After old age,
obesity appears to be the most prominent risk factor for being
hospitalized with COVID-19, doubling the risk of hospitalization in
patients under the age of 60
Most COVID-19
patients have more than one underlying health issue. A study looking at
5,700 New York City patients found 88% had more than one comorbidity.
Only 6.3% had just one underlying health condition and 6.1% had none
Obesity also makes you more vulnerable to infectious diseases by lowering your immune function
Elevated blood
glucose levels appear to play a significant role in viral replication
and the development of cytokine storms. The real pandemic here appears
to be dysregulated glucose metabolism; in other words, insulin
resistance
Amassing data
suggest that even when in close, crowded quarters, the infection rate is
rather low, and fit, healthy individuals are more likely to be
asymptomatic than not when testing positive for SARS-CoV-2 infection
According to a January 2019 update by
the U.S. Centers for Disease Control and Prevention, more than 122
million American adults have diabetes or prediabetes1 — conditions which have been shown to increase your chances of contracting and even dying from COVID-19.2,3,4,5,6,7 As noted in an April 16, 2020, report by The New York Times:8
"Obesity may be one of the most important predictors of severe
coronavirus illness, new studies say. It's an alarming finding for the
United States, which has one of the highest obesity rates in the world."
Obesity Appears To Be Independent Risk Factor for COVID-19
After old age, obesity appears to be the most prominent risk factor
for being hospitalized with COVID-19 — doubling the risk of
hospitalization in patients under the age of 60 in one study9 — even if the individual has no other obesity-related health problems. A French study10,11 also found obese patients treated for COVID-19 were more likely to require mechanical ventilation.
Dr. Leora Horwitz, director of the Center for Healthcare Innovation and Delivery Science at NYU Langone who co-wrote the paper12
"Factors Associated with Hospitalization and Critical Illness Among
4,103 Patients With Covid-19 Disease In New York City" — which has not
yet been peer-reviewed — told The New York Times:13
"Obesity is more important for hospitalization than whether you
have high blood pressure or diabetes, though these often go together,
and it's more important than coronary disease or cancer or kidney
disease, or even pulmonary disease."
Most COVID-19 Patients Have More Than One Comorbidity
While obesity
may top the list of comorbidities — underlying conditions that make
COVID-19 worse — investigations reveal most COVID-19 patients have more
than one underlying health issue. A study14
looking at 5,700 New York City patients found 88% had more than one
comorbidity. Only 6.3% had just one underlying health condition and 6.1%
had none.
In this particular study,15 published in JAMA, high blood pressure at 53.1% beat obesity (41.7%) as the No. 1 most common comorbidity among hospitalized patients, followed by diabetes at 31.7% and coronary artery disease at 10.4%.
Co-author Karina Davidson, senior vice president for the Feinstein Institutes for Medical Research told Time magazine:16
"Having serious comorbidities increases your risk … We want
patients with serious chronic disease to take a special precaution and
to seek medical attention early, should they start showing signs and
symptoms of being infected …"
Advertisement
Obesity Lowers Immune Function
According to The New York Times,17
one hypothesis for why obesity is worsening COVID-19 has to do with the
fact that obesity causes chronic inflammation. Having more
pro-inflammatory cytokines in circulation increases your risk of
experiencing a cytokine storm. Obesity also makes you more vulnerable to
infectious diseases by lowering your immune function.18,19,20,21,22,23
As noted in one such study,24
"there is a positive feedback loop between local inflammation in
adipose tissue and altered immune response in obesity." Yet another
scientific review25
pointed out "There is strong evidence indicating that excess adiposity
negatively impacts immune function and host defense in obese
individuals." A 2018 review article further explained:26
"Adipose tissue is now considered an extremely active endocrine
organ that secretes cytokine-like hormones, called adipokines, either
pro- or anti-inflammatory factors bridging metabolism to the immune
system.
Leptin is historically one of most relevant adipokines, with
important physiological roles in the central control of energy
metabolism and in the regulation of metabolism-immune system interplay,
being a cornerstone of the emerging field of immunometabolism.
Indeed, leptin receptor is expressed throughout the immune system
and leptin has been shown to regulate both innate and adaptive immune
responses."
