“Factual Chaos” at the WHO? Dr. Tedros: Monkeypox Outbreak Is “Among Men Who Have Sex with Men”
The Questionable 99% Estimate



All Global Research articles can be read in 51 languages by activating the “Translate Website” drop down menu on the top banner of our home page (Desktop version).
To receive Global Research’s Daily Newsletter (selected articles), click here.
Visit and follow us on Instagram, Twitter and Facebook. Feel free to repost and share widely Global Research articles.
***
First published on August 1, 2022
Something weird is happening at WHO headquarters in Geneva. On Saturday, July 23, 2022, WHO director-general Tedros Adhanom Ghebreyesus held a press conference in which he declared a Public Health Emergency of International Concern (PHEIC) pertaining to the monkeypox virus.
Dr. Tedros Adhanom Ghebreyesus, took this decision unilaterally against a majority vote of the Second Meeting of the International Health Regulations (2005) (IHR) Emergency Committee (9 against, 6 in favor) held on Thursday, 21 July 2022, in Geneva (from 12:00 noon to 19:00pm Geneva Time CEST), two days prior to Dr. Tedros’s Press Conference which was held on Saturday, 23 July 2022:
“We have an outbreak that has spread around the world rapidly through new modes of transmission…I have decided that the global monkeypox outbreak represents a public health emergency of international concern.”
Did Tedros have the support of his colleagues? Is he in conflict of interest? According to Bloomberg:
“The declaration from Tedros … underscores divisions within the organization over the severity of the threat. The pathogen typically causes flu-like symptoms, followed by a rash that often starts on the face and spreads down the belly. (Bloomberg, emphasis added)
What Bloomberg failed to mention is Dr. Tedros’s Bombshell Statement:
“An outbreak that is concentrated among men who have sex with men”:
“Although I [Tedros] am declaring a public health emergency of international concern, for the moment this is an outbreak that is concentrated among men who have sex with men, especially those with multiple sexual partners.
That means that this is an outbreak that can be stopped with the right strategies in the right groups.
It’s therefore essential that all countries work closely with communities of men who have sex with men, to design and deliver effective information and services, and to adopt measures that protect the health, human rights and dignity of affected communities.
Stigma and discrimination can be as dangerous as any virus.
In addition to our recommendations to countries, I am also calling on civil society organizations, including those with experience in working with people living with HIV, to work with us on fighting stigma and discrimination.
(emphasis added)
Where is the science? What are the implications?
Bear in mind that this was a personalized decision by Dr. Tedros, in defiance of the IHR Committee’ Decision NOT to implement a PHEIC on behalf of 194 member states of the WHO.
Does the above statement constitute an encroachment of the fundamental rights of the LGBT Community which is currently the object of the emergency measures? In the words of the IHR Emergency Committee report cited below: “interventions [are] targeted to this segment of the population [LGBT].”
The calling of a PHEIC has already opened up a Pandora’s box.
Five days after Tedros’ announcement the Mayor of San Fransisco declared a “state of emergency”.
Emergency measures are envisaged in other major US cities.
Before proceeding with a careful review of the WHO report, a few words on the “unspoken history” of this unfolding monkeypox pandemic
Brief Timeline (2017-2022)
 February 2017: Bill Gates’s warning of bioterrorism involving a “synthetic version of the smallpox virus” (Munich Security Conference, February 2017)
February 2017: Bill Gates’s warning of bioterrorism involving a “synthetic version of the smallpox virus” (Munich Security Conference, February 2017)
December 2020: The Expert Planning of A Tabletop Simulation of a Monkeypox Virus Pandemic by the Nuclear Threat Initiative (NTI), a nonprofit organization, founded by former U.S. Sen. Sam Nunn and philanthropist billionaire Ted Turner.
March 2021: The NTI Table Top Simulation which portrays a “fictional exercise scenario of a deadly, global pandemic involving an unusual strain of monkeypox virus” (Munich Security Conference, March 2021)
November 2021: Bill Gates announced possible “Small Pox Terror Attacks” in a TV interview with Jeremy Hunt in early November 2021, Bill Gates warned governments to prepare for simultaneous smallpox terror attacks in 10 airports.
May 5, 2022: Beginning of the alleged “real time outbreak”. First monkeypox reported by the U.K. to the WHO.
