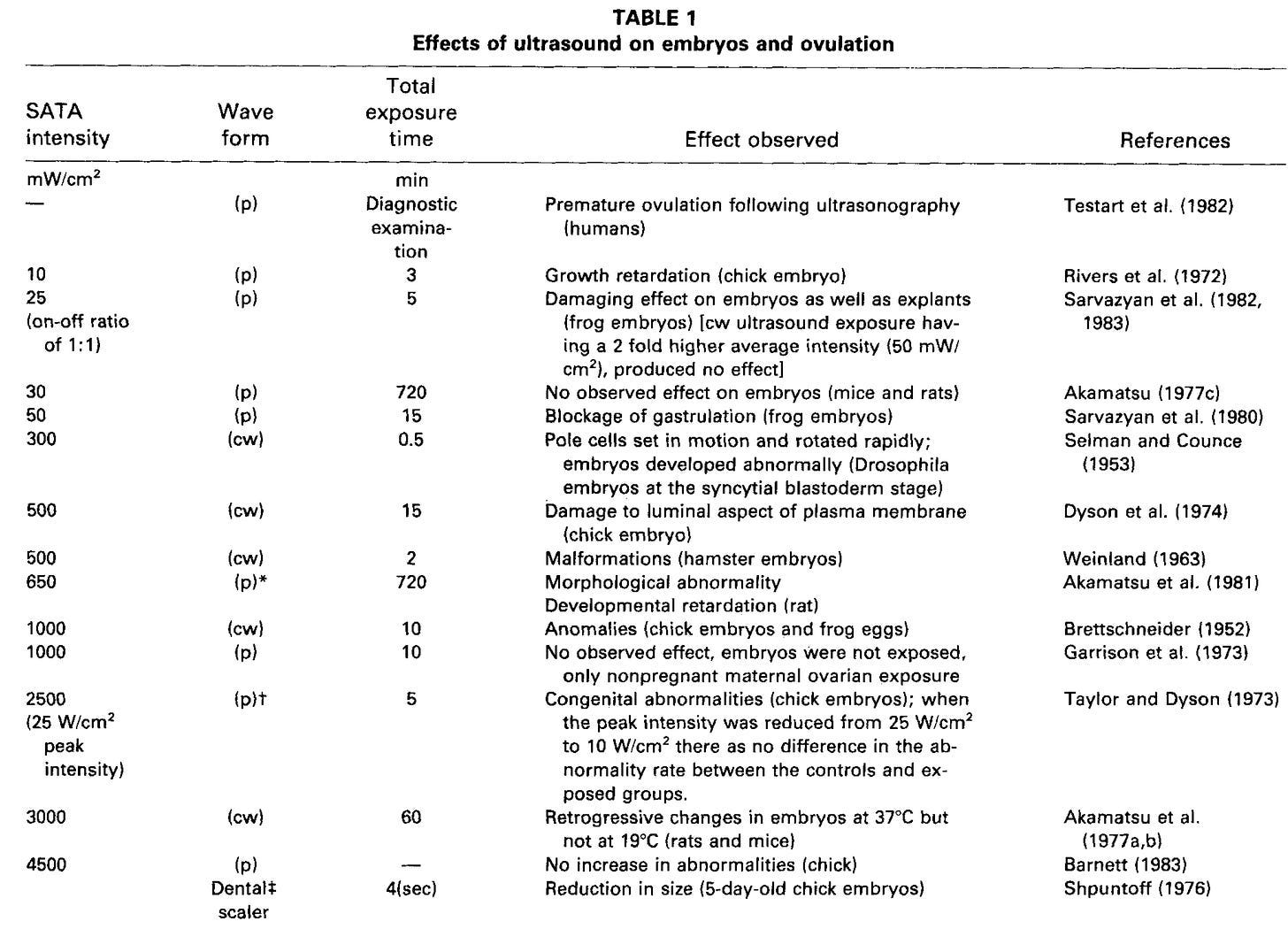
Reduced weight and size:
Fatal abnormalities:
Blood cell damage, increased clotting, and microcirculatory impairments:
Behavioral changes in rats and humans (along with dyslexia):
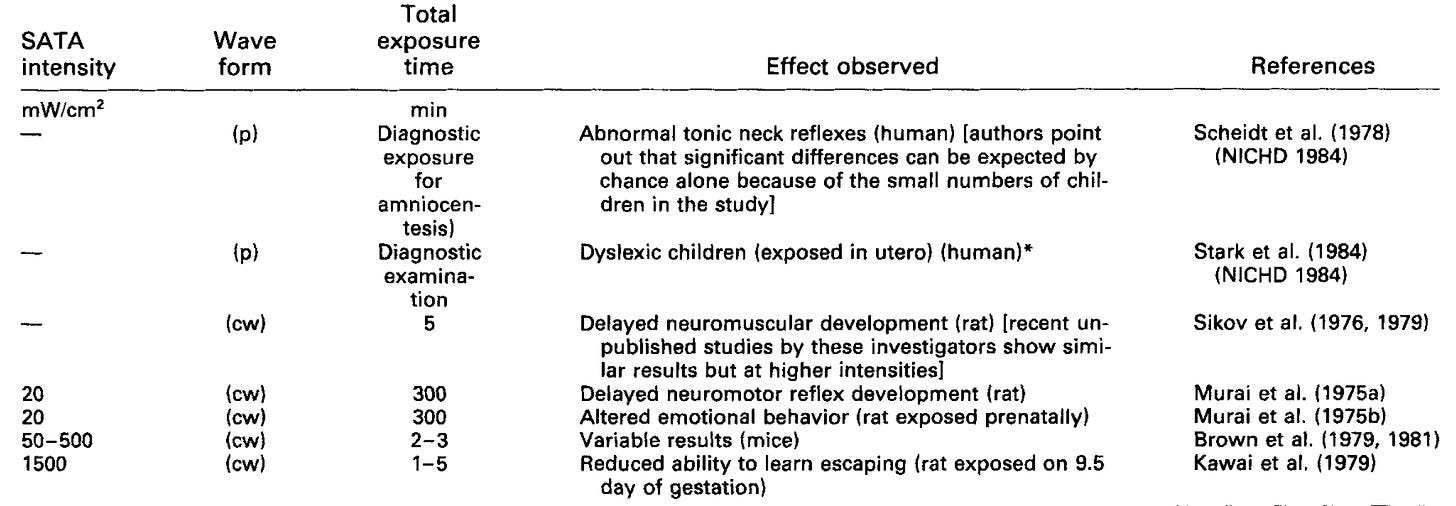
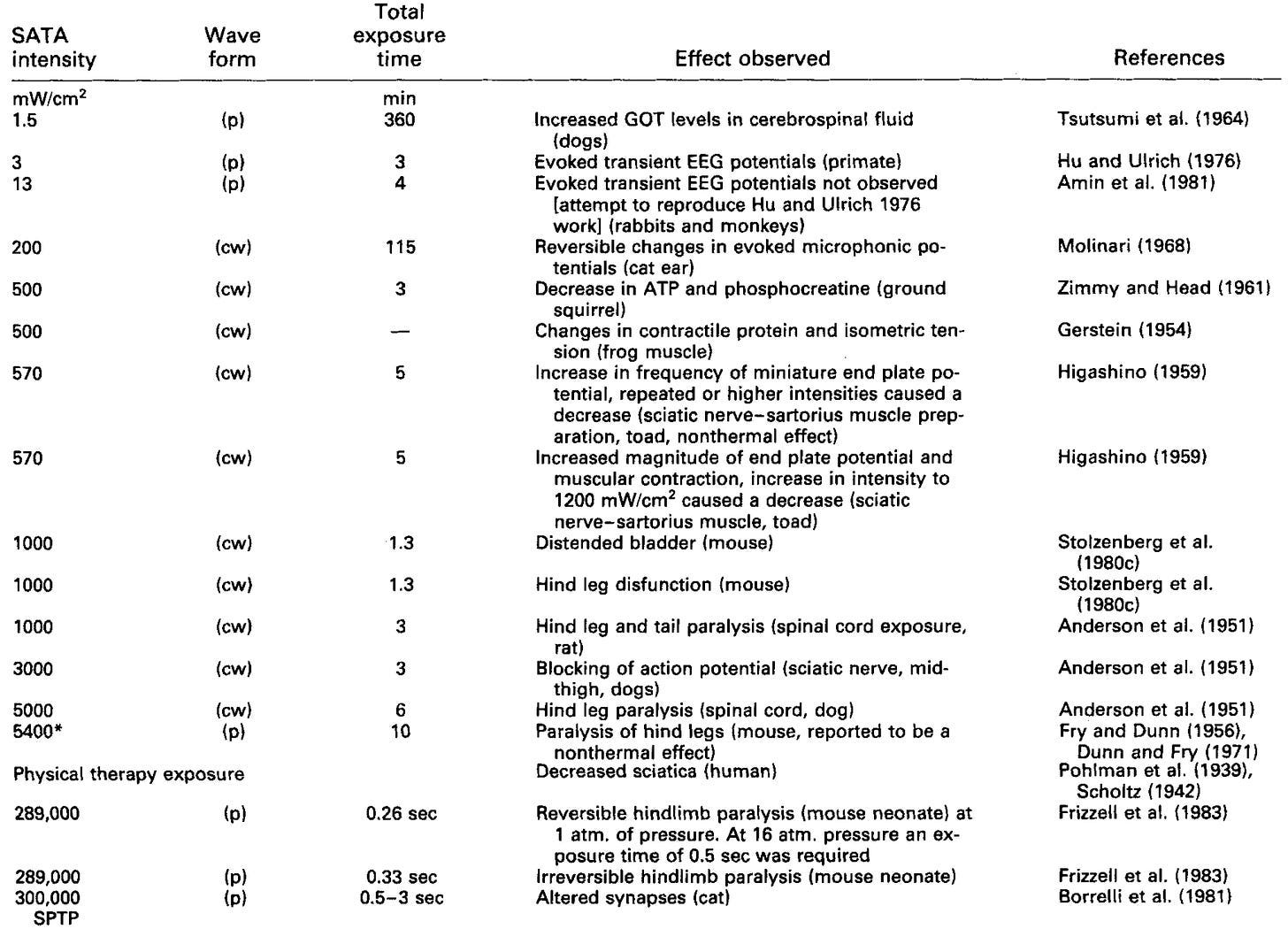
Abnormal nerve firing and abnormal muscle function (e.g., paralysis):
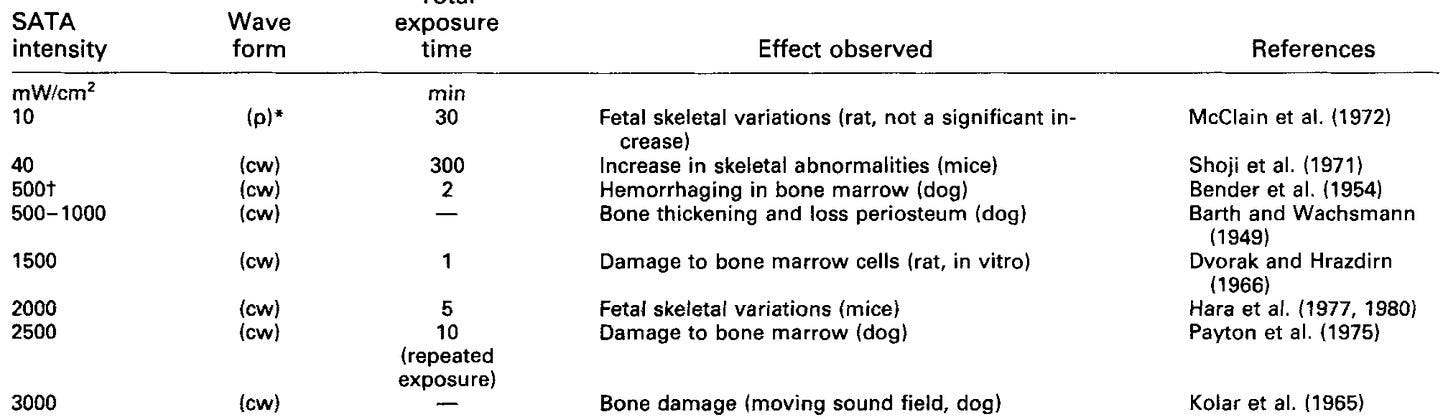
Bone abnormality and damage (e.g., marrow hemorrhages):
Additionally, this review also listed many US studies that demonstrated:
•Immune suppression
•Muscle changes and damage
