Story at a Glance: •Proper
sleep is one of the most important things for our health, and when it
is disrupted, many severe issues consistently emerge (e.g., heart
attacks, psychiatric illnesses, car accidents, fatigue, diabetes,
cognitive impairment, or dementia). •In
1964, a sleeping medication hit the market that was remarkably
effective for a variety of conditions (including insomnia) and hence
profoundly improved the health of its recipients. •In this article, we will review the data that illustrates the harms of poor sleep, the common causes of poor sleep, and the most effective treatments we have found for sleeping disorders that are still available to the public. One of the key themes I’ve tried to illustrate throughout this publication is that chronic illness has vastly increased over the last 150 years. Furthermore, again and again, doctors of each generation who observed each successive wave of that increase noticed that the treatments they learned at the start of their careers were much less effective for treating the patients they saw at the conclusion of their careers.For example, here recent article, I discussed this collective loss of vitality in more detail, and listed what I believed were the primary culprits (which has been quite a challenge as there are now so many unhealthy things in our environment). In addition to listing the key culprits many are familiar with (e.g., the vaccination program has had a horrific impact on our health), I proposed another primary cause of chronic illness was modern life being highly disruptive to the natural rhythms the body depends upon for self-regulation and self-repair. I believe this concept is relatively under appreciated within Modern Medicine (Allopathy) because, unlike almost any other medical system in history, our scientific approach to understanding the body does not recognize the concept of an innate “health” of the body, and as such, many Allopathic treatments are based around doing what they can to stabilize (e.g., in the ICU) or alter the body (e.g., through a surgery) and then hoping the body eventually works things out from there. In contrast, most other medical systems focus on what can be done to augment this innate capacity for recovery (health) and trust that through doing so, the present issue will resolve itself. Note: typically the Allopathic approach (forcing the body to assume the state deemed necessary for the patient) is ideal to utilize for acute conditions, whereas the health-augmenting approach is what gets the best results for chronic conditions (something Allopathic medicine is well-known for struggling with). At this point, I believe there are three reasons why we utilize the Allopathic model (discussed further here) rather than the health-focused model: •Knowing if a therapy actually “works” is quite challenging, especially if the change can only be observed over a long time. Because of this, most medical research is based on whether an overt change can be consistently observed within a patient (e.g., lowering their blood pressure) and hoping that change will yield a long-term benefit rather than evaluating the long-term prognosis of people who receive a medical intervention. Because of this, medical research is strongly biased towards evaluating treatments that create an overt change (e.g., pharmaceutical drugs) rather than ones that augment the body’s health and lead toward a gradual recovery. Likewise, it is much easier to diagnose someone by their symptoms (and prescribe drugs to treat those symptoms) than it is to identify the root cause of their disease. Self Regulating CyclesThe “health” of the body is highly dependent on the normal functioning of a variety of repeating cycles that occur within it. For example: •Practicing slow, smooth, and expansive nasal breathing has a profound impact on one's health and longevity because breathing regulates many different critical physiologic functions. •
Normal exposure to sunlight serves a variety of critical functions for
health, and once it is lost, one’s risk of dying doubles, and a variety
of other conditions, such as depression set in (discussed further here). •The mind is designed to alternate between periods of rest and activity. Yet, in our modern era, we have to think constantly, which often occurs in conjunction with significant stressors. •Humans are meant to alternate between periods of eating and not eating (fasting) rather than continually eating. In
short, many of the natural rhythms our bodies rely upon for
self-regulation are heavily disrupted in modern society, which in turn
results in a variety of consistent derangements to normal physiology
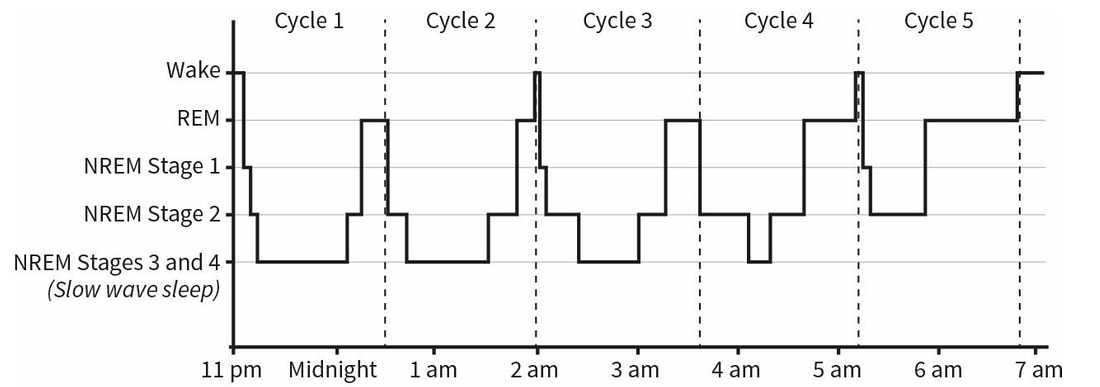
that are now seen throughout the population. The Importance of SleepThroughout my career, I’ve met countless integrative practitioners who believed that one of the most important things to do when treating a chronic illness is to normalize their patient’s sleep, as this cyclical process is one of the foundational methods the body uses to restore its health. Unfortunately, patients with chronic illnesses tend to have highly disrupted sleep cycles which are often very challenging to correct (e.g., insomnia is fairly common following a COVID-19 vaccine injury). The important thing to understand about sleep is that it is a tightly regulated cycle which is both highly responsive to signals from the environment and also responsible for maintaining many of the other critical rhythms within the body. During sleep, the body cycles through different phases of sleep, each of which performs a critical function (e.g., deep NREM sleep heals the brain and allows toxins to drain out of it through the glymphatics, while REM sleep consolidates memories and allows one to process the emotions of their experiences). A typical sleep cycle goes as follows:
Note: since REM sleep predominates later at night, not sleeping long enough disproportionately disrupts REM sleep. Matthew Walker is one of the world’s most vocal sleep researchers. In his book Why We Sleep, he argues that some of the most important functions of sleep include:
I generally agree with this list (and will cite more studies supporting it later in the article). Likewise, I am sure many of know firsthand how bad you feel when you are sleep deprived. Here are some of my personal experiences with sleep: •I am fairly sensitive to the baselines within my body and I immediately notice that things within me go awry if I’ve had insufficient sleep. For example, I notice impairments in a variety of neurologic functions (e.g., I become significantly less able to tolerate the cold, my coordination worsens, and it’s much harder for me to maintain my focus in either an intellectual or social task). •During periods of significant sleep deprivation, I will notice I have fleeting pain within the heart muscle and periodic arrhythmias. This is corroborated by a study that found one night of modest sleep reduction (as little as one or two hours) quickly increased one’s heart rate and blood pressure. •During
periods of insufficient sleep, I experience general mental fogginess
that persists until I get a good night's sleep (and sometimes two). Note: NREM sleep is responsible for eliminating unnecessary memories, whereas REM sleep processes the day's experiences and reinforces them into long-term memory. •I tend to gain weight during periods of poor sleep. Finally, Walker cites many examples of severe consequences occurring after prolonged periods of significant sleep deprivation (e.g., death or psychosis). I have also seen similar things occur. For instance, periodically I will have a patient who comes to me after engaging in an unsafe spiritual practice which involved staying awake for multiple days, after which they developed a permanent psychiatric or spiritual disorder (discussed further here). Quantifying the Importance of Sleep
ImmunityDuring periods of sleep deprivation, immune system function significantly decreases. Some of the consequences of this include: Cancer—Numerous studies have found an association between sleep deprivation and cancer (while conversely, others have not—which I believe is due to the difficulty of properly studying this topic). Data supporting the link includes: •In 2010, using all the available evidence, the WHO classified shift work (one of the most reliable ways to heavily disrupt natural sleep cycles and something many workers in the healthcare field experience) as a probable human carcinogen. This link is also supported by a 2023 review paper. •An English study of 10,036 people over 50 found that poor sleep resulted in a 33-62% increased risk of cancer. •Existing data shows that sleeping pills (which disrupt normal sleep) are associated with a large increase in one’s risk of cancer. Note: the increased cancer risk from poor sleep may also be due to disturbances in the body’s normal release of melatonin or insufficient tissue oxygenation. Infections—individuals who are sick are more likely to develop infections (e.g., most times I get sick are after periods of prolonged poor sleep). Some of the evidence to substantiate this common observation includes: •Rats that are not allowed to sleep deteriorate and eventually die. When death occurs, it is typically due to sepsis from their gut bacteria. •A study determined how much sleep research subjects had had in the last week and then exposed them to the common cold virus (by squirting it in their nose). It found those who had averaged less than 7 hours of sleep were 2.94 times more likely to develop a cold than those who had more than 8 hours. It also found those with poor sleep efficiency (how much of the time bed you are asleep) were 5.50 times more likely to develop a cold than those with good sleep efficiency. A study
of 56,953 nurses found women who slept 5 hours or less were 1.7 times
as likely to develop pneumonia over a 4-year period compared to those
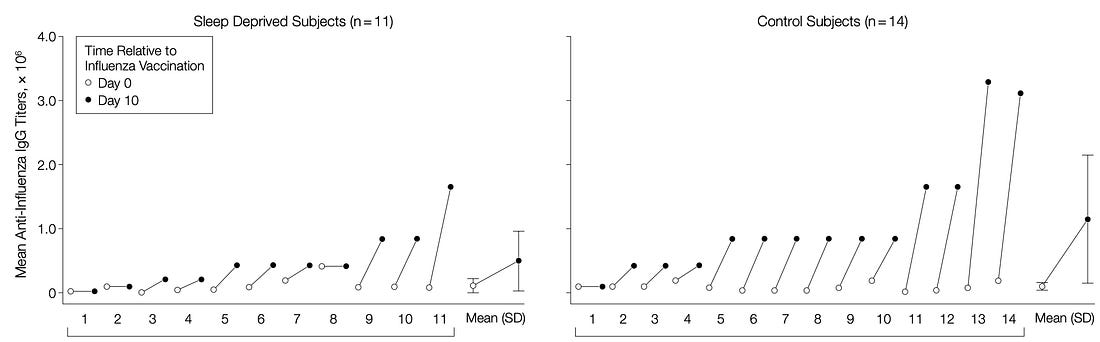
who slept 8 hours a night.