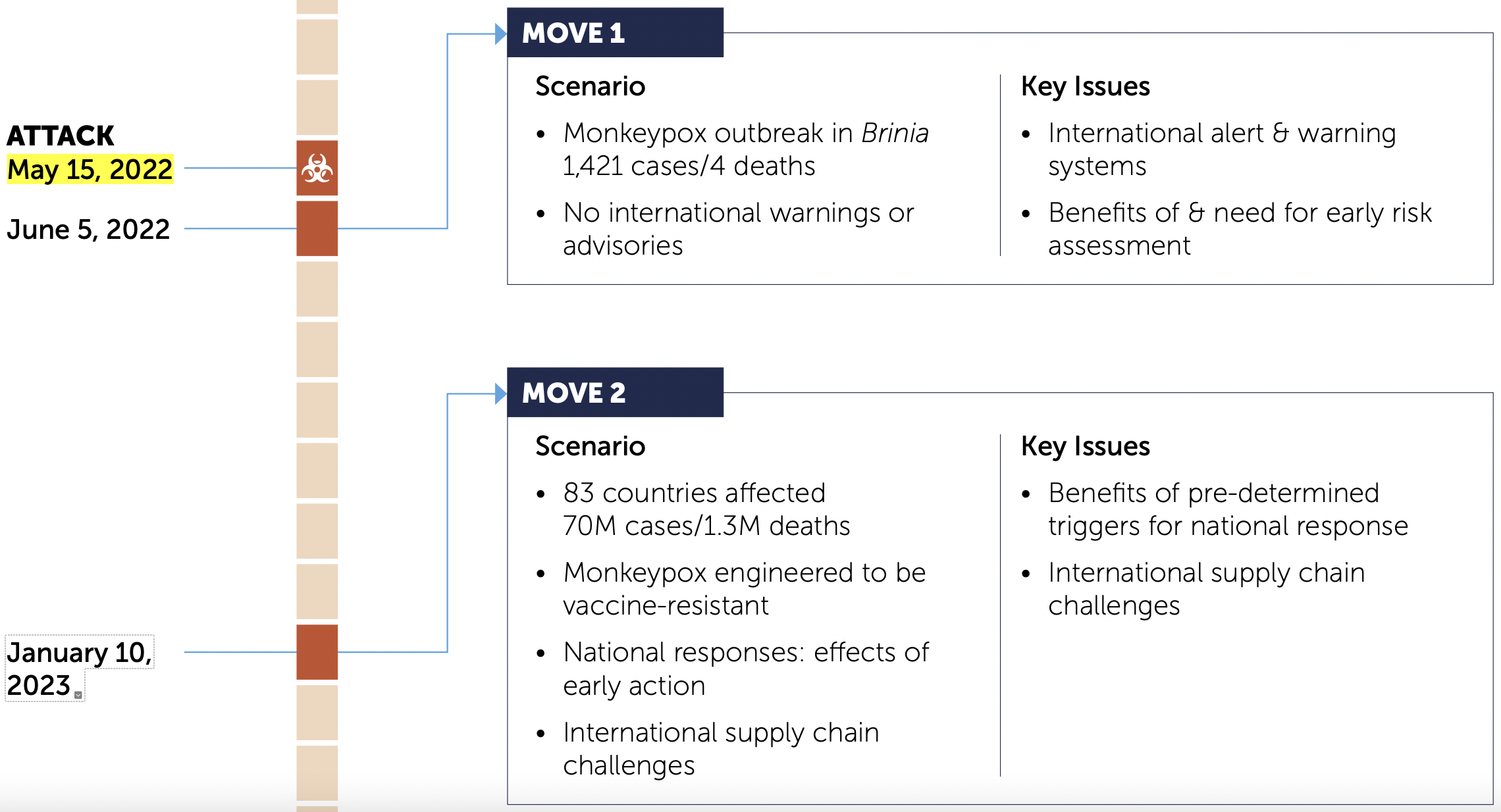
May 15, 2022: Marks the commencement of the monkeypox epidemic in the NTI “Simulated Scenario” (presented to the Munich Security Conference in March 2021), leading up to January 2023 (83 countries affected) with 70 million confirmed cases and 1.3 million deaths. (See below)
July 23, 2022: The WHO Director-General Dr. Tedros Adhanom Ghebreyesus launches a Worldwide Monkeypox Health Emergency (PHEIC)
For further details on the Timeline and Simulated Scenario see:
The Questionable 99% “Estimate”. The Emergency Committee Meeting, July 21, 2022 in Geneva
There is a long history of viral transmission pertaining to the monkeypox pathogen going back to the 1950s. The man to man transmission (MSM) is not corroborated by peer reviewed reports published prior to the May 2022 outbreak.