•Damage to other soft tissues
•Liver damage
•Thyroid changes
•Eye damage (e.g., cataracts)
•A wide range of cellular changes.
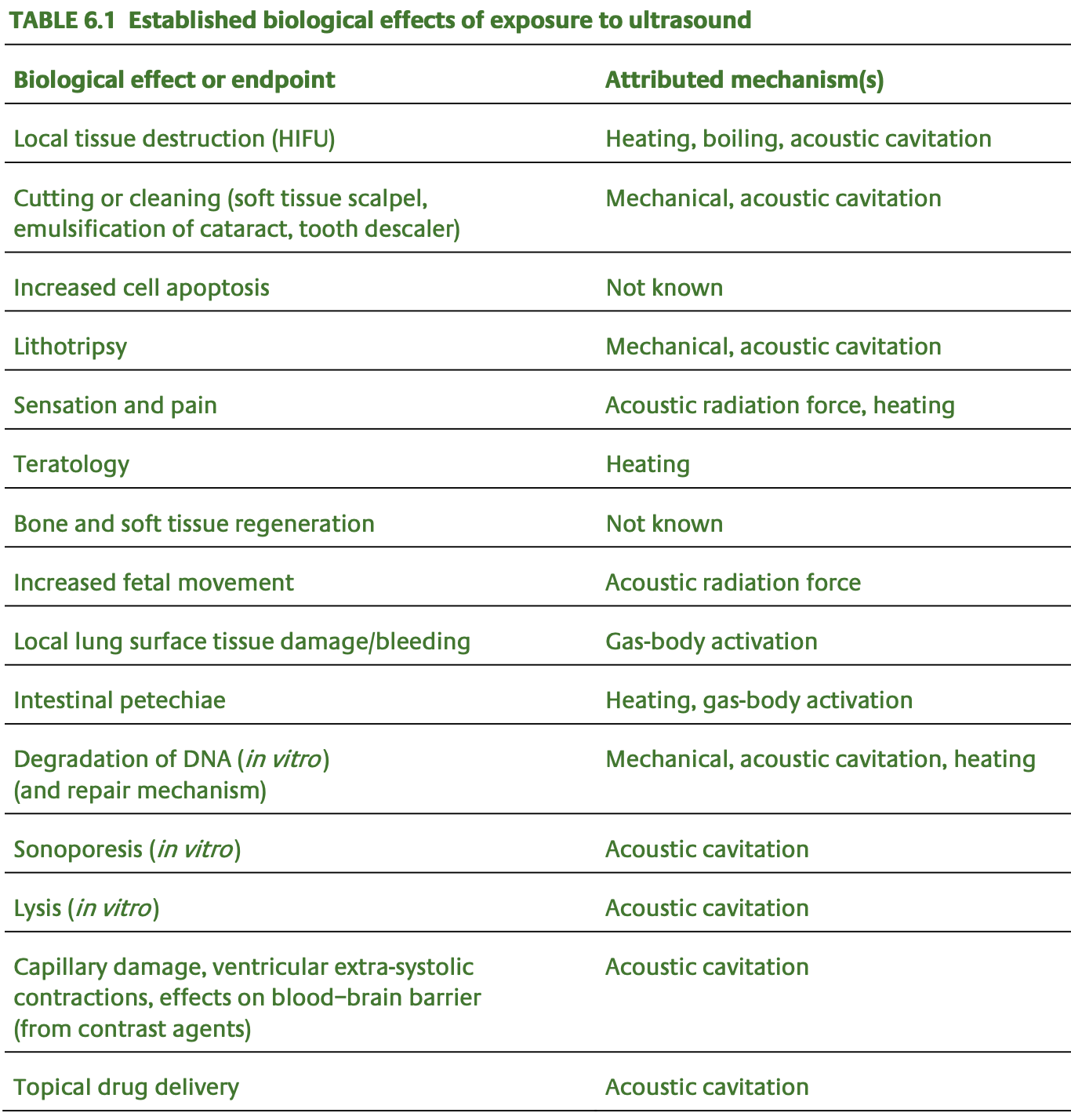
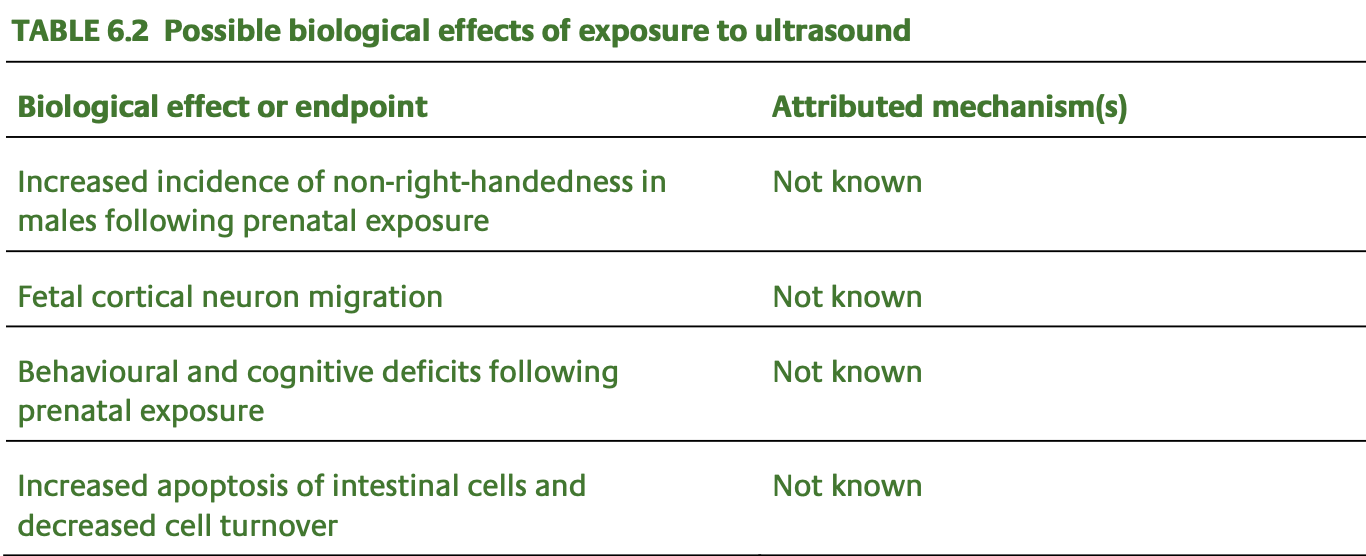
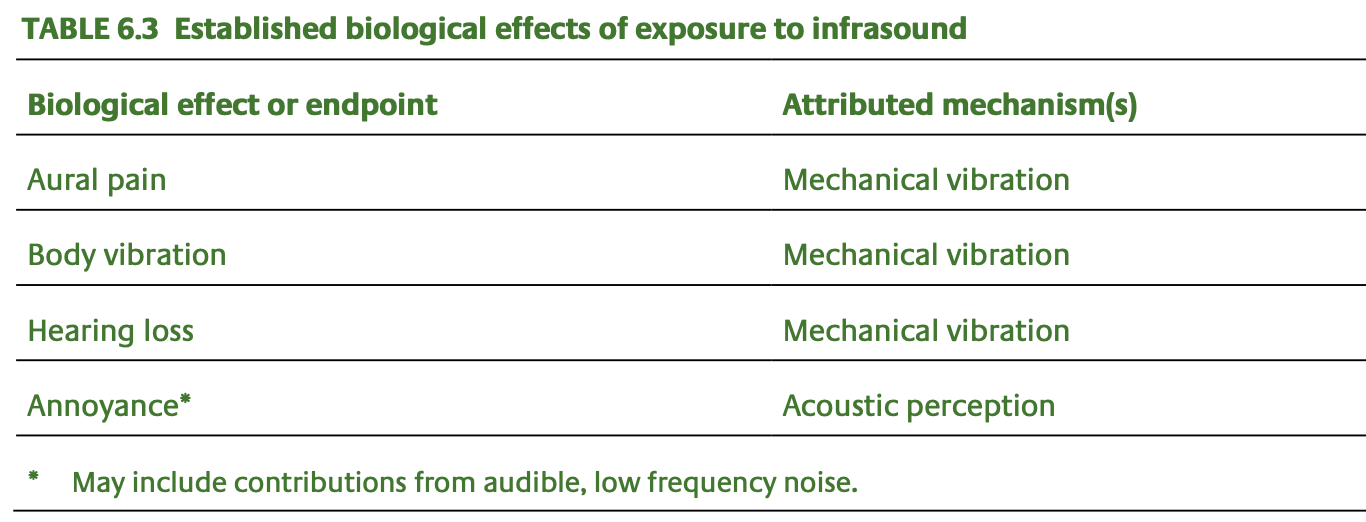
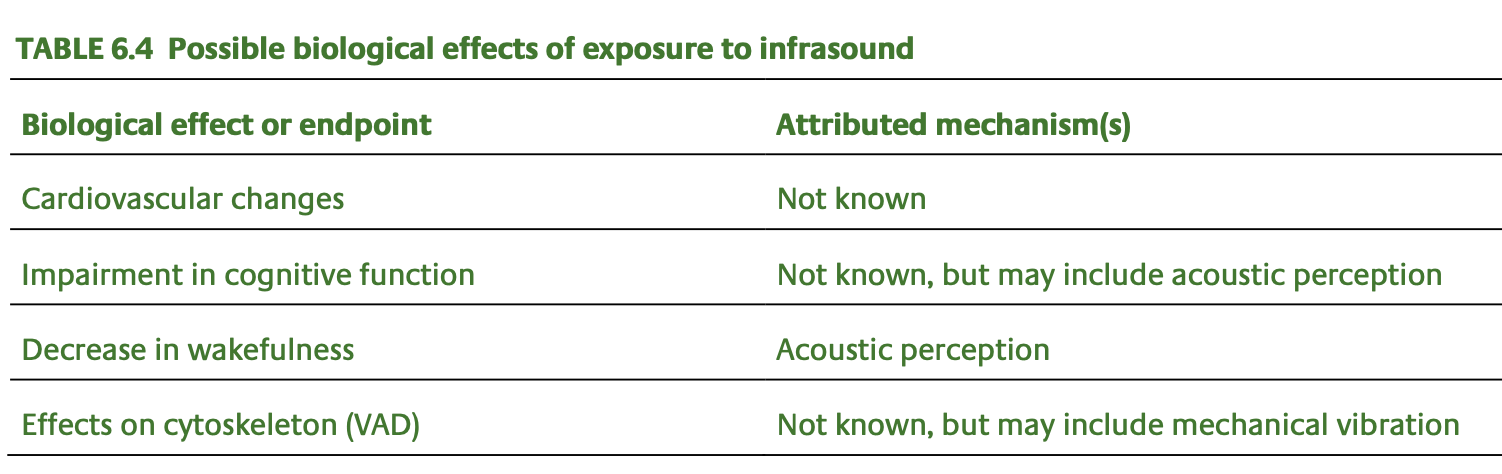
A 2010 report on US by England’s Health Protection Agency (which was quite detailed) concluded:
Ultrasound at high levels of exposure is capable of causing overt biological changes to living tissues, and these may be achieved through heating, cavitation and acoustic radiation force. For example, ultrasound