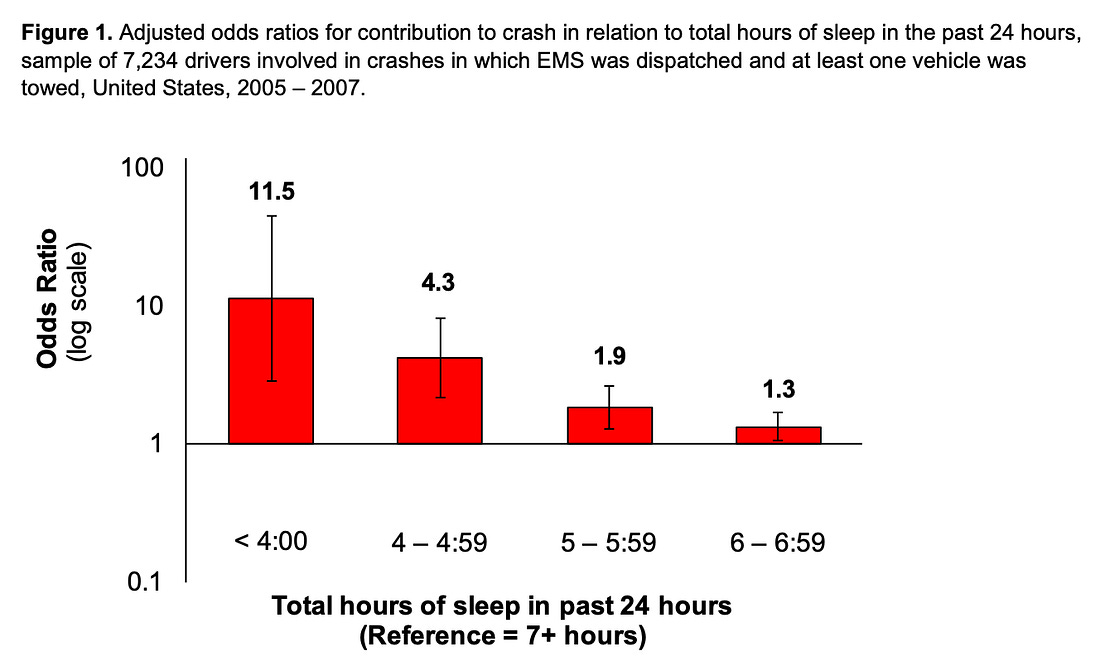
Note: this association has also been seen with other influenza vaccines along with hepatitis A and B vaccines. •When patients take sleeping medications that interfere with the sleep cycle, they have a significantly increased rate of infections (e.g., one large study found they increased one’s risk of pneumonia by 54% and one’s risk of dying from pneumonia by 32%). Car AccidentsWhen people are sleep-deprived they have significant impairments in their attention (which a third of the population is particularly vulnerable to), their reflexes decrease, and they intermittently completely lose their awareness of the environment (e.g., because the brain engages in micro-sleeps). In areas of life where a split second can make all the difference, this can be highly consequential. For instance, when the rates of road accidents are looked at, “drowsy driving” has been found to be as dangerous as drunk driving. For example, consider this study:
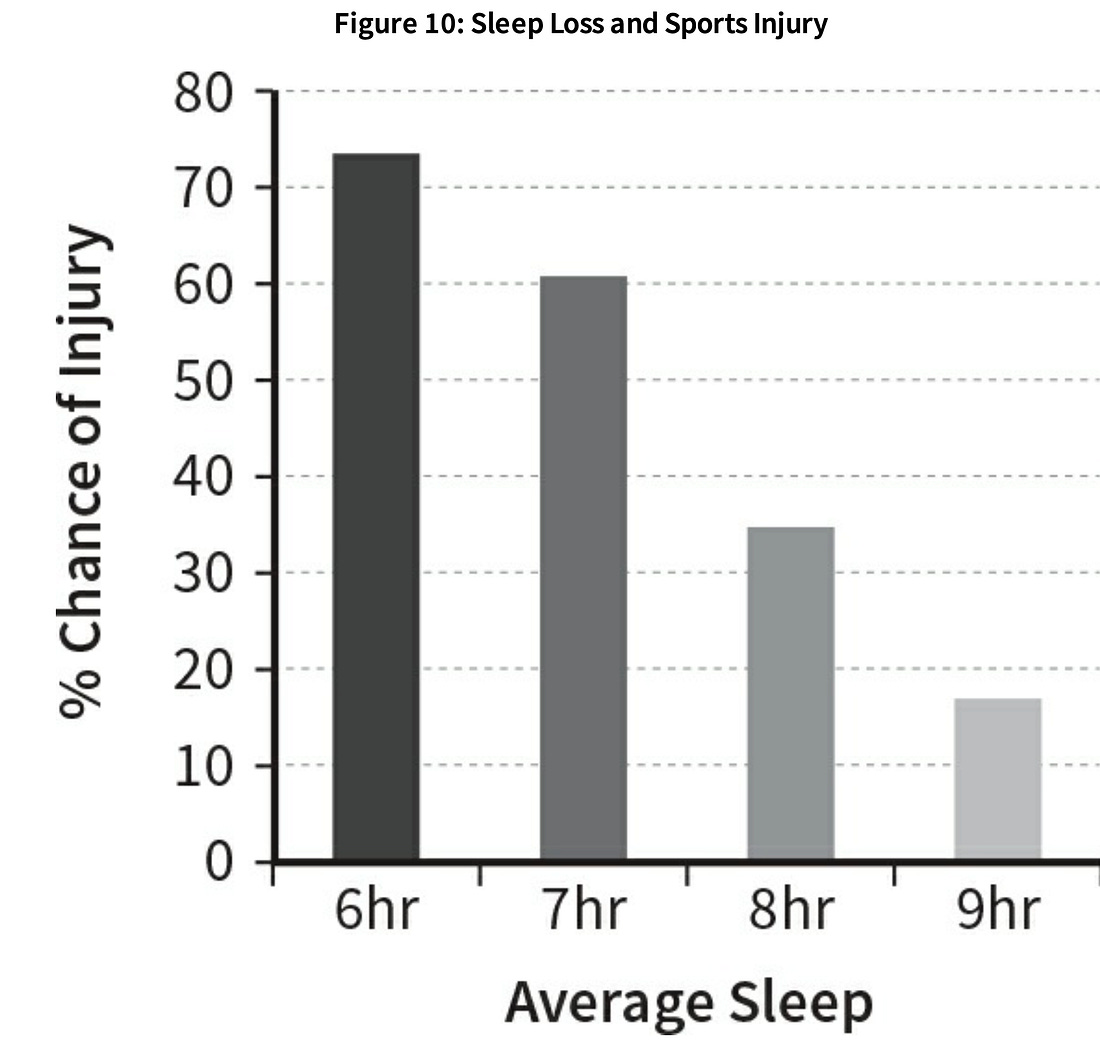
Note: for comparison, those with a blood alcohol content of 0.08 are 4X more likely to crash, whereas those with a BAC of 0.15 are at least 12X more likely to crash. As teenagers have the greatest need for early morning sleep (due to their circadian rhythm being shifted forward) compelling data supporting this hypothesis has emerged in areas which had their school start times become later. Specifically: •When a county in Kentucky made schools start an hour later, it resulted in a 16.5% reduction in car accidents with teen drivers (whereas during that period accidents increased by 7.8% in the rest of the state). •When a Minnesota school district moved their schools’ start time from 7:30 to 8:00 a.m., depending on the district, there was a 6-70% reduction in traffic accidents in drivers 16-18 years of age (which averaged out to a 13% reduction). •When a Wyoming school district moved their start time from 7:35 to 8:55 a.m., there was a 70% reduction in teen driver car accidents. Similarly, the loss of focus and coordination created by sleep deprivation also often leads to sports injuries.
