According to
the American Academy of Pediatrics (AAP), the academic, physical and
mental benefits of returning children to school for in-person learning
outweigh the potential health risks of COVID-19
The AAP and the U.S. Centers for Disease Control and Prevention have issued guidelines for the “safe reopening” of schools
Many parents
wonder whether the guidelines themselves may do far more harm than good
in the long term, as they both unnecessarily frighten and isolate
children from natural interactions
Some of the
basic recommendations found in the CDC and AAP guidelines include
physical distancing on buses and on school grounds, wearing face masks,
screening for symptoms, augmented hygiene and disinfection routines, and
signage and broadcasts reminding students of disease prevention
strategies
Children rarely
become infected and are far less likely to spread the infection than
adults. Scientific evidence also conclusively proves masks do not
prevent infection or spread of viruses
According to the American Academy of
Pediatrics (AAP), the academic, physical and mental benefits of
returning children to school for in-person learning outweigh the
potential health risks of COVID-19.
To that end, the AAP has issued guidelines for the “safe reopening”
of schools. However, many parents wonder whether the guidelines
themselves may do far more harm than good in the long term. One parent
outlines her concerns in the video above.
The U.S. Centers for Disease Control and Prevention has also issued school reopening guidelines1 in anticipation of nationwide reopenings. Unicef2
also supports students’ re-entry into schools, noting that reopenings
should “be consistent with each country’s overall COVID-19 health
response to protect students, staff, teachers and their families.”
American Academy of Pediatrics Calls for School Reopenings
As noted in the AAP’s guidance for school re-entry:3,4
"The importance of in-person learning is well-documented, and
there is already evidence of the negative impacts on children because
of school closures in the spring of 2020.
Lengthy time away from school and associated interruption of
supportive services often results in social isolation, making it
difficult for schools to identify and address important learning
deficits as well as child and adolescent physical or sexual abuse,
substance use, depression, and suicidal ideation.
This, in turn, places children and adolescents at considerable
risk of morbidity and, in some cases, mortality. Beyond the educational
impact and social impact of school closures, there has been
substantial impact on food security and physical activity for children
and families."
Children Rarely Transmit COVID-19
AAP points out that, unlike the influenza virus, SARS-CoV-2 does not
appear to spread easily among children and teens. Indeed, studies from
the U.S.,5 Israel6 and the Netherlands7
have demonstrated that children are far less likely to become infected
than adults, and far less likely than adults to transmit the virus to
others.
In one such study,8 children accounted for just 13% of transmissions within households. Another found9
children under the age of 4 were 47% less likely to test positive for
SARS-CoV-2 infection compared to adults in the same household.
A July 2020 study10
looking at COVID-19 in children and the dynamics of infection within
families found only 0.9% of COVID-19-positive patients were under the
age of 16, and in just 8% of cases did a child within the household
develop symptoms before an adult. Science Daily11 also cites a number of other studies confirming the theory that children are rare disease vectors when it comes to COVID-19:
“In a French study, a boy with Covid-19 exposed over 80
classmates at three schools to the disease. None contracted it.
Transmission of other respiratory diseases, including influenza
transmission, was common at the schools.
In a study in New South Wales, nine infected students and nine
staff across 15 schools exposed a total of 735 students and 128 staff
to Covid-19. Only two secondary infections resulted, one transmitted by
an adult to a child.
‘The data are striking,’ said Dr. [William V.]Raszka.
‘The key takeaway is that children are not driving the pandemic. After
six months, we have a wealth of accumulating data showing that children
are less likely to become infected and seem less infectious; it is
congregating adults who aren't following safety protocols who are
responsible for driving the upward curve.’"
Originally, school closings were based on the premise that the virus
responsible for COVID-19 would behave like other respiratory viruses,
but since it doesn’t, returning children to school is unlikely to pose a
significant risk to health.
“ … the preponderance of evidence indicates that children and
adolescents are less likely to be symptomatic and less likely to have
severe disease resulting from SARS-CoV-2 infection. In addition,
children may be less likely to become infected and to spread
infection,” AAP notes,12 adding that:
“Policies to mitigate the spread of COVID-19 within schools must
be balanced with the known harms to children, adolescents, families,
and the community by keeping children at home.”
Advertisement
Guidelines Promote ‘Institutionalized Isolation’
As mentioned, the CDC has also issued guidelines13
for the re-opening of schools. While the CDC and AAP guidelines are
very similar, the AAP’s restrictions tend to be a bit more flexible.
For example, while both call for social distancing with 6 feet
between each student at all times, the AAP concedes that this may not
always be feasible, and if not, spacing can be 3 feet if students wear
face masks and are asymptomatic. Still, as noted in the featured video,
students are likely to be just as scarred having to follow COVID-19
prevention guidelines as they are staying at home.