Glucose Metabolism Influences Cytokine Storms
An April 15, 2020, article27 in The Scientist also reviews new evidence28,29 that sheds further light on why obesity and diabetes are such potent risk factors for severe COVID-19 infection.
In a nutshell, higher blood glucose levels appear to play a
significant role in viral replication and the development of cytokine
storms. While the research in question looked at influenza A-induced
cytokine storms, these findings may well be applicable in COVID-19 as
well.
Cytokines are released by your immune system in response to foreign
invaders. They, in turn, act as messengers that instruct other immune
cells to fight the pathogen. In some cases, this immune response goes
into overdrive, resulting in what's known as a "cytokine storm" that can
cause severe tissue damage and lead to death.
A cytokine storm response
is typically the reason why people die from infections, be it the
seasonal flu, Ebola, urinary tract infection or COVID-19. A critical
player in cytokine production is the transcription factor interferon
regulatory factor 5 (IRF5). In mice, genetically eliminating IRF5
protects them from influenza-induced cytokine storms.30
Interestingly, "the inflammatory response to influenza infections is
also known to drive up glucose metabolism," The Scientist reports,31
"in part so that immune cells have the necessary energy to mount a
strong response, and also because the virus needs the sugar to
replicate."
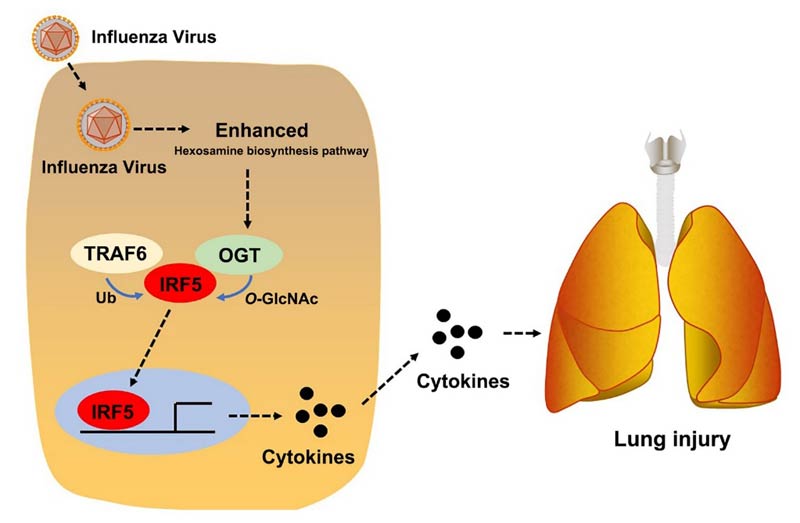
According to researchers at the State Key Laboratory of Virology at
Wuhan University, the hexosamine biosynthesis pathway — a glucose
metabolism pathway — is responsible for activating IRF5-induced cytokine
production in cells and mice. The same pathway is also responsible for
viral replication, they say.32,33,34 As reported by The Scientist:35
"Hexosamine biosynthesis starts with glucose and results in an
end product called uridine diphosphate N-acetylglucosamine (UDP-GlcNAc) …
Liu's team now shows that O-GlcNAcylation of IRF5 is necessary for the
transcription factor's cytokine-producing activity …
The team also showed that patients infected with influenza have
higher blood glucose levels and more O-GlcNacylation of IRF5 than
healthy controls. Furthermore, blood glucose levels correlated tightly
with levels of inflammatory cytokines.
The results show that 'there is a connection [between] influenza
virus infection, enhanced glucose metabolism and cytokine storm, all
linked through O-GlcNAcylation of IFR-5,' Mengji Lu, a virologist at the
University Hospital Essen and a coauthor of the study, writes in an
email to The Scientist …"
In a Science Advances press release, co-author Shi Liu states:36
"We believe that glucose metabolism contributes to various
COVID-19 outcomes since both influenza and COVID-19 can induce a
cytokine storm, and since COVID-19 patients with diabetes have shown
higher mortality."