Heart DiseaseThere is a strong link between heart disease and sleep deprivation. For example: •When time shifts forward during daylight savings (which results in people having to wake up an hour earlier) a 24% increase in heart attacks is observed, while conversely, when the clocks shift back, a 21% decrease occurs. •A 2011 study
of 474,684 people across the globe found that shortened sleep was
associated with a 48% increased risk of developing or dying from heart
disease over 7-25 years. •A Japanese study
of 2,282 male workers found that those who slept less than 6 hours a
night were 4-5 times more likely to have a coronary event (e.g., a heart
attack or prolonged chest pain requiring catheterization or surgery)
attack than those who slept between 7-7.9 hours each night. •A 2019 study found those with high blood pressure or diabetes who slept less than six hours had twice the risk of dying from heart disease or stroke compared to people who slept six or more hours. •Sleep deprivation damages the lining of the blood vessels and shuts off the release of growth hormone (which is critical for the health of that lining). This is important, since heart disease is largely due to damage in that lining. •Insufficient sleep impairs the brain’s control of blood vessel function, hence raising blood pressure. •Sleep loss increases the levels of the white blood cells, which causes inflammation within the blood vessels. •A study of 23,620 Europeans
found that those who slept for less than 6 hours per day were 41% more
likely to experience strokes and 44-78% more likely to experience heart
attacks. Diabetes and Obesity:Diabetes is defined by too much sugar being in the bloodstream (e.g., because cells no longer respond to insulin telling them to absorb the sugar or because too much sugary food was eaten). In the case of insufficient sleep: •Numerous studies (e.g., this one and this one) have found insufficient sleep increases the desire for sugary foods, and increases the tendency to overeat them, along with increasing the hormones that cause hunger. •Numerous studies (e.g., this one and this one) have found that poor sleep elevates blood glucose levels and decreases insulin sensitivity. •There is a direct relationship between the health of one’s gut microbiome and the health of one's sleep. •A meta-analysis found insufficient sleep made children 89% more likely to be obese and adults 59% more likely to be obese. Note: many of the conditions sleep deprivation worsens are considered to be interrelated (e.g., diabetes greatly increases one’s risk for heart disease, and both heart disease and diabetes greatly increase one’s risk for Alzheimer’s disease). Because of this, the effects of poor sleep are often much greater than initially appreciated. Learning:One of the most important functions of sleep is that it determines which memories from the previous day should be retained (the rest are “eliminated” during NREM sleep) and then integrates them into long-term memory during REM sleep (e.g., see this study and this review article). Furthermore, it also integrates tasks the body had difficulty with during the day. For example, consider this anecdote which was shared with Walker:
Walker has focused on this area and conducted a large volume of research (which can be found here) that demonstrates sleep is essential for all aspects of learning. For example: •Numerous studies (e.g., this one, this one) have demonstrated that sleep is responsible for developing fine motor skills (e.g., being able to quickly and smoothly perform a task that requires significant coordination) and that the integration is facilitated by NREM 2 sleep (especially what occurs in the last two hours of an eight-hour night of sleep). •Numerous studies (e.g., this one) have demonstrated that sleep transfers short-term memory to long-term memory, while sleep deprivation has been repeatedly shown to impair retention. •Sleep plays a key role in episodic memory (one’s memory of events that happened that day) and in memory consolidation. •Prolonged wake time impairs learning, while healthy sleep restores it. •Impaired sleep has been shown to account for the difficulty older adults often have retaining new memories. Mental Health:There is a longstanding association between psychiatric disorders and impaired sleep (e.g., as mentioned above, schizophrenia and psychosis are linked to poor sleep). In turn, my more integrative psychiatrist colleagues consider optimizing sleep to be one of the most important things they can do for their patients. To illustrate: •Sleep deprivation increases emotional reactivity and impulsivity, and engaging in risky activity (e.g., gambling). Conversely, healthy sleep decreases one’s reactivity to traumatic experiences. •Poor sleep has been shown
to significantly increase one’s autonomic response to unpleasant things
in their environment (e.g., they become more easily upset by them). •Studies (e.g., this one and this one) show that poor sleep predisposes one to anxiety. •Sleep loss makes individuals less able to accurately interpret non-verbal expressions, (e.g., see this study), which causes them to feel more threatened by those they encounter) and amplifies basic emotional reactivity, thereby increasing negative mood states (e.g., anxiety, depression, suicidality). Conversely, healthy sleep improves positive mood states and decreases emotional reactivity. •Sleep loss has been shown to cause social withdrawal and loneliness. •Sleep loss makes individuals less willing to help others the next day, and when the daylight savings transition occurs, donations to charity decrease. •It is well known in psychiatry that bipolar episodes are triggered by sleep deprivation. One study that artificially created this situation found impaired sleep worsened a patient’s bipolar disorder. Note: individuals with psychiatric disorders also frequently have impaired memory retention (another symptom of sleep deprivation) which may prevent them from retaining the lessons of psychotherapy sessions. Cognitive Impairment:As many of you know from personal experience, sleep loss is well recognized to cause brain fog and cognitive impairment (e.g., this study demonstrated sleep depriving test subjects worsened their auditory processing and responses on neurophysiological tests). This process is particularly consequential in the elderly (who are widely recognized to be more susceptible to memory loss and cognitive impairment), and likewise more likely to suffer from impaired sleep as they age. As this review paper shows, a significant body of research hence ties poor sleep (especially if chronic) to dementia. For example: •A study compared 105 older women with sleep-disordered breathing (which impairs sleep) to 193 without it and found that sleep-impaired individuals were 71% more likely to develop mild cognitive impairment and 104% more likely to develop dementia. •In one study, 737 older adults initially without dementia received annual measurements of their sleep quality, their cognition, and the presence of Alzheimer’s Disease (AD). After 6 years, individuals with poor sleep (high sleep fragmentation) were found to have a 22% increase in their risk of AD, with those who had the worst sleep fragmentation having a 50% increase. •A study
recruited 346 patients with normal cognition, averaging 75.9 years of
age, 80 of whom had insomnia. It found those with insomnia were 139%
more likely to develop AD. Furthermore, many studies have directly tied poor sleep to the pathogenesis of AD. For example: •A remarkable 2020 study
of 32 individuals without cognitive impairment who received an average
of 6.1 months of sleep assessments and 3.7 years of PET scans (a
non-invasive way to measure Alzheimer’s plaques in the brain) found that
disrupted sleep caused an accelerated accumulation of Alzheimer’s
plaque and forecasted the development of dementia. These results are
very important as most adults at this stage do not recognize the damage
accumulating in their brain which will inevitably lead to dementia. It is thus remarkable that sleep is rarely considered in the field of AD, given that AD is one of the most costly diseases in society. Unfortunately, like many other areas in medicine, all of that knowledge has been buried, and for decades we’ve instead spent billions of dollars each year on (flawed) research to develop incredibly expensive drugs which, at best, may slow the progression of AD (which simultaneously have a wide range of severe side effects such as causing brain swelling and brain bleeding in 41% of those who receive them). Note: this article only scratches the surface of the research on the benefits of sleep (e.g., women sleeping less than 8 hours have a 17% reduction in follicular-stimulating hormone, are 30% more likely to have abnormal menstrual cycles, and may have reduced fertility, relative to those obtaining sufficient sleep). However, I hope what I presented here sufficed to make the point that sleep is very important. The Sleep Crisis“Adequate sleep” in turn requires one to achieve all of the following: •Have enough time set aside to sleep. •Being
able to fall asleep once you are in bed (as if you lie awake for 2
hours of a “8” hour sleep, you are only actually sleeping for 6 hours). Note:
significant debate exists as to exactly what constitutes enough sleep.