Below is a review of the published report of “The Second Meeting of the International Health Regulations (2005) (IHR) Emergency Committee” regarding the alleged multi-country outbreak of monkeypox. This meeting was held two days prior to Dr. Tedros’s Press Conference.
The report provides details on the thrust of the WHO Director-General’s decision to launch a Public Health Emergency of International Concern (PHEIC), focussing on the incidence of the monkeypox virus on “bisexual, gay and men who have sex with men”. Of significance, the members of this Committee (21 July 2022) turned down Dr. Tedros proposal to launch the PHEIC.
Below are selected and summarized quotations of a rather long document. Read carefully (the meeting in Geneva lasted for five hours):
“The majority of reported cases of monkeypox currently are in males, and most of these cases occur among males who identified themselves as gay, bisexual and other men who have sex with men (MSM), in urban areas, and are clustered in social and sexual networks.
There has also been a significant rise in the number of cases in countries in West and Central Africa, with an apparent difference in the demographic profile maintained than that observed in Europe and the Americas, with more women and children amongst the cases.
The genome sequence of the virus obtained in several countries shows some divergence from the West African clade.
Representatives of Spain, the United Kingdom, the United States, Canada and Nigeria updated the Committee (in this order) on the epidemiological situation in their countries and their current response efforts. With the exception of Nigeria, the remaining four countries reported that 99% of cases were occurring in MSM, and mainly among those with multiple partners.
The vaccine strategy is targeted and aims to interrupt transmission through post-exposure prophylaxis and pre-exposure prophylaxis among MSM at highest risk.
In the United States, cases of monkeypox are widely distributed across the country, although most cases are concentrated in three large cities. While a few cases have occurred in children and a pregnant woman, 99% are related to male-to-male sexual contact.
In Canada, 99% of cases have occurred among MSM, and the country is taking a broad approach to pre-exposure prophylaxis, given the challenges with contact tracing; and is strongly focused on engagement with community-led organizations supporting key affected populations groups.
Nigeria recorded a little over 800 cases of monkeypox between September 2017 and 10 July 2022 and has seen at 3% case fatality ratio among confirmed cases. Cases are predominantly in men aged 31 to 40 years; there was no evidence of sexual transmission presented. The highest number of annually reported cases since 2017 has been observed in 2022.”
[Members of the Committee underscored the following]:
“The moral duty to deploy all means and tools available to respond to the event, as highlighted by leaders of the LGBTI+ communities from several countries, bearing in mind that the community currently most affected outside Africa is the same initially reported to be affected in the early stages of HIV/AIDS pandemic;
The vast majority of cases are observed among MSM with multiple partners, and, despite the operational challenges, there is the opportunity to stop ongoing transmission with interventions targeted to this segment of the population. Cases observed beyond this population group, including among health workers are, to date, limited; …”
(emphasis added)
Fake Science: Flawed PCR Test “Detects” Monkeypox Virus
The WHO document does not provide relevant sources (pertaining to scientific analysis) nor the data on the alleged monkeypox “confirmed cases”.
What the WHO confirms is that the flawed RT-PCR test was the basis of monkeypox data collection and tabulation (since early May) (see below).
Both the CDC and the WHO endorsed the controversial Real Time Polymerase Chain Reaction Test (RT-PCR) as a means to identifying virus and “detecting the monkeypox pathogen“. A totally absurd initiative.
On June 6, 2022, barely two weeks before Dr. Tedros’s Press announcement, the CDC issued the following advisory:
“This [RT-PCR] assay detects DNA at varying concentrations, providing a qualitative result of either positive, negative, or inconclusive in the identification of Monkeypox virus infections.” (CDC)

It sounds contradictory: on December 31, 2021, the CDC declared that the PCR test was invalid pertaining to SARS-CoV-2 (unauthorized by the FDA). According to the CDC advisory (acknowledging the failures of the RT-PCR test):
“CDC encourages laboratories to consider adoption of a multiplexed method that can facilitate detection and differentiation of SARS-CoV-2 and influenza”.

Let’s not get things mixed up: Versatility of the RT-PCR test. “Anything Goes”.
If you test RT-PCR positive for COVID-19, it may be “mistakenly” tabulated as a “positive” Monkeypox virus infection. How convenient. The PCR positives are then assigned to the monkeypox (“confirmed cases”).