Insulin Resistance Is the Real Pandemic
So, to summarize, the real pandemic here appears to be dysregulated
glucose metabolism; in other words, insulin resistance, which is
exceedingly prevalent in the U.S.37,38 Insulin resistance, in turn, is a diet-induced condition.
Specifically, processed foods — which are loaded with added sugars,
processed grains and industrially processed omega-6 vegetable oils — are
the primary culprits causing insulin resistance, Type 2 diabetes and obesity, and according to FoodNavigator.com,39 doctors are finally starting to talk about the food industry's role in the COVID-19 pandemic.
"A cardiologist has blamed the food industry for 'normalizing'
ultra-processed junk food as more evidence emerges suggesting poor diet
is the root cause behind increased mortality from COVID-19," FoodNavigator states, adding:40
"In light of the mounting evidence that obesity and poor diet
increases the risk of a severe response to COVID-19 infection, medical
professionals now want the public health message urgently updated. And
this, they warn, means the food industry bracing itself for regulation,
such as bans on advertising and taxes …
Dr. Aseem Malhotra, a London-based cardiologist, told the BBC
that a Government and Public Health England failure to tell the public
to change its diet would represent an act of 'negligence and ignorance' …
For him, the pandemic highlighted that it was in the interest of
everybody, including those in the food industry, to make sure the
population was as healthy as possible."
Malhotra stresses these views in his April 16, 2020, article41
"COVID-19 and the Elephant in the Room," published in European
Scientist. "Obesity and chronic metabolic disease is killing COVID-19
patients: Now is the time to eat real food," he says. Indeed, if our
public health agencies really want to save lives, it's time to get
onboard with nutrition.
"If this is not the time for Britain to reverse its epidemic of
Type 2 diabetes, which as a single condition has been the most costly to
the NHS [National Health Service], then when is?" Malhotra writes.42
"Healthcare systems were already overstretched before COVID-19
because of decades of maldistribution of resources due to 'too much
medicine' combined [with] our collective failure to implement policy
changes to address the root cause of diet related disease — the
unavoidable junk food environment.
The government public health message enhanced by the media to
stay at home, protect the NHS and save lives has been powerful and
effective. Given the speed at which health markers for metabolic disease
improve from dietary interventions, an equally strong if not more
significant population health message should now be to 'eat real food,
protect the NHS and save lives.'
Such implementation backed by policy changes may not just save
hundreds and potentially thousands of lives around the world in the
coming months but given the high likelihood of another international
viral pandemic in the next decade a healthier population and a
subsequently more manageable health service will be much better equipped
to handle what would then be a smaller mortality peak on the next
occasion."
Junk Food Industry Faces Increasing Pressure
This is timely, considering a Corporate Accountability report,43 announced44 April 21, 2020, highlights the "outsized role" of International Life Sciences Institute (ILSI), a junk food industry front group funded by Coca-Cola, plays in shaping nutritional policies around the globe. According to the Corporate Accountability press release:45
"Notable among the findings is that more than half of the 2020
Dietary Guidelines Advisory Committee — the body that informs both
national nutrition policy and how Americans eat and drink — has ties to
ILSI …
The food and beverage industry's role in stymying public health
policy and propagating junk science is also taking on new dimensions
during today's pandemic. The surge of diet-related disease behind one in
five deaths annually, is putting hundreds of millions of people at high
risk of severe illness from COVID19.
'For decades, Coke, its competitors, and its surrogates like ILSI
have trafficked in junk science, co-opted public officials, and bullied
advocates like myself …' said Dr. Esperanza Ceron … 'But we won't be
silenced. Too much is at stake' …
'It's time for Coke to put something more on ice than its soft
drinks,' said Corporate Accountability Research Director Ashka Naik, a
co-author of the report.
'Coke is telling investors it cares about public health on the
one hand, but funds ILSI to block public health safeguards on the other.
Its misleading of investors and consumers is a liability that will only
grow.'
A resolution … calls on Coke to come clean with its shareholders
about its public health harms and liabilities. It would require a
public, independent audit of how the corporation is contributing to the
crisis of diet-related disease, whether through its products, its
marketing, its political interference, or junk science."