It is generally agreed that normal adults, need between 7-9 hours a
night (whereas many, myself included believe 7 hours a night is too
low). Furthermore, the amount humans need varies with age and to some
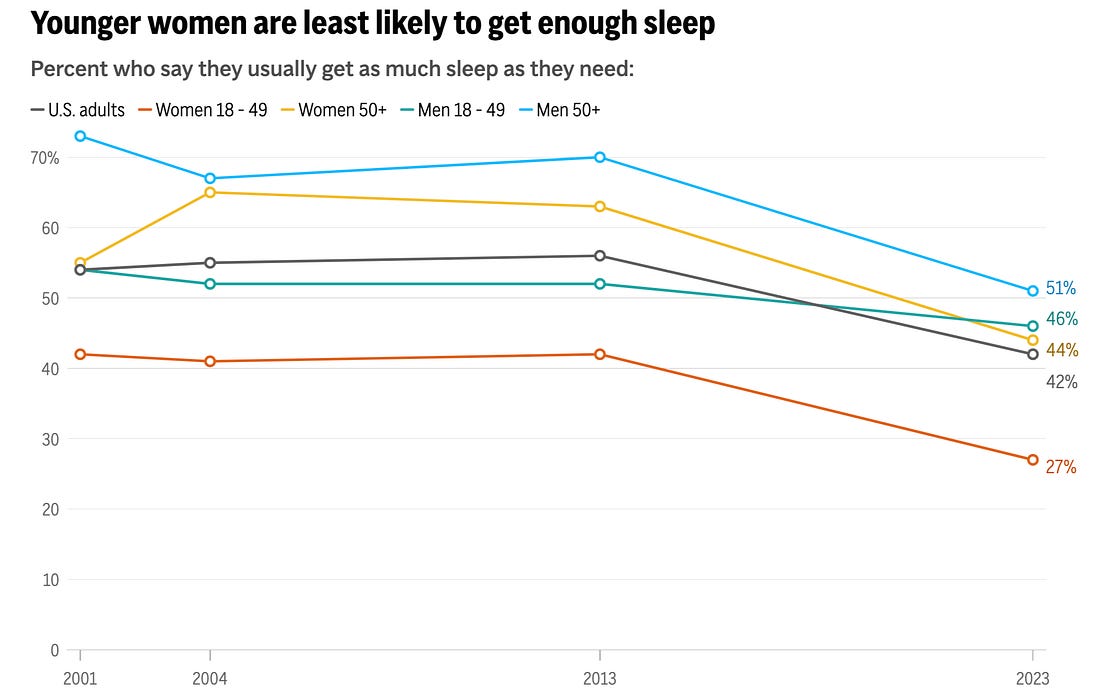
extent by individual. Sadly, we get nowhere near that much sleep, which in turn likely plays a key role in the widespread illness throughout our society. For example, a Gallup poll, released April 15, found 57% of Americans say they would feel better if they could get more sleep, while only 42% say they are getting as much sleep as they need. More concerningly, these numbers have continued to worsen as the years go by (which I believe is a symptom of the fact we are being forced into a feudalistic economy that overworks everyone so they can never challenge the system).
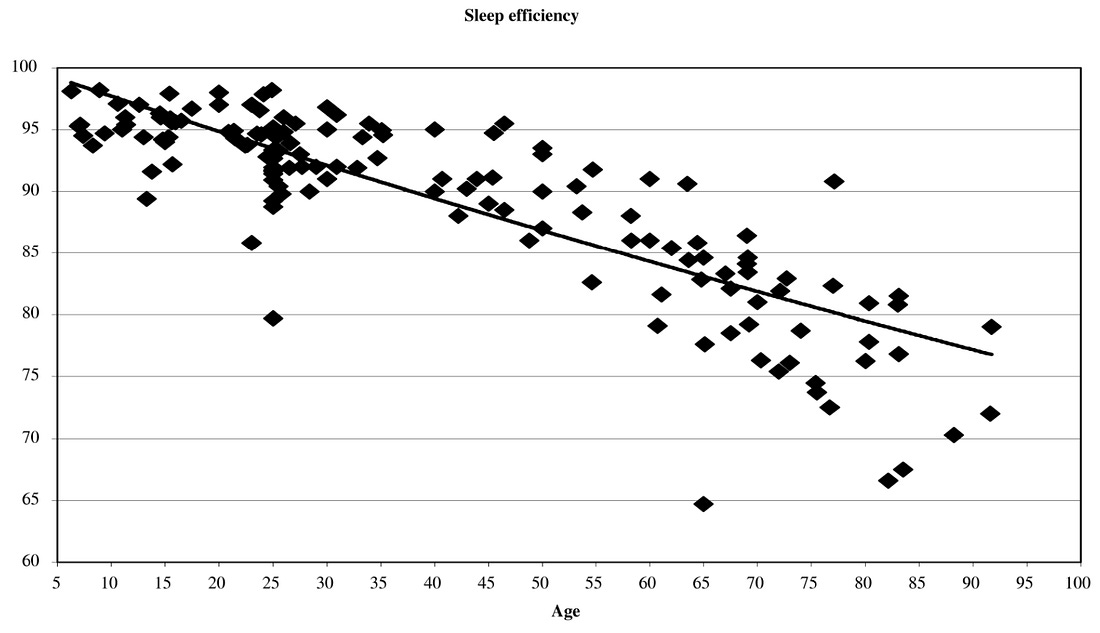
Furthermore: •35.5% of American adults report they sleep less than 7 hours per night. •Roughly 30% of adults have symptoms of insomnia, with 14.5% experiencing insomnia all (or most days) of the month and 10% having insomnia which impacts their daily activities. •13.5% of adults report feeling tired or exhausted most days. •Poor sleep (e.g., insomnia, early awakening, or not feeling rested) is even more common in the elderly (who have the greatest need for sleep). For example 1995 study of over 9,000 individuals 65 or older found less than 20% rarely or never had sleep issues, while more than 50% reported sleep issues most of the time (e.g., 23-34% had symptoms of insomnia). That study in turn found that many of the consequences of poor sleep discussed earlier were elevated in those with sleep disturbances. More current estimates find that 30-48% of the elderly experience symptoms of insomnia and between 12-20% have insomnia disorders. •As we age, we become less able to spend all of our time in bed being asleep:
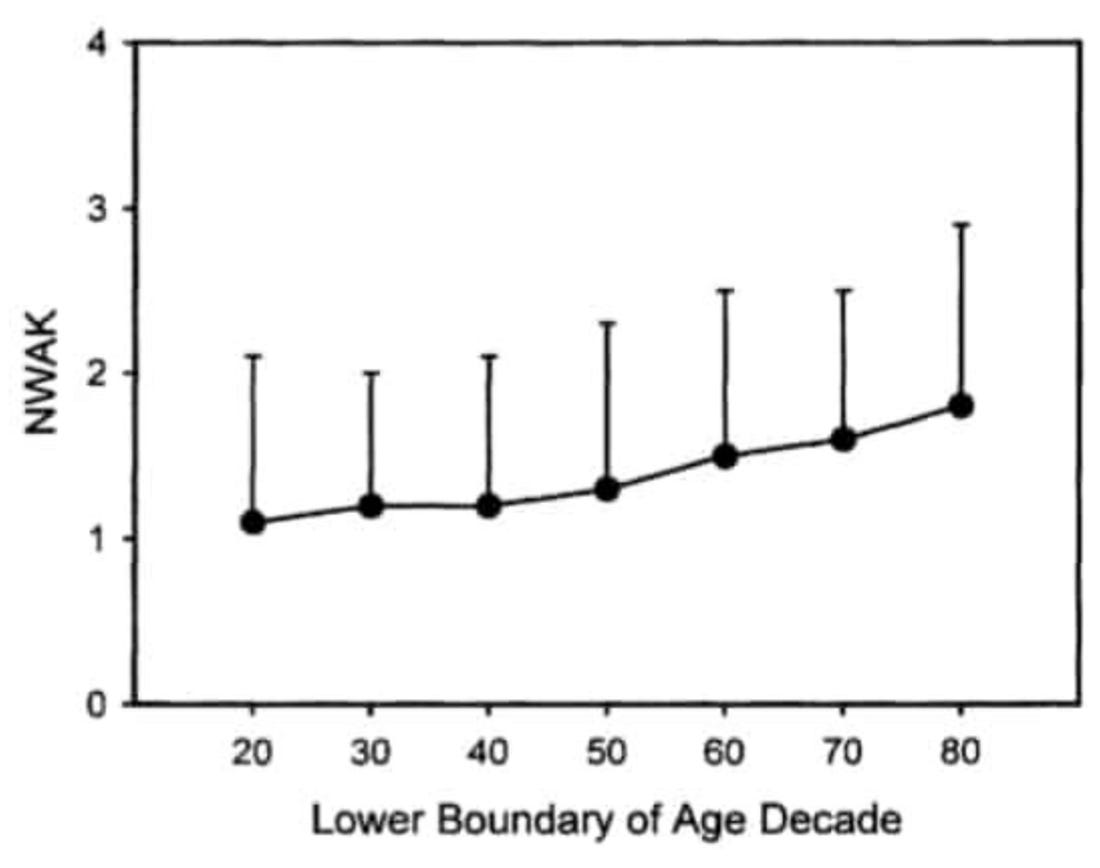
•Likewise, we become more likely to awaken multiple times each night (e.g., due to age-related incontinence):
Given that the elderly are the most vulnerable to deficient sleep (and the least able to initiate the restorative sleep cycle while sleeping due to things like the development of AD), these changes with age are quite unfortunate and again illustrate why healthy sleep should be prioritized. Sleep DisruptorsUnfortunately, in addition to us not having enough time to sleep, a variety of things in our environment either disrupt our ability to stay asleep, or more insidiously, our brain’s ability to perform the vital functions of healthy sleep while we are sleeping. Some of the biggest offenders include: •Habitually consuming long-acting substances that block our ability to sleep (e.g., caffeine or alcohol). Sleeping PillsBecause of the immense problems our society faces from sleeping issues, a massive “treatment” market exists. Unfortunately, like many things in modern medicine, the more money we put into the problem, the worse it becomes. To illustrate:
The entire scam comes down to the fact most sleeping pills are sedatives, not sleep aids.