While the exact measures vary depending on the age of the students,
some of the basic recommendations found in the CDC and AAP guidelines
include:14,15,16,17
Physical distancing — Students must sit apart on
the school bus; desks must be spaced 6 feet apart and face in the same
direction; floor markings will indicate “safe distancing” from the
teacher’s desk and other areas where lines are formed; plexiglass
barriers will be used in work spaces where physical distancing cannot
be achieved; congregation in shared spaces, including playgrounds and
cafeterias, is to be discouraged for students and teachers alike;
hallways are to be trafficked in one way only to minimize face to face
interaction; students may not share school supplies; nonessential
visitors, including parents, are discouraged from entering the school,
and field trips are to be replaced with virtual events.
Face covering — Teachers and students are to wear face coverings at all times.
Symptom screening — Symptom screening such as
temperature checks should ideally be made by parents before dropping the
child off at the bus stop or at school. Staff or students with a
temperature above 100.4 degrees Fahrenheit will not be permitted in
school.
Disinfection — Hand hygiene, use of disinfectant and regular cleaning of surfaces must be adhered to.
Signage and broadcasts — Signs are to be posted
in various areas, such as entrances and bathrooms, promoting protective
measures to minimize spread of pathogens, and announcements are to be
broadcast over loudspeakers and/or video screens informing students of
the same.
As noted in the featured video, these guidelines amount to
“institutionalized isolation” and fear-mongering that can cause
significant emotional and mental harm to children, especially if
implemented for weeks or months on end.
Humans need physical contact and social face-to-face interactions,
and this is particularly true for children. At best, these remedies
will lead to the creation of a generation of fearful germophobes. At
worst, it may stunt their ability to function normally in social
situations altogether.
Choices Vary Depending on Where You Live
While the AAP and CDC are calling for the reopening of most schools
nationwide, parents may face a variety of choices, depending on where
they live. As reported by USA Today:18
“In just two examples, the Nashville, Tennessee public school system recently offered
parents a choice between sending their children back to school full
time or keeping them at home for online classes, while Fairfax County,
Virginia public schools are making families choose between fully
online schooling or a ‘hybrid’ that combines in-person and remote
instruction.”
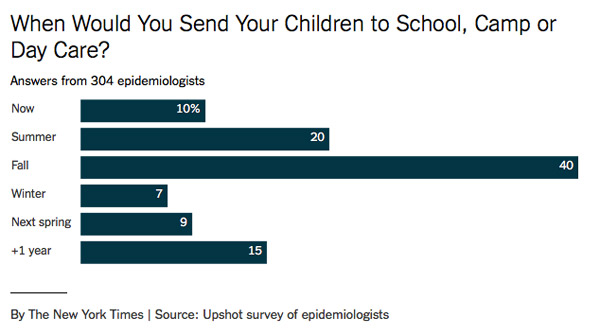
In a June 12, 2020, article19,20
in The New York Times, epidemiologists weighed in on the decision to
send children back to school. Of the 304 epidemiologists that replied
to the New York Times’ survey, a majority — 70% — said they were ready
to send their children back to school somewhere between now and this
fall.
Costs May Have Catastrophic Consequences for School Systems
On top of everything else, there are financial dilemmas to address. As noted in a July 9, 2020, New York Times article,21,22
school budgets that are already stretched thin are facing
million-dollar expenditures if they are to comply with school opening
guidelines:
“Bus monitors to screen students for symptoms in Marietta, Ga.:
$640,000. Protective gear and classroom cleaning equipment for a small
district in rural Michigan: $100,000. Disinfecting school buildings and
hiring extra nurses and educators in San Diego: $90 million …
Exactly how much money the nation’s schools need to reopen is a
matter of debate, complicated by the conflicting, sometimes shifting
advice and guidelines that administrators have received from government
agencies and medical authorities …
Regardless of which recommendations are followed, reopening
schools will require changes. An average-size district of 3,700
students can expect $1.8 million in pandemic-related costs for 2020-21,
representing 3 to 4 percent of a typical annual budget, according to an
estimate from AASA, the School Superintendents Association …
But some experts have suggested that much of what schools are
planning for the fall, such as checking students’ symptoms before they
board buses or enter schools, is unnecessary, akin to the type of
‘security theater’ Americans became accustomed to after the terrorist
attacks of Sept. 11, 2001 — reassuring, but often providing only
superficial protection.”
As reported by U.S. News,23
some school systems are already feeling the economic pain from the
shutdown. Both state and local budget cuts are expected in many areas,
some projected to be as high as 25%, due to lost revenue.
In Massachusetts, 2,000 teachers have already been laid off due to
budget cuts, and the National Education Association estimates upward of
700,000 teachers may lose their jobs over the next two years.
Some states are also seeing skyrocketing homeschooling submissions,
which further threatens schools’ funding. In North Carolina, the online
system for filing a Notice of Intent to Establish a Home
School temporarily crashed24 due to the influx of NOIs being filed, according to a July 7, 2020, report by Life Site.25
I personally find this very encouraging as most educational systems
in the U.S. leave much to be desired. While it certainly is an
additional challenge for parents, I am convinced most children will be
far better off home schooled.