SARS-CoV-2, Influenza, Corona common cold, and now the monkeypox. The PCR test is also being applied to detect the “dangerous” COVID Omicron variants and the BA4 and BA5 sub-variants.
The WHO Report: Invalid Results Derived from Biased Sample?
Were random sample surveys undertaken which corroborate “man to man” (MSM) transmission as outlined by Dr. Tedros in his Press Conference on July 23, 2022? Were women and children included in a random sample procedure?
How is it that MSM male to male sexual transmission is “99% of the cases” in the US, UK, Spain and Canada, while in Nigeria among 800 cases recorded over a five year period, there was not a single case of MSM sexual transmission?
The answer is obvious: the Nigerian data was recorded based on a medical diagnosis of patients over a five year period, whereas the figures pertaining to the US, UK, Canada, Spain were most probably derived from a biased sample, confirmed by a totally invalid PCR Test.
Confirmed in the report: “The 99% of the confirmed cases” were also based on statements by the representatives of those four countries at the IHR Emergency Committee Meeting. Dr. Demetre Daskalakis of the CDC (US) and Dr. Theresa Tam of Health Canada (both advisors to the IHR Committee) were present (see list of members).
Similarly, the report admits that in West and Central Africa there were “more women and children amongst the cases”, whereas as in Europe and North America, the confirmed cases are almost exclusively MSM men.
The report also refers to a monkeypox vaccine specifically for “men who have sex with men, especially those with multiple sexual partners.”
Were these 99% MSM confirmed cases the object of a medical diagnosis, i.e. flu-like symptoms, rashes on the face and the body? Or was it just a PCR test and a biased sample?
The statements in this report are not corroborated. The WHO does not outline its methodology.
From a scientific and statistical standpoint, it does not make sense.
What is the intent?
“Pandemic Preparedness”?
A fear campaign which targets the LGBT community, creating social divisions?
A monkeypox vaccine is already in the pipeline. Governments had already placed orders for the delivery of smallpox vaccines effective against monkeypox.
On May 18, 2022, less than two weeks following the announcement by the WHO, the US government had already signed a contract with Bavaria Nordic consisting of an order of “millions of doses of a vaccine that protects against the virus” (Forbes).
The New England Journal of Medicine (NEJM) Article First Published on Thursday, 21st of July
An important article entitled Monkeypox Virus Infection in Humans across 16 Countries — April-June 2022 was released on Thursday 21st, 2022.

The NEJM study was coordinated by the Share HIV research team at the University of London. No doubt, the NEJM article (published on July 21st) was made available to the WHO as well as to members of the NIH Emergency Committee who were meeting on that same day.
The methodology applied by the Share Group appears to be similar to that of the WHO. The empirical results (confirmed cases) of a biased sample are: “98% of the persons with infection were gay or bisexual men, 75% were White”, using the RT-PCR test applied to the monkeypox virus.
Most of the patients in the “sample” already had a record of HIV and/or sexually transmitted infections (STI). We are not dealing with a random sample.
The authors refer to a “convenience sample” whereby data is collected in collaboration with 43 participating entities in 16 countries most of which are involved in the treatment and research in HIV and sexually transmitted diseases.
Designated patients were recruited for the “sample”, a large percentage of whom already had HIV and/or STI, etc.
We report 528 infections diagnosed between April 27 and June 24, 2022, at 43 sites in 16 countries. Overall, 98% of the persons with infection were gay or bisexual men, 75% were White, and 41% had human immunodeficiency virus infection; the median age was 38 years. Transmission was suspected to have occurred through sexual activity in 95% of the persons with infection. (emphasis added)
The designated patients were submitted to take:
“a laboratory-confirmed monkeypox virus infection defined by a positive result on monkeypox virus polymerase-chain-reaction (PCR) assay in a specimen from any anatomical site”.
It’s “a biased sample” using an invalid test (aka RT-PCR).
Most of the patients who tested positive in the “PCR monkeypox assay were ALREADY de facto HIV and/or STI cases, leading to the “corroborating” FALSE statement pari passu that monkeypox is a sexually transmitted disease.
Related Article
By , July 29, 2022
Note to readers: Please click the share buttons above or below. Follow us on Instagram and Twitter and subscribe to our Telegram Channel. Feel free to repost and share widely Global Research articles.
No comments:
Post a Comment