What this means is that once you take them, you are no longer
conscious, but since this is done through sedating the brain, its
ability to initiate restorative sleep functions is greatly impaired. As a
result, people who take sleeping pills effectively have greatly reduced
sleep, and in turn, are both tired throughout the day (because they did
not have a restorative night of sleep) and are at high risk of
developing a wide range of health issues associated with poor sleep. Most prescription sleeping pills (e.g., Ambien) are classified as “sedative hypnotics” and are fairly similar to the benzodiazepine medications commonly used for anxiety (e.g., Valium). The problem with these drugs is that they are highly addictive, but unfortunately, despite the fact they are only supposed to be used in the short term, individuals typically end up being permanently on them (at which point they can’t withdraw from them). Conversely, over the counter sleeping pills (e.g., Benadryl or Unisom) are typically antihistamines, and unfortunately are also sedatives that damage the sleep cycle (e.g., I once had a medical student who habitually used Unisom and then had to drop out because they gradually became psychotic). Note: alcohol has a similar mechanism to benzodiazapines, which may explain why it is an addictive sedative that inhibits the sleep cycle. Gamma-Hydroxy-ButarateWhile most of the sleeping medications are unsafe and ineffective drugs that are best avoided, one actually worked and frequently produced miraculous results. In turn, I know of numerous cases where my colleagues prescribed it to chronically ill patients with challenging conditions (e.g., non-restorative sleep is one of the classic symptoms of fibromyalgia) who almost completely recovered once they received it. That
drug, originally developed in 1874, is gamma-hydroxybutyrate, and in
1964, it began to be marketed in Europe as an intravenous anesthetic but
never quite caught on due to its unusual properties. On one hand, it is
an ideal anesthetic as: Over the decades that followed, a wide range of research was done on this substance, where it was discovered it had a variety of other extraordinary properties and very low toxicity (e.g., it metabolized to succinate and then water within the mitochondria, its LD50 was 4.28 grams/kg, no deaths have ever been conclusively attributed to it, and when humans have been kept asleep for 24 hours on it or rats for 5 days, they recover immediately once it wears off). The
most apparent benefit was that it was a powerful (and consistent) sleep
aid that immediately put the recipient deep into the sleep cycle,
resulting in the benefits of those cycles being restored for many who
had previously lost them, and the individual waking up feeling
completely refreshed and energized. Furthermore, it frequently could
allow people to feel fully refreshed after just a 3-4 hour sleep, was
unlikely to be addictive, and did not suppress the reticular activation
system. As scientists (and then members of the public) began exploring the drug, according to Ward Dean MD (who provided extensive references to support his claims), they found a variety of benefits from GHB including: •It
dramatically increased the levels of growth hormone (e.g., 2.4 grams
given intravenously, in 30 minutes, caused a 16-fold increase in GH
levels). As growth hormone heals and repairs the body (but greatly
declines with age), this resulted in many previously frail elderly
patients on GHB having significantly increased strength, stamina, muscle
mass, and function, while in younger patients, significant improvement
was seen in their healing from musculoskeletal injuries. •It produced remarkable results in the treatment of a variety of addictions, particularly opioids (e.g., see this study), alcohol (e.g., see the results of this study), and benzodiazepines, along with helping mitigate the withdrawals from each of these substances. Conversely, GHB was not addictive. •It increased dopamine levels within the substancia niagra (thereby counteracting the effects of Parkinson’s disease). •It aided childbirth by relaxing the mother, dilating the cervix, and protecting the fetus from respiratory depression (which for context revolutionizes labor and delivery). •It had a variety of aphrodisiac effects, such as making people much more comfortable with sexual intimacy, dramatically increasing their sensitivity to touching or being touched, improving male erectile capacity and premature ejaculation, and increasing capacity for female orgasms. •Helping
individuals address subjects they are otherwise inhibited from
exploring during therapy (thereby allowing therapeutic breakthroughs to
happen). GHB was also found to be particularly helpful for couples
therapy. •It temporarily helped with anxiety but without many of the side effects seen with benzodiazepines. Similarly, in France, it was frequently used by students who had to pass an exam or give a public presentation. Given these remarkable benefits and the decades of research supporting its use, why has no one ever heard of it? The Ivermectin of Sleep MedicinesIn
this publication, I have tried to illustrate how frequently the medical
industry recruits the public relations (PR) industry to concoct a
campaign that guarantees them lucrative profits at the expense of
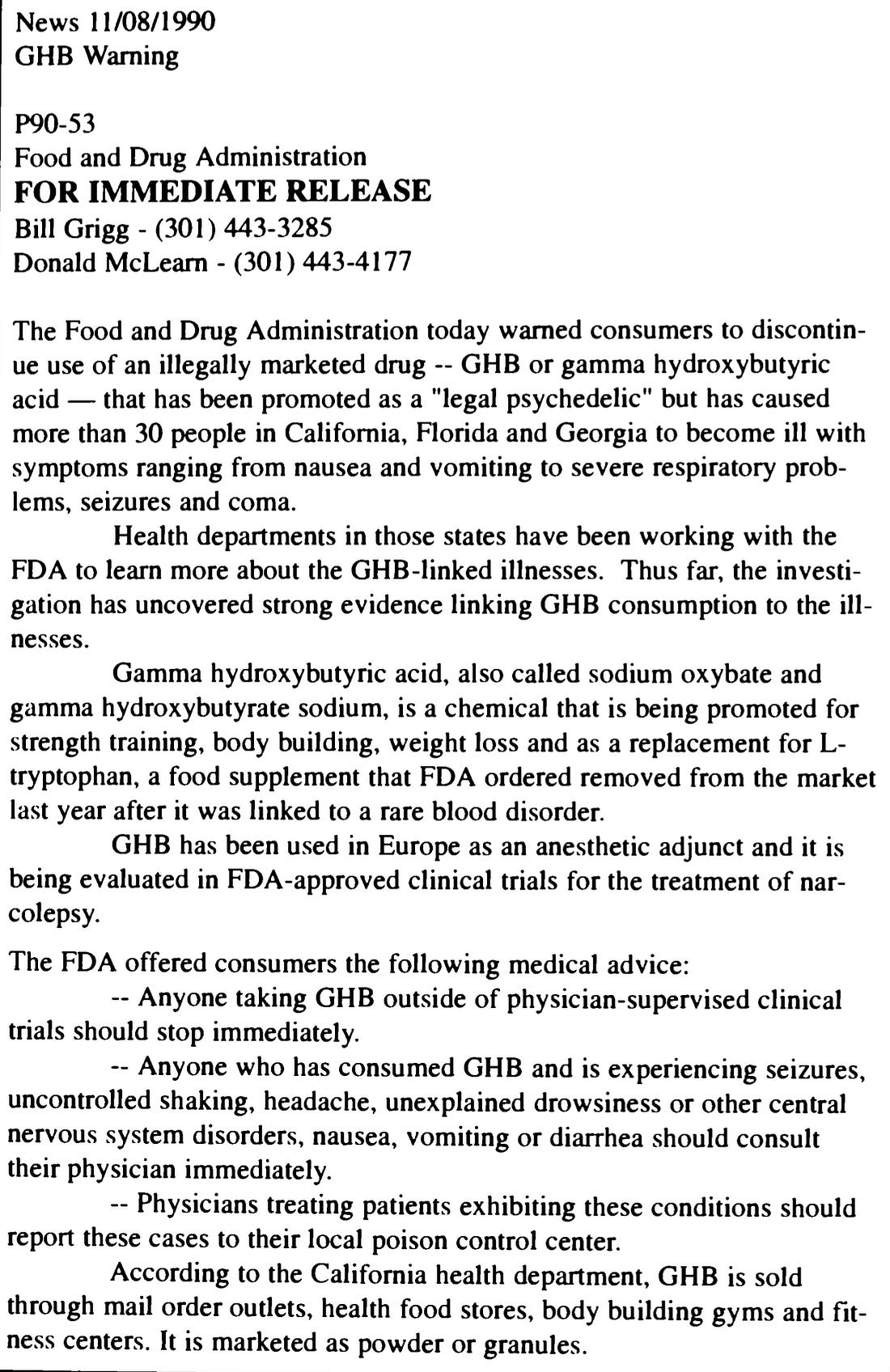