Mask Test Reveals Hazardous Carbon Dioxide Levels
Last but certainly not least, many parents worry the wearing of face
masks might jeopardize the health of their child by restricting oxygen
flow and allowing for the buildup of carbon dioxide with each exhale.
There may indeed be something to this concern, and it’s something that
none of the health authorities have addressed.
The Occupational Safety and Health Administration (OSHA), which is
part of the U.S. Department of Labor, requires the oxygen level in a
working atmosphere to be above 19.5%. Anything below that is considered
hazardous to health.
In the video above, which, of course, was banned and removed from
YouTube, Del Bigtree shows a video of a man demonstrating how the
oxygen concentration — when wearing a surgical mask — can easily drop
below OSHA air quality standards.
Bigtree then conducts a simple carbon dioxide test with his
11-year-old son to check the air quality behind a variety of masks.26
Using a testing device that measures carbon dioxide concentrations in
ambient air, Bigtree checks the carbon dioxide concentration behind his
son’s mask.
With an N95 mask on, the carbon dioxide level spikes above 8,480
parts per million (ppm) within seconds. Above 5,000 ppm, OSHA warns
that “toxicity or oxygen deprivation could occur.”
Carbon dioxide levels between 2,000 ppm and 5,000 ppm are associated
with headaches, sleepiness, poor concentration, loss of attention,
increased heart rate and slight nausea. The maximum permissible daily
exposure limit is 5,000 ppm.
Wearing a standard surgical mask, carbon dioxide levels again
reached above 8,000 ppm, although it took longer. Shockingly, wearing a
cloth bandana resulted in carbon dioxide buildup near the nose and
mouth exceeding 8,000 ppm.
Even wearing a clear plastic face shield (without a mask) resulted
in carbon dioxide levels in the 1,500-ppm range, which is associated
with drowsiness and poor air quality.
There Is No Scientific Basis for Most of These Measures
Unfortunately, many have been swept up in the mainstream media
fearmongering that has bombarded us daily for several months, and when
government and health officials encourage shaming and reporting those
who refuse to succumb to irrationality, it only worsens matters.
The scientific evidence is clear on several points, however. We now
know children are not significant vectors of disease, even when they’re
infected. Children are also at virtually zero risk of death when they
develop symptoms.
Even among adults, the infection mortality rate is now down to a median of about 0.25%.27
As Stanford University's disease prevention chairman Dr. John
Ioannidis noted in a June 27, 2020, interview with Greek Reporter:28,29,30
“For people younger than 45, the infection fatality rate is
almost 0%. For 45 to 70, it is probably about 0.05-0.3%. For those
above 70, it escalates substantially, to 1% or higher for those over
85.”
And, as testing continues, and more people are found to be
asymptomatic yet positive, these mortality rates will be driven down
even further. Science also conclusively shows that masks do not protect
the wearer against viral infection and do not prevent its spread to
others.
This evidence was clearly laid out in my interview with Denis Rancourt, Ph.D.
He did a comprehensive review of the scientific literature on masks,
concentrating on evidence showing masks can reduce infection risk,
especially viral respiratory diseases:
“What I found when I looked at all the randomized controlled trials31,32
with verified outcome, meaning you actually measure whether or not the
person was infected … NONE of these well-designed studies that are
intended to remove observational bias … found there was a statistically
significant advantage of wearing a mask versus not wearing a mask.
Likewise, there was no detectable difference between respirators
and surgical masks. That to me was a clear sign that the science was
telling us they could not detect a positive utility of masks in this
application.
We're talking many really [high-]quality trials. What this means —
and this is very important — is that if there was any significant
advantage to wearing a mask to reduce this [infection] risk, then you
would have detected that in at least one of these trials, [yet] there's
no sign of it.
That to me is a firm scientific conclusion: There is no evidence
that masks are of any utility either preventing the aerosol particles
from coming out or from going in. You're not helping the people around
you by wearing a mask, and you're not helping yourself preventing the
disease by wearing a mask.”
Third, we also now know that COVID-19 has not been the devastating
pandemic killer it’s been made out to be. When looking at all-cause
mortality from year to year, Rancourt found the pandemic has not led to
a significant increase in deaths compared to the same time frame in
previous years. To understand why all-cause mortality statistics are
crucial for understanding the impact of this pandemic, please review my
interview with Rancourt.
Clearly, I’m not going to tell you what to do with your children.
The choice to send your children back to school will have to be a
personal one. All I will suggest is to look at some of the statistics
and scientific evidence brought forth in this article.
Look up the references, read the studies. Try to really understand
the data. Chances are, armed with science rather than mainstream media
reports, you’ll be better equipped to make your choice, and feel
confident in doing so.

No comments:
Post a Comment