What They Don't Tell Us About Heart DiseaseUnpacking the Great Cholesterol Scam and the Dangers of StatinsStory at a Glance: •There
is a widespread belief that elevated cholesterol is the “cause” of
cardiovascular disease. However, a large body of evidence shows that
there is no association between the two and the real data shows lower
cholesterol significantly increases one’s risk of death. The more I study science, the more I come to see how often fundamental facts end up being changed so that a profitable industry can be created. In the case of heart disease, I very much believe that is the case and in this publication, I’ve tried to expose the erroneous information that predominates our understanding of this subject (e.g., previously I’ve discussed why our model of how the heart pumps blood in the body is incorrect, the forgotten Russian research that shows the heart intelligently controls how blood moves within the body, and how blood pressure management is filled with erroneous premises that exist to perpetually sell medications). Within cardiology, I believe one of the most damaging falsehoods is that cholesterol causes heart disease and that taking statins (or their newer lucrative equivalents), which lower cholesterol, are the key to preventing heart disease. This is because, in addition to those “facts” being incorrect, statins are also some of the most dangerous and widely used pharmaceutical drugs on the market. Cholesterol and Heart DiseaseFrequently, when an industry harms many people, it will create a scapegoat to get out of trouble. Once this happens, a variety of other sectors that also benefit from that scapegoat existing will jump on the bandwagon. Before long, a false belief that harms society becomes an unquestionable dogma that becomes very difficult to overturn because many corrupt parties have a vested interest in maintaining the lie. For example, various easily addressable factors (which often exist in the first place because they benefit