everyone’s health. Likewise, as many of you know, throughout COVID-19, the FDA covered up the clear and unambiguous evidence demonstrating the benefits of ivermectin for COVID-19, creating a hysteria about it (and hydroxychloroquine’s) dangers despite them both being incredibly safe drugs, as well as doing all that it could to block ivermectin from being used in the USA (which was later defeated in court). In the case of GHB, in the early 1990s, it began entering the USA as a supplement (largely due to bodybuilders recognizing the value of it increasing growth hormone in the body). Before long, the FDA decided they needed to stop it, and became very interested in publicizing the adverse reactions that occurred to it, and in no time, discovered 57 calls to poison control about it (which the CDC heavily publicized), including 9 which resulted in ICU admissions (but 0 of which are fatal). This in turn, is very similar to the epidemic of poison control calls for ivermectin and hydroxychloroquine deaths we saw throughout COVID-19 (all of which were later shown to be a hoax—for example, the photos of people lining up at the ERs that were supposedly overloaded with ivermectin poisonings were actually old images of individuals lining up for COVID-19 vaccines). Note: one of the unusual properties of GHB is its short half-life (it typically wears off in 3-4 hours). Because of this, individuals who take a high dose of it (especially if it is combined with alcohol or a benzodiazepine) will fall into a deep slumber with slowed but expansive breathing they cannot be woken from until the drug wears off (which can be mistaken for a coma). In turn, there were many cases of individuals passing out on GHB, and then being brought to the hospital by panicked relatives and then briefly intubated (by doctors who did not understand what was going on and following protocols intubated a non-responsive patient), including instances where someone woke up fully alert as they were about to be intubated and leaving (along with at least one case where they were then forcefully intubated). In response to this “epidemic” the FDA decided to release an urgent press release.
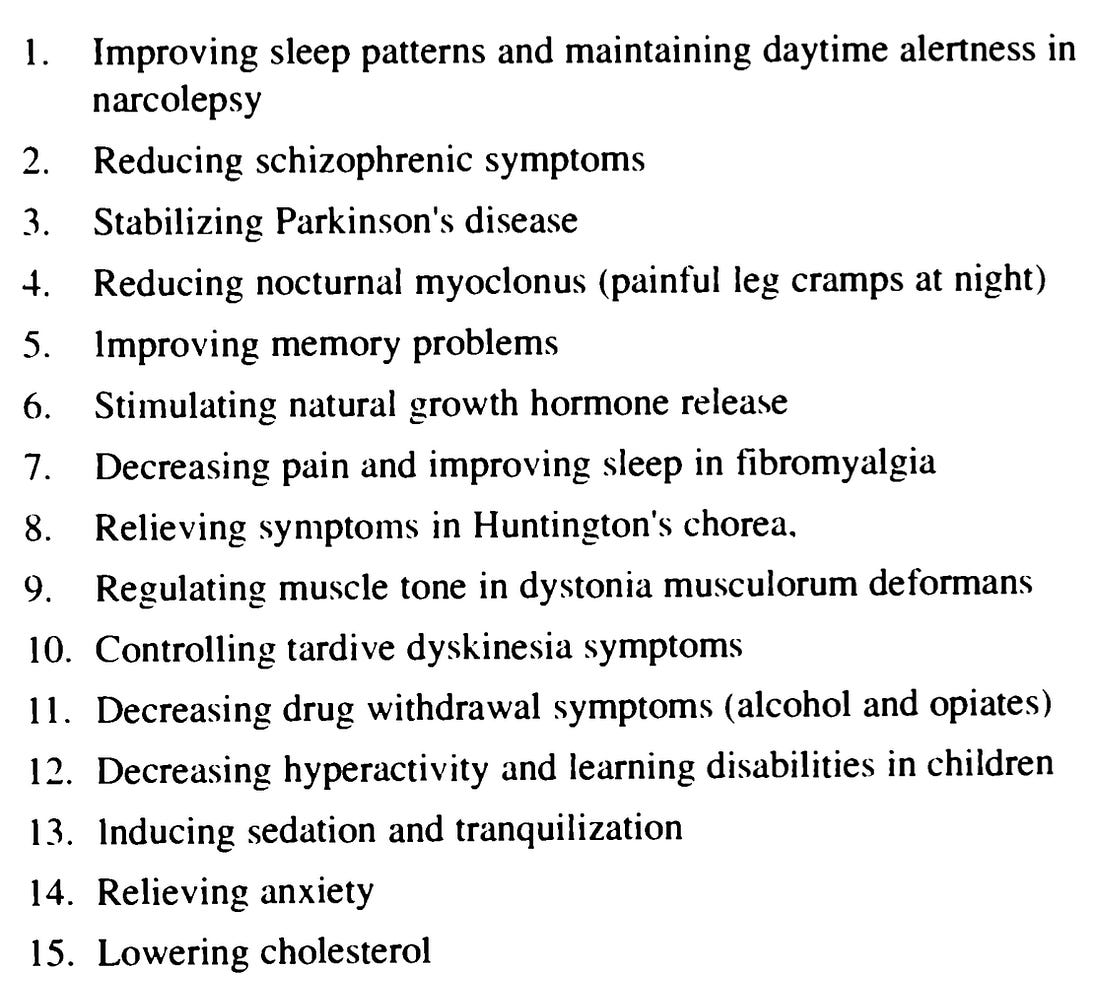
Then on the basis of the authority “bestowed” by this press release (which was full of deceptive inaccuracies), the FDA banned GHB in the country, threatened compounding pharmacies into no longer supplying it, and began raiding people who were supplying it (which they did not have the legal authority to do). Many of these arrests eventually went to the courts, where the FDA engaged in a series of highly unscrupulous tactics. For example, when attempting to prosecute individuals for supplying GHB, they argued that there was “no evidence” GHB had any valid use or had any evidence of safety, but simultaneously, they refused to let the courts admit the decades of evidence arguing otherwise or the fact there were 15 investigational new drug applications which had been submitted to them for GHB (each of which indicated a lot of that evidence actually existed). For reference, those INDs were for:
Note: this is similar to how there was “no evidence” ivermectin worked for COVID-19 despite the fact dozens of trials had proven otherwise. Because of how egregious the FDA's tactics were (e.g., prosecutorial misconduct, withholding evidence from the defense, lacking a legal basis for the prosecution, entrapment, or illegal searches and seizures), the higher courts gradually sided with the defendants and began overturning the convictions. The FDA in turn, switched to trying to persuade the state legislatures to outlaw GHB (as politically it was not possible for the FDA to do so at a Federal level). Note: at the same time this was happening, the FDA was also silencing thousands of SSRI antidepressant victims (the recently released Prozac was one of the most complained about drugs in FDA history), silencing its own employees who tried to speak out, producing fraudulent research to protect the drugs and defying Congressional oversight of their conduct with the SSRIs. I previously wrote an article documenting that saga because I felt it represented one of the best case precedents to predict what they will do with the COVID vaccines. Likewise, as I’ve shown throughout the DMSO series, despite clear evidence DMSO safely treated a variety of debilitating conditions medicine could not help, the FDA fought for decades (including against Congress) to keep DMSO away from the public (and ultimately only “lost” because of a law legalizing all natural supplements). As Rohypnol (“Roofies”) had recently entered the United States and fear was beginning to build over its use as a date rape drug (since it both made the recipient unable to resist the assault and likely to forget it), the fear of Roofies was juxtaposed onto GHB. In turn, the media began trumpeting that America was facing a wave of rapes from a silent, odorless, and colorless drug that made one helpless to resist or even remember sexual assault. In parallel, these (likely focus-group tested) words began flooding those stories about GHB: "dangerous," "potentially lethal," "hallucinogenic," "addictive," "illegal," "designer," "date-rape" "drug." Before long, a few young women were identified who had been date-raped while on GHB and then died afterward from the drug's side effects. The media did all that it could to fan the hysteria (e.g., see this Time article or this San Francisco Chronicle article or consider these patently false quotes):
Note: one of the most extraordinary ones was the Tennessee Bar Association publishing an alleged affidavit from the medical examiner who performed Elvis’s autopsy claiming GHB killed him (although once questioned, they stated it was just an “academic exercise”). Using
this fear campaign, the FDA gradually convinced individual states to
ban it, and in 2000, in honor of two GHB victims, Congress passed the “Hillory J. Farias and Samantha Reid Date-Rape Drug Prohibition Act of 2000." That law made GHB a Schedule I drug (whereas cocaine for example, is a Schedule II drug), thereby bypassing the protections GHB had from the 1994 DSHEA Act
(as GHB is produced naturally within the body and found in small
amounts within meat and wine). Remarkably however, the (“emergency”) law
also included a special exemption for a pharmaceutical preparation of
GHB, which was instead made a schedule III drug (which violates the
entire basis for the scheduling as something can only be a schedule I if
there is no accepted medical use for it).