can cause the destruction of kidney stones and induce localised necrosis to soft tissues, and prenatal exposure at levels well above diagnostic levels can result in teratogenic effects in animals.
These tables were sourced from that report:
A 2011 review on the cellular toxicology of US highlighted that:
•Thrombus (clot) formation after US-induced endothelial damage was one of the earliest demonstrations of its adverse effects.
•US facilitated an influx of calcium ions in fibroblasts, and this action may have resulted from a mechanical effect on ion channels (calcium ion influx often precedes cell death).
•Acoustic microstreaming was the postulated mechanism by which ultrasound caused efflux of intracellular potassium ions.
•Cells
will die when the concentration of solutes around them differs too much
from the cell (causing them to either swell or shrink), and when
ultrasound was used, smaller concentration differences became lethal.
•US can inactivate several enzymes and cause free radical production, both of which may initiate cellular injury.
•A
decrease in somite numbers (somites become vertebrae) was noted when
embryo cultures were exposed to ultrasound for 15 min at 40°C.
•Synaptic vesicles clumped when exposed to US (300 W/cm2) for 0.5–3 s.
Note: this 1997 review also examines the known biological harms of ultrasound.
Mechanisms of Harm
Presently, the following mechanisms exist to explain why US damages tissue:
1. Ultrasound heats tissue. To illustrate:
•A 2001 review
highlighted that US creates the greatest temperature elevation in the
head (due to the thickness of the cranial bones creating a high
absorption coefficient), which in one guinea pig study reached 5.2°C (whereas 4.0°C is thought to be the threshold where irreversible damage occurs).