an industry) are responsible for the chronic diseases we face in society and our vulnerability to infectious diseases (e.g., the obese and diabetics were much more likely to catch COVID-19). However, by saying all diseases result from insufficient vaccination, it gets all those destructive industries off the hook and creates a huge market for selling vaccines and treatments for these illnesses. Thus, since there are so many vested interests behind the vaccine paradigm, it is very difficult to overturn—despite the fact there’s no evidence vaccines ended the era of infectious disease but the existing evidence does show they are responsible for the massive epidemic of chronic disease that is sweeping our country. In the 1960s and 1970s, a debate emerged over what caused heart disease. On one side, John Yudkin effectively argued that the sugar being added to our food by the processed food industry was the chief culprit. On the other side, Ancel Keys (who attacked Yudkin's work) argued that it was due to saturated fat and cholesterol. Note: a case can also be made that the mass adoption of vegetable oils lead to this increase in heart disease. Likewise, some believe the advent of water chlorination was responsible for this increase. Ancel
Keys won, Yudkin's work was largely dismissed, and Keys became
nutritional dogma. A large part of Key’s victory was based on his study
of seven countries (Italy, Greece, Former Yugoslavia, Netherlands,
Finland, America, and Japan), which showed that as saturated fat
consumption increased, heart disease increased in a linear fashion. Note: the author who unearthed that study also discovered another (unpublished) study from the 1970s of 458 Australians, which found that replacing some of their saturated fat with vegetable oils increased their risk of dying by 17.6% Likewise, recently, one of the most prestigious medical journals in the world published internal sugar industry documents. They showed the sugar industry had used bribes to