Note: Rohypnol (which was never brought to the market in America but was in many other countries), thanks to Roche remains a schedule IV drug (like Valium and Xanax) and is not mentioned in any of the state or Federal anti-date rape drug laws that swept through America. In looking at these events, there are three important things to take note of. First, the entire epidemic was made up of: •A safety database
(used for monitoring these types of things) found GHB accounted for
less than 0.1% of the drugs mentioned in Emergency Department reports. •A 2010 literature review determined that GHB had been detected in between 0.2-4.4% of reported sexual assaults and hence was not causing the rape epidemic the media’s hysteria had suggested. Note: the most detailed account I have found about the (tiny) GHB epidemic can be found here. Second, it didn’t make any sense as: •If
GHB actually was an effective date rape drug, the last thing you would
want to do would be to widely advertise it to potential rapists.  Note: much of the previous two sections were sourced from the book Dean Ward M.D. wrote about GHB, some of which can be found in a shorter statement he made. The AftermathBecause of this debacle, it became much more difficult to get GHB, and many leading integrative doctors at the time were disgusted with the FDA as they saw how much GHB benefitted their patients and treated a variety of immensely challenging illnesses. For example, one of my (somewhat-renowned) colleagues is fairly left-wing and reflexively denies the notion any type of coordinated conspiracy could ever exist, but even he is outraged over what happened with GHB and believes the stories of GHB rapes were a complete hoax. In
my own case, I periodically have patients request it from me, and I
sadly have to explain that were I to help them obtain it, I could get in
far more trouble than if I were to become a humble cocaine dealer.
However, while GHB was outlawed, the pharmaceutical preparation, sodium oxybate (Xyrem) was not. Since strong evidence exists to support the use of GHB for many other conditions (e.g., it's a safe and highly effective treatment for alcohol addiction and data shows it cures spasmodic dysphonia—the condition affecting RFK Jr.’s voice), many people have tried to get the FDA to change their position that it’s just a “dangerous date-rape drug” over the years. Consider for a moment what happened with fibromyalgia (a condition which is conventionally incurable and affects at least 4 million Americans):
Note: the only other thing GHB has been approved for (in 2021 after years of lobbying) is the treatment of idiopathic hypersonmnia, a condition similar to narcolepsy. Since
GHB is easy to synthesize and it essentially allows people to become
drunk without the hangover (while simultaneously functioning as an
effective aphrodisiac), it became very popular in the rave scene (where
to some extent, it is still used). Likewise, since some patient
populations who are dealing with significant challenges (e.g., due to
PTSD) find GHB greatly helps them, I periodically hear of them finding a
way to get it. “I have seen a few people who repeatedly used it become somewhat addicted to it.” “I’ve never had an issue with it.” “It is incredibly helpful for sleep, so I use my limited supply when I really need to be well-rested and clear-headed the next day.” “It is a remarkable drug, but I have seen it cause memory loss, addiction, airway issues, and mood depression in people who use it so it needs to prescribed appropriately.” “The growth hormone release is a big deal.” “Make sure you never use it while driving.” Note: many of these also match what Ward Dean M.D. believed. Conversely, when I’ve looked into anonymous online reports, I’ve found many had remarkably positive experiences, while others reported negative experiences which while bad, were not as bad as the things I often see the traditional sleeping pills cause, but nonetheless indicate that GHB needs to be used responsibly under the supervision of a doctor who what they are doing. For this reason, it is my sincere hope the our new FDA will consider creating a pilot program to make GHB available to patients with insomnia under a strict monitoring and verification program (e.g., using AI to ensure only the patient is using the prescription and doing so in a 100% safe manner), as were this to be done, it would be much safer than the existing options being used and transform the lives of its recipients. Overall, one of the most extraordinary things about the GHB saga is that its many of benefits discovered over the decades of research it received were then subsequently discovered by the sleep research community to result from healthy sleep. This again illustrates how often the research we really need already exists but was simply buried due to it being inconvenient for industry. Fortunately however, now that we are at last in an era where forgotten medical truths are being unearthed, more and more are learning about them—for example, recently Joe Rogan and Jimmy Dore discussed the GHB story in front of millions of listeners: More than anything else, I believe the GHB story demonstrates the importance of not being overly biased. For example, while many doctors hold a strong prejudice against any “natural” (e.g., non-drug) therapy, I am the opposite and typically avoid using pharmaceutical drugs because of how frequently I find their harms outweigh their benefits. Nonetheless, I periodically find extraordinary drugs (e.g., DMSO) I give a hard look at and end up using throughout my medical practice. Sadly, as the war against ivermectin showed the world, the primary motivation behind most of medicine is money, and as a result, whenever a true miracle drug is discovered (that competes with existing drugs), medicine moves to bury it, regardless of how much evidence there is in support of it. Sleep HygieneWhile GHB is challenging to obtain (options are discussed further below), there are also many other options for improving sleep. One of the most tried and true ones is to change the signals your body receives so it can go to asleep on its own. Briefly, three processes are at work:
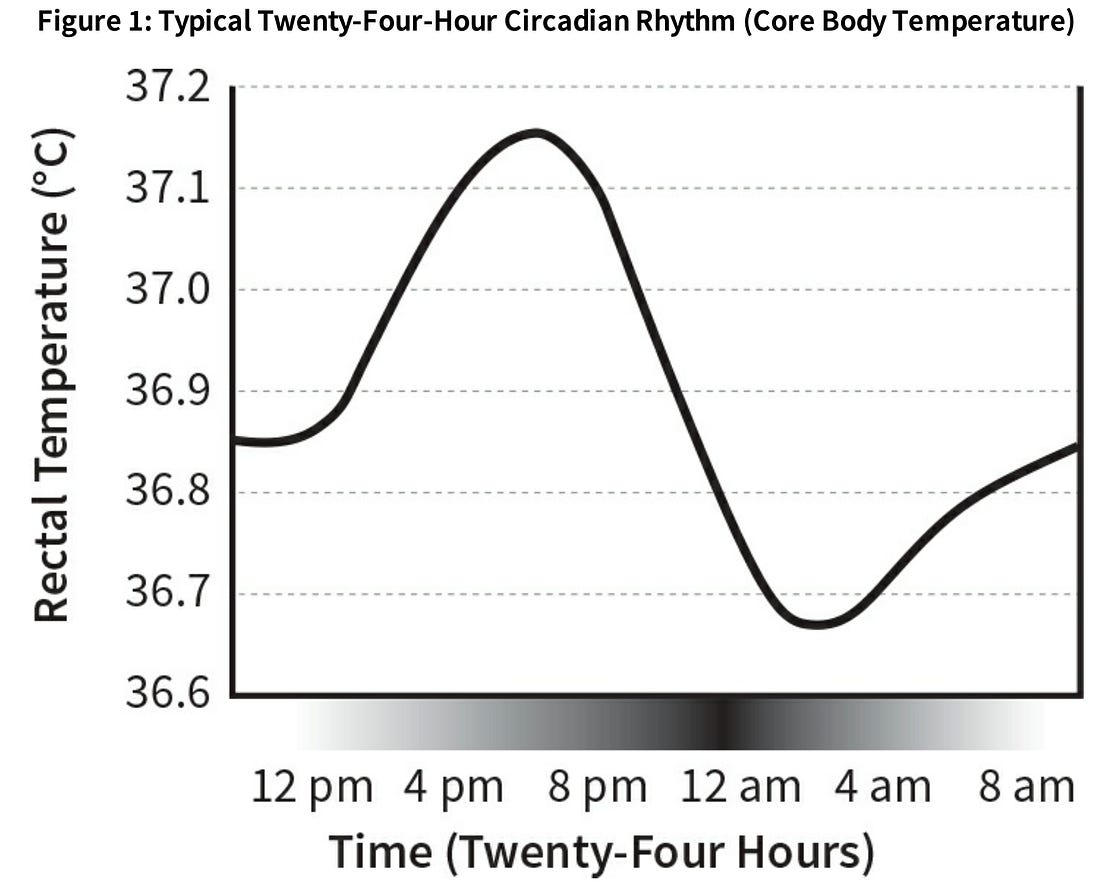
This rhythm is self sustaining, signals to the body when to go to sleep, and also responds to environmental cues. Because of this, the ideal thing is to go to sleep at the same time each day and have the daily signals your body receives be consistent in their timing and match those that would tell it to go to sleep at the correct time (e.g., at 10pm each day). Unfortunately, modern life continually prevents that from happening, and as a result, we often get signals from our circadian rhythm to be asleep when we should be awake. 3.