•A 2007 review paper concluded the adverse effects to fetuses caused by US were most likely due to USs tendency to heat water up rather than the other mechanisms which had been proposed to account for those effects, and that under certain conditions, there was a real risk of these thermal effects being damaging.
•Heating is a dose-dependent effect (e.g., when focused US is used for neurological surgery, it can heat the tissue by 18°C).
•Since developing tissue is very sensitive to heat (e.g., mothers are encouraged to avoid excessive heat) many of the guidelines around safe prenatal US base the device limits on how much heating is acceptable.
2. US creates cavitations (dissolved gas in water expanding into bubbles which then collapse and create powerful shockwaves). To illustrate:
•One study for instance found that the acoustic pressure necessary to cause microcavitations in the blood was in the range of that generated by commercial ultrasound devices.
•Ultrasound contrast agents work by US causing cavitation bubbles to form which can then be seen with ultrasound.
•The most detailed review I’ve found on US generated free radicals (which are thought to be a key means through which it causes damage) shows that they are created from collapsing cavitation bubbles.
Note: I’ve written more about the biological importance of cavitation bubbles in biology here here.
3. The mechanical stress that US creates is sufficient to break apart the internal structure of cells.
Note: there are two other (less likely) mechanisms I’ve come across to explain how US affects cells. One is that it disperses the liquid crystalline water which coats cells (and plays a pivotal role in biology). The other comes from a Russian researcher who studies the sounds DNA emits (and their biophysical implications) and observed that exposing DNA to ultrasound overrides the diversity of sounds present in DNA, leading him to postulate they could be causing vast subtle damage to our species.
Of these, in the ultrasound literature, the temperature effects are the most commonly focused upon, mixed opinions exist around the biological significance of the cavitation bubbles, and the mechanical stresses are typically (but not always) viewed as being a result of the cavitation bubbles.
Note: numerous studies (e.g., see this 1997 review) have found rapidly dividing cells are more vulnerable to the adverse effects of ultrasound—which is concerning given that embryo cells rapidly divide.
Ultrasound Guidelines
As a large number of guidelines and review papers exist, it’s not possible to quote all of them. However, a few general trends can be found in them. These include:
•Despite US being “safe and effective,” many of the guidelines acknowledge that real risks exist from their use.
•Various degrees of caution exist on their use (e.g., avoiding medically unnecessary scans such as keepsake pictures of your baby’s face, making the exams as short as possible, avoiding them during the first ten weeks of life).
•As time went forward, those cautions were relaxed and reduced, especially after the 1992 FDA change on acceptable US levels.
Let’s now compare how the guidelines evolved over time:
•The authors of Williams Obstetrics, one of the primary textbooks for obstetricians (in numerous editions), states:
Sonography should be performed only with a valid medical indication, and with the lowest possible exposure setting to gain necessary information.
Note: the aptly named 2012 textbook “The Safe Use of Ultrasound in Medical Diagnosis” (which can be read online here) provides a significant amount of useful information about the biological effects of ultrasound and how parameters of devices can be adjusted to mitigate them.
•The American College of Obstetricians (ACOG), in their 1997 guidelines on routine ultrasound in low-risk pregnancy, concludes
In a population of women with low-risk pregnancies, neither a reduction in perinatal morbidity [harm to babies around the time of birth] and mortality nor a lower rate of unnecessary interventions can be expected from routine diagnostic ultrasound. Thus ultrasound should be performed for specific indications in low-risk pregnancy.
•The 1999 Australian Senate Committee report, ‘Rocking the Cradle’ recommended that the cost-benefit of routine scanning, and of current US practices, be formally assessed. Recommendations were also made to develop guidelines for the safe use of all obstetric US, as well as for the development of standards for the training of ultrasonographers). So far, none of these recommendations have been implemented.
•In 2004, the FDA put out a warning cautioning against getting US keepsake videos of what your unborn child looked like.
The 2015 guidelines from England’s Royal College of Obstetricians and Gynecologists urged caution in giving Doppler ultrasound to embryos less than 10 weeks old.
In contrast, the current ACOG guidelines (made in 2017) state that “there have been no reports of documented adverse fetal effects for diagnostic ultrasonography procedures,” states that there is no risk from the temperature changes induced by the highest intensity diagnostic US, but acknowledges that the theoretical risk means that US should be “be performed efficiently and only when clinically indicated” to reduce the “potential for risk.”
Note: some national health guidelines urge caution for workers using US. Canada for example lists multiple precautions US operators should take to avoid it entering their body.
Is Ultrasound Effective?
Most medical specialties have their “bread and butter” procedures, things which are routinely done for a large number of patients and hence make the medical specialties financially viable (e.g., routinely vaccinating children at each pediatric visit). While these procedures are “necessary” after assessing the risks and benefits of each one, my family has opted out of most of them and has not had any negative consequences from doing so. In turn, what I often find quite surprising is that the doctors who routinely do them typically aren’t familiar with the evidence behind the procedure and thus often can’t explain the risks and benefits of them (e.g., this has been the case for every doctor I’ve spoken to who routinely circumcises young boys).