make scientists place the blame for heart disease on fat so Yudkin's work would not threaten the sugar industry. In turn, it is now generally accepted that Yudkin was right, but nonetheless, our medical guidelines are still largely based on Key’s work. However, despite a significant amount of data that now shows lowering cholesterol is not associated with a reduction in heart disease (e.g., this study, this study, this study, this review, this review, and this review) the need to lower cholesterol is still a dogma within cardiology. For example, how many of you have heard of this 1986 study which was published in the Lancet which concluded:
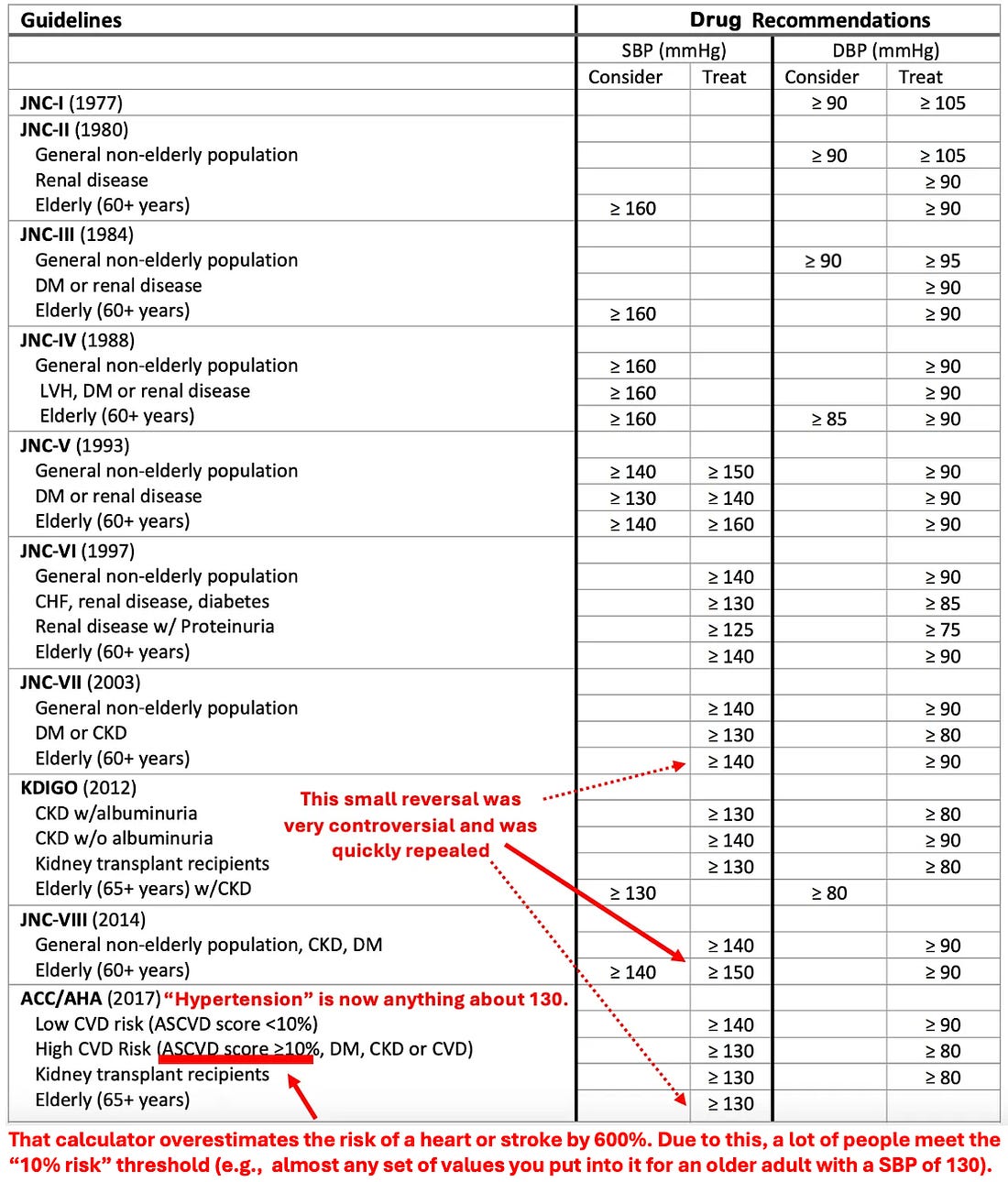
Note: when people are diabetic (which leads to the liver having to process too much sugar) the liver will convert to fat and then create more cholesterol to transport some of that fat. In these instances, many argue the actual issue is an excess of sugar rather than elevated cholesterol levels it causes. Statin MarketingOne of the consistent patterns I’ve observed within medicine is that once a drug is identified that can “beneficially” change a number, medical practice guidelines will gradually shift to prioritizing treating that number and before long, rationals will be created that require more and more of the population to be subject to that regimen. For example, consider what happened with blood pressure:
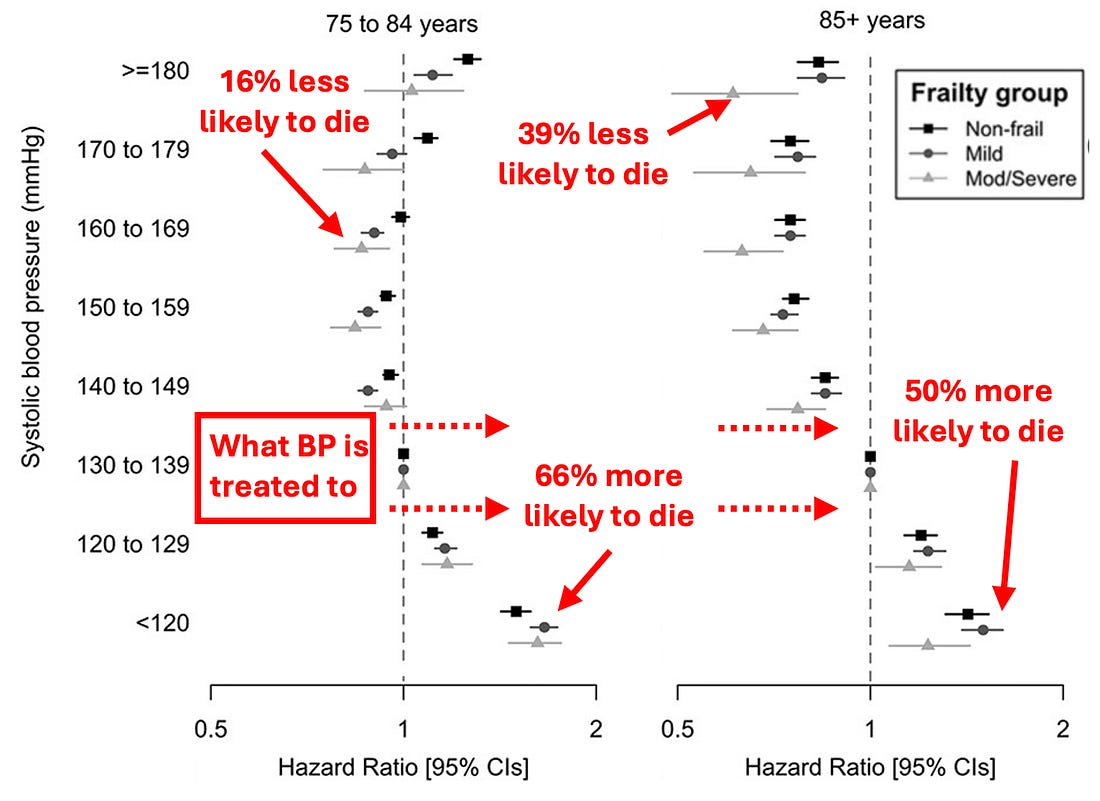
Because of this, blood pressure levels were enforced that are much more likely to harm than help the elderly (and likewise to create many debilitating side effects along the way).
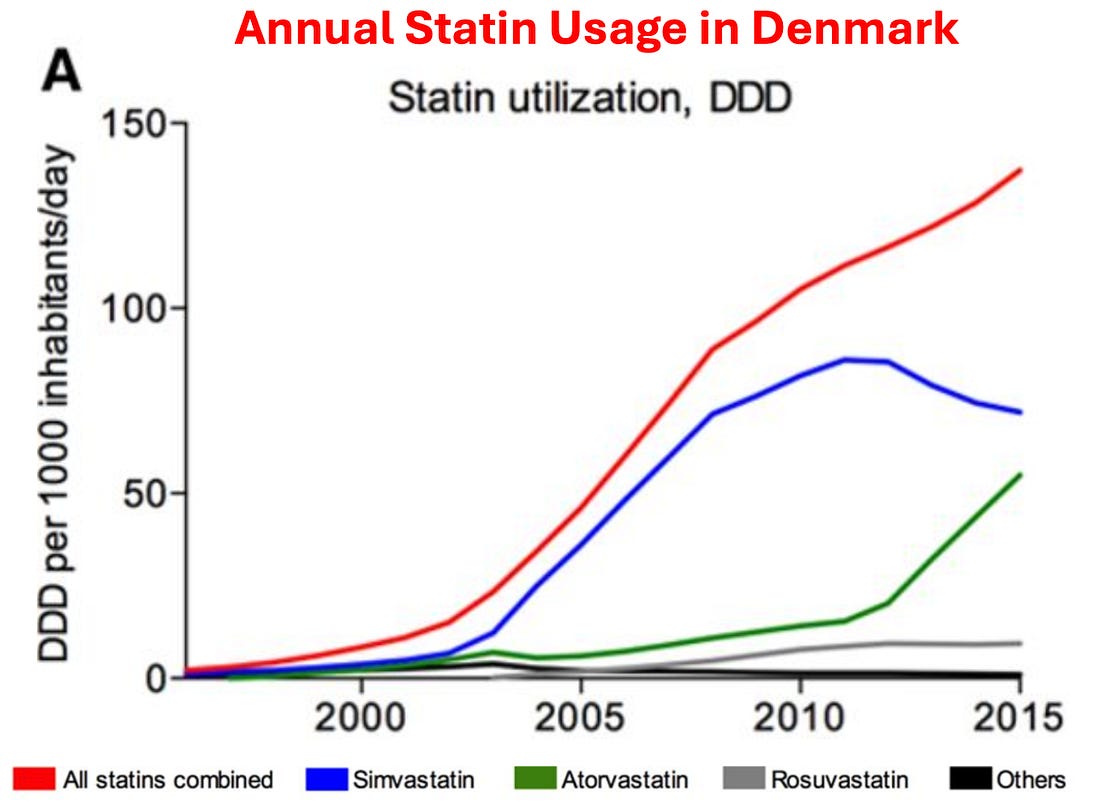
In the case of statins, prior to their discovery, it was difficult to reliably lower cholesterol, but once they hit the market, research rapidly emerged stating that cholesterol was more and more dangerous, that lower and lower blood cholesterol levels were needed, and, hence that more and more people needed to be on statins.