Data Show COVID-19 Isn't a Significant Threat
In the featured Fundamental Health podcast above, Dr. Paul Saladino
interviews Dr. Kirk Parsley about the lifestyle factors that are
contributing to the high COVID-19 caseload in the U.S.
Saladino cites findings46
showing that of the roughly 4,800 crew on the U.S. aircraft carrier USS
Theodore Roosevelt, 660 had tested positive for SARS-CoV-2. (As of
April 23, when all of the crew had reportedly been tested, 840 tested
positive.47) However, as noted by Saladino and reported by Business Insider,48 60% were asymptomatic, meaning they had no symptoms. Only one crewmember has died,49 and as of April 23, none were in intensive care.50
Similarly, among the 3,711 passengers and crew onboard the Diamond
Princess cruise ship, 712 (19.2%) tested positive for SARS-CoV-2, and of
these 46.5% were asymptomatic at the time of testing. Of those showing
symptom, only 9.7% required intensive care and 1.3% died.51
Military personnel, as you would expect, tend to be healthier than
the general population. Still, the data from these two incidents reveal
several important points to consider. First of all, it suggests that
even when living in close, crowded quarters, the infection rate is
rather low.
Only 17.5% of the USS Theodore Roosevelt crew got infected — slightly
lower than the 19.2% of those onboard the Diamond Princess, which had a
greater ratio of older people.
Second, fit and healthy individuals are more likely to be
asymptomatic than not — 60% of naval personnel compared to 46.5% of
civilians onboard the Diamond Princess had no symptoms despite testing
positive.
Saladino and Parsley go on to discuss current pandemic response
efforts, such as the recommendation (and in some areas mandate) to wear a
face mask when venturing outside. Both are convinced wearing a bandana
across your face is completely useless, for the simple fact that the
virus is so small it can easily slip through the fabric.
Parsley also reviews the statistics as of April 21, 2020, using Worldometer data,52
showing only 1.7% of American COVID-19 cases require hospitalization,
and of those an even smaller ratio will actually die. Is it really
reasonable to shut down the entire country and place everyone under
house arrest over a 1.7% hospitalization rate?
So-called "COVID-19 cases," by the way, simply means people who have
tested positive using an RT-PCR (reverse transcription polymerase chain
reaction) test, which is used to diagnose an active infection by
detecting the presence of SARS-CoV-2 genetic material.53
Mortality Rates Are Still Vastly Overestimated
The hospitalization is actually bound to be even lower than 1.7% in
real life, seeing how few people have actually been tested. Preliminary
findings54
published April 17, 2020, reveal the actual infection rate in Santa
Clara County, California, is likely to be between 50- and 85fold higher
than the number of confirmed cases.
This is based on seroprevalence data, meaning antibody testing. If
you have antibodies against a particular pathogen, you've been exposed
to it in the past, whether you developed symptoms or not, and you're now
immune to it.
Between April 3 and April 4, 3,330 Santa Clara county residents were
tested for antibodies to SARS-CoV-2 using a lateral flow immunoassay. In
an effort to ensure results were as accurate as possible, they were
adjusted for test performance characteristics using three estimates:
Test manufacturer data
A sample of 37 positive and 30 negative controls tested at Stanford
A combination of both
According to the authors:55
"The unadjusted prevalence of antibodies to SARS-CoV-2 in Santa
Clara County was 1.5% … and the population-weighted prevalence was 2.81%
… Under the three scenarios for test performance characteristics, the
population prevalence of COVID-19 in Santa Clara ranged from 2.49% … to
4.16% …
These prevalence estimates represent a range between 48,000 and
81,000 people infected in Santa Clara County by early April, 50-85-fold
more than the number of confirmed cases.
Conclusions: The population prevalence of SARS-CoV-2 antibodies
in Santa Clara County implies that the infection is much more widespread
than indicated by the number of confirmed cases. Population prevalence
estimates can now be used to calibrate epidemic and mortality
projections."
Randomized antibody tests done in New York show that upward of 20% of
the population in New York have been infected, suggesting that the
virus had spread far more widely than known.56
This is also strong support for a lower fatality rate as previous
inaccurate PCR tests were only done on sick people and there was no idea
how many in the population had been infected. Since more people are
infected, this increases the denominator in the calculation and lowers
the mortality rate calculation.