Note: in addition to physicians facing liability for not performing these practices, many of them became established by intense lobbying from the AMA (through this Medicare committee) to guarantee high reimbursements for them, as this allows many medical specialties to be lucrative enough that young doctors will choose to specialize in them. This may however soon change as RFK Jr. has proposed removing the AMA from being able to set the reimbursement rates.
While medicine continually orders tests for everything imaginable, in a large number of cases, the value of those tests is quite questionable as the results will not change how a condition is managed (e.g., I know individuals with COVID vaccine injuries who have gotten hundreds of thousands of dollars of tests but none of those test results ever led to something being done).
Because of this, when ordering tests, unlike most of my colleagues, I typically (in an abridged fashion) tell the patient what the test could detect and what we will do depending on those results, particularly if I don’t feel they offer much for the patient or they pose an actual risk to the patient (e.g., contrast agents, particularly for MRIs have safety issues, and frequently will not provide anything of practical use that could not be gained from a non-contrast MRI scan).
In the case of prenatal US, something many do not appreciate is that their value is vastly overstated, especially early in pregnancy (when infants are the most vulnerable to the effects of US). To illustrate:
•A 2010 Cochrane review (the gold standard for evaluating medical evidence) of 11 trials comprising 37,505 women found early pregnancy US provided minimal benefit (there were no reductions in adverse outcomes for babies or in health service use by mothers and babies) but reduced failures to detect multiple pregnancies (e.g., twins) by 93% and inductions for ‘post term’ pregnancies by 41%.
A 2005 RCT of 4,187 pregnant women (28 and 34 weeks of gestation) found that umbilical Doppler monitoring led to a significant increase in the number of ultrasonographic and Doppler examinations subsequently conducted, but there were no other statistically significant effects on the management or outcome of the pregnancy.
A 1990 randomized clinical trial compared 57 patients being surveilled for preterm labor who received weekly pelvic exams or cervical US. Premature labor occurred in 52% of those receiving US, and 25% of those receiving pelvic exams. Those receiving US were more likely to receive tocolytic (labor inducing) agents (55% vs. 21%) and did not see any benefits from the monitoring.
•A 1993 BMJ meta-analysis of 15,935 pregnancies from 4 RCTs (randomized controlled trials) found US did not increase the live birth rate or reduced perinatal mortality and has a risk of incorrectly diagnosing fetal malformations.
•A 1993 NEJM double-blind trial of 15,151 low-risk pregnant women found that routine US screening resulted in 5% of those receiving routine US and 4.9% of controls having a severe adverse perinatal outcome and that “the ultrasonographic detection of congenital anomalies had no effect on perinatal outcome.”
Note: another use of ultrasound is to monitor a fetus's heart rate continually through the labor process. As I will discuss in the next part of this series (about the birthing process) there is no evidence this practice improves neonatal outcomes. Rather it just increases the rate of C-sections (e.g., in 1970 when it began, 5.5% of deliveries were C-sections, while in 2023 it was 32.3% of them).
When mothers receive prenatal US, since its use has become so normalized, they typically aren’t told how it actually benefits them. Briefly, it can:
•Tell you if you have a defective baby that “needs” to be aborted.
Note: one of the most common reasons for these abortions is a baby having Down Syndrome, a condition which to a large extent can be ameliorated with DMSO.
•Tell you the age of the baby.
•Tell you if you have twins (or triplets).
•Let you know the gender of your baby and what its face looks like.
•Tell you if you have an at risk baby that must be intensely monitored throughout the pregnancy.
•Tell you if the baby has a high risk condition that requires a C-section rather than vaginal delivery.
•Tell you if the baby has a high risk condition that requires intrauterine surgery (which applies to roughly 1 in 2000 pregnancies) or specialized surgical care immediately following childbirth.
However, there are major issues with most of these “benefits” (e.g., many don’t hold up—this study and this study for instance found dating a pregnancy by a woman’s last menstrual period can be as accurate as US dating).
In
regards to terminating a pregnancy (which is arguably the most common
use of a prenatal US—but something very few parents realize when they
agree to the test):
•Sometimes the US findings are
false positives (e.g., I know numerous people whose parents were
repeatedly told they needed to abort them, but their parents declined,
and when born had no issues). In one large trial that directly assessed it, was determined that 2.4 per 1,000 women who receive a prenatal US will have an erroneously identified defect (which translated to approximately a third of them being false positives), while another large study found 0.5% of women who were aborted for US findings had an erroneously terminated pregnancy.
Note: that trial also found, depending on the hospital, that US missed between 23.1-64% of fetal malformations.
Likewise, a 2002 study examined 124 fetuses who were diagnosed through US with a central nervous system malformation (CNS). Of these, 46% were aborted, 15% miscarried, and 39% were born. Of those who were born, 69% were still alive at 3 months, after which, one died at 4 months, two died at 3 years of age, and of the remaining 25, five were completely normal, seven were slightly disabled, and eight were severely disabled. What this essentially means is that the majority of infants identified with a developmental malformation “necessitating” an abortion are unlikely to survive, but about a quarter will survive and either be normal or only have minor disabilities.