As you would expect, similar increases also occurred within the USA. For example, in 2008-2009, 12% of Americans over 40 reported taking a statin, whereas in 2018-2019, that had increased to 35% of Americans. Given how much these drugs are used, it then raises a simple question—how much benefit do they produce? As
it turns out, this is a remarkably difficult question to answer as the
published studies use a variety of confusing metrics to obfuscate their
data (which means that the published statin trials almost certainly
inflate the benefits of statin therapy), and more importantly, virtually
all of the data on statin therapy is kept by a private research collaboration which consistently publishes glowing reviews of statins (and attacks anyone who claims otherwise) but simultaneously refuses to release their data to outside researchers, which has led to those researchers attempting to get this missing data from the drug regulators. In circumstances like these where an unsafe and ineffective but highly lucrative drug must be sold, the next step is typically to pay everyone off to promote it. For example, to quote Chapter 7 of Doctoring Data:
Note: the primary reason no cure for COVID-19 was ever found was that the guideline panel for COVID-19 treatments was handpicked by Fauci, comprised of academics taking money from Remdesivir’s manufacturers. Not surprisingly, the panel always voted against recommending any of the non-patentable treatments for COVID-19, regardless of how much evidence there was for them. Likewise, the American College of Cardiology made a calculator to determine your risk of developing a heart attack or stroke in the next ten years based on your age, blood pressure, cholesterol level, and smoking status. In turn, I’ve lost track of how many doctors I saw proudly punch their patient's numbers into it and then inform them that they were at high risk of a stroke or heart attack and urgently needed to start a statin. Given that almost everyone ended up being “high risk” I was not surprised to learn that in 2016, Kaiser completed an extensive study which determined this calculator overestimated the rate of these events by 600%. Sadly, that has not at all deterred the use of this calculator (e.g., medical students are still tested on it for their board examinations). Note: one of the most unfair things about statins is that the healthcare system decided they are “essential” for your health, so doctors who don’t push them are financially penalized, and likewise patients who don’t take them are as well (e.g., through life insurance premiums). So, despite the overwhelming evidence against their use, many physicians believe so deeply in the “profound” benefits of statins that they do things like periodically advocating for statins to be added to the drinking water supply. In tandem, a cancel culture has been created where anyone who challenges the use of Statins is immediately labeled as a “statin denier” accused of being a mass murderer and effectively canceled. Recently, one of those dissidents, Dr. Aseem Malhotra British cardiologist who has also spoken out against the COVID vaccines went on Joe Rogan where he discussed that dirty industry and the remarkable parallels between how Statins and the COVID vaccines were pushed on the world: Note: one of the most remarkable facts Aseem shared was that the previously mentioned statin collaboration (which militantly insists less than 1% of statin users experience side effects) also created a test one could utilize to determine if one was genetically at risk for a statin injury—and in their marketing for the test said 29% of all statin users were likely to experience side effects (which they then removed once attention was brought to it). In addition to doctors being forced to follow these guidelines, patients often are too. Doctors often retaliate against patients who do not take statins (similar to how unvaccinated patients were denied essential medical care during COVID-19). Employers sometimes require cholesterol numbers to meet a certain threshold for employment (although they never did anything on