Blood Pressure Drugs May Worsen COVID-19
Making matters worse, the drugs routinely used to treat
lifestyle-induced afflictions such as high blood pressure, diabetes and
heart disease may also be contributing to adverse outcomes in patients
with COVID-19. According to Reuters:57
"A disproportionate number of patients hospitalized by COVID-19 …
have high blood pressure. Theories about why the condition makes them
more vulnerable … have sparked a fierce debate among scientists over the
impact of widely prescribed blood-pressure drugs.
Researchers agree that the life-saving drugs affect the same
pathways that the novel coronavirus takes to enter the lungs and heart.
They differ on whether those drugs open the door to the virus or protect
against it …
The drugs are known as ACE inhibitors and ARBs … In a recent
interview with a medical journal, Anthony Fauci — the U.S. government's
top infectious disease expert — cited a report showing similarly high
rates of hypertension among COVID-19 patients who died in Italy and
suggested the medicines, rather than the underlying condition, may act
as an accelerant for the virus …
There is evidence that the drugs may increase the presence of an
enzyme — ACE2 — that produces hormones that lower blood pressure by
widening blood vessels. That's normally a good thing.
But the coronavirus also targets ACE2 and has developed spikes
that can latch on to the enzyme and penetrate cells … So more enzymes
provide more targets for the virus, potentially increasing the chance of
infection or making it more severe.
Other evidence, however, suggests the infection's interference
with ACE2 may lead to higher levels of a hormone that causes
inflammation, which can result in acute respiratory distress syndrome, a
dangerous build-up of fluid in the lungs. In that case, ARBs may be
beneficial because they block some of the hormone's damaging effects."
This presents significant challenges for patients and doctors alike,
as there's currently no significant consensus on whether patients should
discontinue the drugs. The Centre for Evidence-Based Medicine at the
University of Oxford in England recommends switching to alternative
blood pressure medicines in patients who have only mildly elevated blood
pressure and are at high risk for COVID-19.
A paper in NEJM stressed the potential benefits of the drugs instead,
saying patients should continue taking them. However, several of the
scientists who wrote that paper have done "extensive, industry-supported
research on antihypertensive drugs," Reuters notes.
Dr. Kevin Kavanagh, founder of the patient advocacy group Health
Watch USA, believes it would be unwise to allow scientists funded by the
drug industry to give clinical directions at this time. "Let others
without a conflict of interest try to make a call," he said.58
Restore Insulin Sensitivity for Long-Term Risk Mitigation
If we want people to survive the next pandemic, whatever that might
be, then improving public health has got to be the No. 1 priority going
forward. Waiting for a drug cure or vaccine is a fool's game.
Health care really needs to start emphasizing strategies known to
improve overall health rather than throwing drugs at symptoms that don't
address the underlying causes. Robust immune function is necessary to
effectively combat COVID-19, and the same is true for all other
infectious disease.
When it comes to improving health, addressing insulin resistance is
truly key, seeing how it's a factor in virtually all chronic diseases.
And, to do that, we need to dramatically cut down on processed foods.
As noted by Dr. Sandra Weber, president of the American Association of Clinical Endocrinologists, in The New York Times,59
"We know that if you do not have good glucose control, you're at high
risk for infection, including viruses and presumably this one [COVID-19]
as well … [improving glucose control] would put you in a situation
where you would have better immune function."
For details on what and when to eat to reverse insulin resistance, see "Want to Defeat Coronavirus? Address Diabetes and Hypertension."
In that article, I also summarize several key strategies for getting
and staying healthy and metabolically fit. For additional COVID-19
remedies and top tips, see my COVID-19 Resource Guide.
For those who desire more in-depth understanding of how you can
become metabolically flexible and eliminate insulin resistance, consider
picking up a copy of my book, "Fat for Fuel."
It goes into far greater detail, providing a comprehensive program that
will help optimize your metabolic flexibility and strengthen your
immune system — both of which are crucial components of health and
disease prevention.

No comments:
Post a Comment