At one point, the British press was filled with stories of women who may have aborted healthy babies due to inaccurate scans. In one [on page 9], Jacqui James of Brierley Hill in the West Midlands, a 24-year-old mother of two, was told scans done at Birmingham Maternity Hospital during her 27th week of pregnancy showed that her third baby was not growing properly and likely to have brain damage. After a family discussion, she decided she had no choice but to have an abortion. Because she was more than six months pregnant, the ‘abortion’ was done by cesarean section. However, the baby girl, who survived the operation for 45 minutes, was later found to be perfectly healthy.
An Australian mom went into labor last week, thinking that she may have only a few hours to hold her newborn daughter.
While she was pregnant, Dinah DeRegt was told that her unborn daughter had a terminal brain condition, and doctors recommended an abortion. DeRegt refused.
Then, on Dec. 2, baby Brianna surprised everyone when she was born completely healthy, according to the report.
Doula and photographer Serena Rollason who was there for Brianna’s birth said they all were in “shock” when doctors deemed her healthy.
“We literally saw the diagnosis. We spoke with multiple doctors and specialists in depth. We were referred to the pallative care team to ‘plan,’” Rollason said. “And on multiple occasions, even I was asked if I knew what I was in for and prepared myself for the journey that I was about to undertake as a doula supporting this family.”
Note: another common condition US tests for, Down Syndrome, is highly prone to false positives and requires 15,893 women to be scanned to detect one case.
•More
frequently, there is an ambiguous result (the baby “may” have a severe
defect), which results in the parents having immense stress throughout
the pregnancy (which is not good for the baby) and a large number of potentially harmful tests. For example, a 1988 study showed ambiguous results create significant anxiety, depression, and hostility for the mother. Likewise, in 1997
the British Medical Journal published a letter describing the severe
stress parents face when being told their baby may have a severe birth
defect (which is further discussed in this book that details the years of heartache many of these mothers go through).
Note:
two commonly recommended follow-up tests to abnormal ultrasounds,
amniocentesis and chorionic villus sampling (CVS) have a roughly 0.5-1% chance of causing miscarriages. CVS has many other risks (e.g., bleeding, infection, sensitizing the mother against the fetus's blood, limb deformities—many of which are also found with amniocentesis) and in a 3,248 person study
was found to decrease the likelihood of a successful pregnancy by 4.6%.
Based on the data I’ve presented thus far, I have long wondered if some
of the abnormal findings that result from CVS are actually due to US
(which is required to perform CVS) damaging the chorionic villi.
•Once parents are told to abort their baby, they are racked with guilt over it. In turn, if the fetus dies of natural causes, the parents can typically move on, whereas parents are often devastated for far longer after an elective abortion.
•Non-viable pregnancies will typically abort on their own.
Similarly, the early detection of defects requiring a higher level of care provides less benefit than patients realize.
Consider a 1997 study that evaluated 36 children with congenital defects who had received prenatal US. It found US at 17-18 weeks gestation detected 19% of them, and overall (when including later ones), detected 36% of them (2/8 in diaphragmatic hernias, 6/12 abdominal wall defects, 5/13 meningomyeloceles and 0/3 bladder exstrophies). In those whose defects were detected with ultrasound (and the management of their labor was thus altered), 77% survived, whereas for those whose defects were missed and nothing was done, 96% survived. Additionally, for those who needed abdominal wall surgeries, it took 13 hours for those in the unscanned group to get surgery (whereas it took 4 hours in the scanned group), but no difference in mortality resulted. Finally, those with early detection tended to be delivered earlier (typically by C-section) and had a variety of other issues (e.g., lower Apgar scores at birth, lower birth weight, more time spent on the ventilator, etc.).
Because of all of this, a strong argument exists that US should either be:
•Only used near the end of the pregnancy (to be better prepared for labor).
•Only used if signs of a more serious condition are present (e.g., vaginal bleeding).
•Not used at all.
Healthy Children
At a very young age, I realized the authorities we trusted would routinely lie. Because of this, I adopted the belief that many things we were told were “safe” weren’t. As such, I routinely avoided things where there was any uncertainty regarding their safety—an approach I later learned was encapsulated by the “Precautionary Principle” (something which is practiced significantly more in Europe than in America).
Even though it’s often a hassle (and sometimes completely pointless) to do that, I’ve had so many times this approach allowed me to avoid something that ended up being disastrous for many others. In the case of children, while I am typically very accepting of people who do things I disagree with, I was quite pushy to ensure the Precautionary Principle (e.g., no ultrasounds or vaccines) was followed for the children in my immediate circle.
In turn, we (and everyone else who interacted with them as they grew up) noticed those children were completely different (e.g., much happier, healthier, aware, and intelligent—to the point many who met the babies wished they could keep them), and on so many levels it’s been heart wrenching to see how much of what our society now views as being normal with children in reality is a profoundly damaged state of health and not the way our children should be.
In the final part of this article, I will discuss some of the approaches we’ve found to be the most helpful before and during pregnancy to help the mother (e.g., to reduce back pain, pre-eclampsia, and edema), prevent miscarriages and ensure a healthy child (along with some of the safer prenatal diagnostic alternatives)—many of which I am still in disbelief the obstetrics field has not widely adopted.
No comments:
Post a Comment