Sleep is an active energy intensive process. Because of this, if the
drive for sleep is weak and significant barriers to sleep exist (e.g.,
age related damage to the parts of the brain which initiate sleep), it’s
often not possible (or quite difficult) to get to sleep, which in turn
creates a downhill spiral (because deficient sleep further worsens the
brains ability to maintain its health). Treating insomnia hence is a product of improving one or more of these and hoping that gets you to sleep. Caffeine and Alcohol:Both caffeine and alcohol are highly disruptive to sleep. In the case of caffeine, it works by blocking the adenosine receptors in the brain (hence eliminating the pressure you feel to be tired as a result of the brain having built up metabolic waste products during the day it needs sleep and the gylmphatics to clear out). In the case of alcohol, like sleeping pills, it functions as a sedative which is highly disruptive the actual sleep cycle (hence why people wake up not feeling clear in the head after a night of drinking and why drinking greatly impairs your ability to memorize whatever you’ve studied). Note: at a young age, I noticed each of these substances negative impact the health of the adults around me, so I avoided them completely, and I believe that gave me a major leg up in life. The important thing to understand about each substance is that it takes a while for the liver to metabolize and eliminate them, and furthermore, that the rate of elimination varies person to person. Because of this, people often still have the substances active in their blood stream at the time they are trying to get to sleep (e.g., slower metabolizers are kept awake in bed by an afternoon cup of coffee, while moderate metabolizers have their sleep disrupted by an evening glass of wine). Furthermore, for most people liver metabolism declines with age (which is another reason why sleeping issues are so prevalent in the elderly). Lastly, one of the most intriguing data points I’ve seen about the effects of caffeine came from this NASA study:
Temperature:Note: I know someone who shared with me that the most restorative period of their life was when they spent the winter in a snowy mountain cabin without gas or electricity, and that each night they went to sleep in front of a fire (so they didn’t freeze), then woke up in the middle of the night from the cold (because the fire went out) at which point they restarted the fire and went back to sleep. While this is a bit extreme, it helps illustrates how different modern life is from what the human body experienced throughout most of human history. One of the most consistent signs in the environment to sleep is the temperature dropping at night. For this reason, people often find cooling the body (which warm baths ultimately do once you get out as they bring core blood to the surface which is then cooled as the bathwater evaporates off your skin) helpful for putting them to sleep. Likewise, the body’s temperature drops by 1-2 degrees when you sleep, and people often find sleeping in a cooler room helps them get to sleep (whereas many, myself included) have a great deal of difficulty sleeping in hot rooms (so I’ve learned to make sure I never run into this issue when I travel). Because of this, people struggling with insomnia are often advised to make their rooms colder (e.g., according to Walker, assuming standard bedding and clothing, the ideal bedroom temperature for sleep is around 65 degrees F° [18.3°C]). Note: one of the most interesting approaches to overcoming the temperature barrier for sleep was a study that found using a customized suit to externally drop people’s temperature made it much easier for them to sleep (especially in the elderly). Since that time, a variety of devices have been made which replicate this process and many report significantly improve sleep. Light:Your
brain evolved to have the light present in the early morning (blue)
wake you up, while the light present at the end of the day (red) signals
you to sleep. Since we are continually exposed to blue light (most
electronic screens give them off—which I believe was done intentionally
to make them more addictive), we have widespread issues with sleep cycle
dysregulation (as blue light stops the pineal gland from secreting
melatonin). To address the unnatural light issue, people suggest: •Using blue light filters on all electronic devices. I think f.lux is
the easiest option for computers, while with cell phones, a variety of
apps exist (however, the default settings in the phones typically do not
remove blue light from the screens). You can also put blue
light-blocking material directly on screens or wear blue light blocking
glasses. •Change the lighting in your house. Most people believe halogen lamps and incandescent bulbs are the best options, while fluorescents are the worst, followed by LEDs with a low amount of blue light (many have a lot of blue light). Some people like to use red lights in the house at night too. Unfortunately, in recent years there has been a gradual push to phase out these healthier lights and replace them with unhealthy energy efficient ones (which has made incandescent bulbs more difficult to obtain). Note: my favorite lighting option I ever came across was the traditional sodium-vapor lamps (the orange street lights). Unfortunately, these are gradually being replaced with toxic LED street lamps that emit large amounts of blue light (which, amazingly, even the AMA said was a bad idea). •Do everything you can to reduce the light in your room (e.g., no electronics that blink) and, if possible lightproof everything (e.g., use effective blackout curtains that can entirely block the light in each room). I have incredible difficulty sleeping in poorly light-proofed rooms, which is one of the primary reasons I do not travel as much now. •If your circadian rhythm has been disrupted (e.g., from traveling to another time zone), having melatonin a few hours before bed can help reset your circadian rhythm to the correct time. Note: many melatonin supplements on the market do not contain the melatonin they claim to. Additionally, we have observed that long term continual usage of melatonin can lead to a variety of other problems, something we suspect is due to the pineal gland becoming dysregulated (due to an excess of melatonin in the system) and hence no longer performing its normal secretion of melatonin throughout the day. For this reason, I believe melatonin should be applied in a targeted and judicious manner rather than it being a supplement that is always taken for sleep. Behavioral:•You need to have your bedroom be a place that is psychologically associated with sleeping (this can include physical intimacy). Sleep hygienists generally advise minimizing the number of non-sleep-related things in your bedroom (e.g., a TV or desktop computer) and avoiding intellectual activity or social media in your bedroom. •You
need to have a set time to wake up and sleep each day. The body adapts
to a rhythm, and if you keep changing that time, the body has much
greater difficulty falling asleep. •You
need to allow your mind to wind down before sleep. If you can give
yourself at least a 1-2 hour buffer between screens and other mentally
taxing or emotionally stressful activities before sleep, that is ideal.
For many people, this is the single most important thing for ensuring healthy sleep (especially those with unaddressed anxiety), and an area where CBT can be extremely helpful. •Having
more physical activity during the day often makes it much easier for
people to fall asleep at night. I believe this is primarily due to the
increased fluid circulation in the body those activities create. •Use good earplugs at night. Note: sleep specialists often recommend keeping a sleep journal where you log both how much sleep you are getting and what you did throughout the day. When you have this type of a journal it can frequently help you identify what is contributing to your insomnia (e.g., certain foods). Legal Sleep AidsOver the years, we’ve looked at a lot of different options for fixing sleep, and as the years have gone by, my perspectives on what to do for insomnia have evolved. For example, I’ve long believed that sleep apnea is something which needs to be checked for (due to how disruptive it is to sleep) but as the years have gone by, I’ve become of the opinion CPAPs are not an ideal way to treat it (as while helpful for addressing this critically important issue, they are simultaneously disruptive to the body). In the last part of this article I will discuss our preferred approaches for treating sleep issues (e.g., which supplements, devices, and pharmaceutical drugs help), some of the aspects of insomnia I believe are the most important to focus upon (but are not acknowledged within the orthodoxy), my preferred devices for improving sleep (or making partners able to comfortably share beds) along with highlighting a few additional resources for those wishing to learn more about GHB and how to obtain it... Continue reading this post for free in the Substack app
|

No comments:
Post a Comment