the scale of the COVID-19 vaccine mandates placed on workers around America). Similarly, life insurance policies often penalize those with "unsafe" cholesterol numbers. Worse still (as the processed food industry intended by creating the war against cholesterol) even if we disagree with this dogma, its difficult to boycott it as the entire food supply has replaced healthy saturated fats (e.g., from animals or coconuts) with unhealthy vegetable oils. Fortunately, after decades of work, we’ve managed to bring enough attention to this subject (especially with RFK’s recent support for returning to saturated fats) that market pressure is at last emerging to make seed oil free foods become more widely available to consumers. Statin InjuriesMy primary issue with the statins is not the fact we waste billions each year on a useless therapy (approximately 25 billion per year in America alone). Rather, it’s the fact that they have a very high rate of injury. For example, the existing studies find between a 5-30% rate of injuries, and Dr. Malhotra, having gone through all the existing evidence estimates that 20% of statin users are injured by them. Statins in turn, are linked to a large number of complications that have been well-characterized (e.g., mechanistically) and described throughout the medical literature.1, 2, 3, 4, 5, 6
The other group are those not overtly noticed by the patient. These include:
All of this, in turn, highlights one of the major issues with our medical system—statins have a high rate of side effects, and since so many people are on them, a lot of people we routinely encounter are being affected by them. However, because of how pervasive those side effects are, we’ve become habituated to them and just see them as “normal.” For instance, Senator Ron Johnson, a reasonably informed and intelligent person (who being a Senator receives top quality medical care) experienced a sudden hearing loss that was investigated but no one could explain. Recently he shared on Tucker Carlson that after he learned sudden hearing loss (one of the side effects listed above) was a statin side effect and he’d been on one at the time of the hearing loss, he decided to discontinue it, and then noticed his inexplicable dizziness disappeared. In short, Johnson’s experience suggests many others are frequently experiencing unrecognized side effects from routinely prescribed drugs. In my own case, the moment I first encountered statin patients, I quickly noticed that they would report either numbness in their body, muscle weakness and pain, or impaired cognition, which began after they started the statin and resolved once they stopped using it. Remarkably, we also noticed that whenever they (or we) pointed this out to their doctor, the doctor would become extremely hostile, and then insist that the statin could not be causing the symptom (e.g., “because in all their years of practice, they had never had a patient who was injured by a statin”) and that even if it was harming them, the patient needed to stay on it because otherwise they would get a heart attack and die. Note: typically, it is the most easy to recognize if something is poisoning the population if you could see the baseline before and after it was introduced (e.g., since the COVID vaccine rollout, patients are much sicker than they were before). Unfortunately, since the historical baseline is never taught in medicine, doctors entering practice always assume the sickness they see around them is “normal” and it’s often not until the ends of their careers that they can see how much sicker and harder to treat patients become throughout the period. As such, while there has been a massive decline in human health over the last 150 years many have corroborated (which I believe began with the introduction of the smallpox vaccine), this decline remains largely unrecognized by the medical system and instead is simply the “new normal.” In turn, as the years went by, I saw increasingly elaborate excuses being created to protect the statins from an ever-increasing awareness of their dangers. For example, I lost count of how many doctors I knew who cited this 2016 study when patients stated they had been injured:
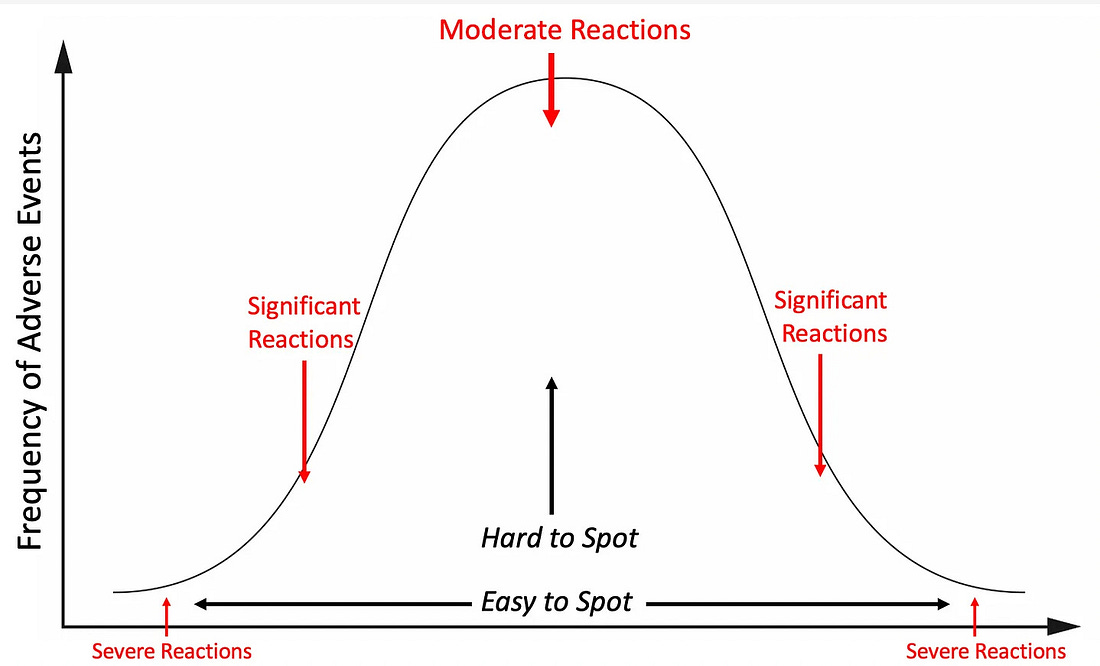
Which, when translated into plain English means that the only reason people believe statins injured them is because they were tricked into imagining the injury, so the best solution is to tell them the symptoms are in their head (a tried and true tactic of the medical industry known as “medical gaslighting”). What I found remarkable about this study was that the doctors who cited it never considered that the nocebo effect could not apply as their patients were not aware things like muscle pain were associated with statins until they experienced them (and then looked up what was happening) or that the discrepancy in the observed rate of adverse events could also be explained by the fact the randomized controlled trials are always funded by the pharmaceutical industry and hence consistently cover up injuries that occur there. Similarly, the thing that finally made me realize how impressive the marketing for these drugs had been was the recurring battle I would have with relatives. In each case, I would take them off a statin and provide a strong argument with data supporting why they should not be on the drug. At some point later, they would go to their doctor and inform them that their relative (me), who was a doctor, had taken them off the statin. Their doctor (often a cardiologist), in turn, would tell my relative I was incredibly ignorant, insist they knew the data much better than I did, say I was endangering my relative’s health, and promptly restart the statin, to which my relative dutifully complied. In many cases, I would provide the cardiologist with literature supporting my argument. In each case, they would make an excuse not to read it while simultaneously asserting that they knew all the data and that I, not being a cardiologist, was unqualified to have an opinion on this subject. This made me further appreciate just how challenging a situation patients (without access to the resources my relatives had) were in. If you take this story and replace “statin” with COVID-19 vaccines, you will see it is essentially what everyone has experienced over the last four years with the vaccines. I suspect this is because, before the COVID-19 vaccines, statins were one of the most profitable medical franchises and, thus amongst the medications most aggressively pushed on patients. Note: two adverse event reporting systems exist for adverse reactions to pharmaceuticals, MedWatch and FAERS. Like VAERS, they suffer from severe underreporting (it is estimated only 1-10% of adverse events are reported to them). The author in the next section was able to find hundreds to thousands of reports for many of the statin injuries in MedWatch that matched what he had personally observed. However, despite these reports existing, nothing has been done with them, and there is almost no knowledge within the medical community that these adverse events exist. The Statin Damage CrisisThroughout this publication, I have tried to make the point that less severe reactions to a toxin are much more common than severe ones. Because of this, if you see a cluster of severe reactions, it indicates that far more, less severe reactions are occurring as well (which is how after learning of a few people in my circle dying suddenly from the COVID vaccines, I was able to correctly predict the scale of the non-fatal injuries that would hit America).
Likewise, if you see a large number of less severe reactions to a pharmaceutical (e.g., the statin-induced muscle and nerve damage), you can predict far more severe injuries are lurking in the background. As the longer list of adverse events I shared above demonstrates, this unfortunately is true for statins. In the next two sections, I will quote one of the best books I have found on this subject:
Duane Graveline MD was started on a statin and soon after developed global amnesia (which is really scary). He decided to stop the statin and recovered.
Eventually, he was persuaded to try the statin again.
Later he discovered:
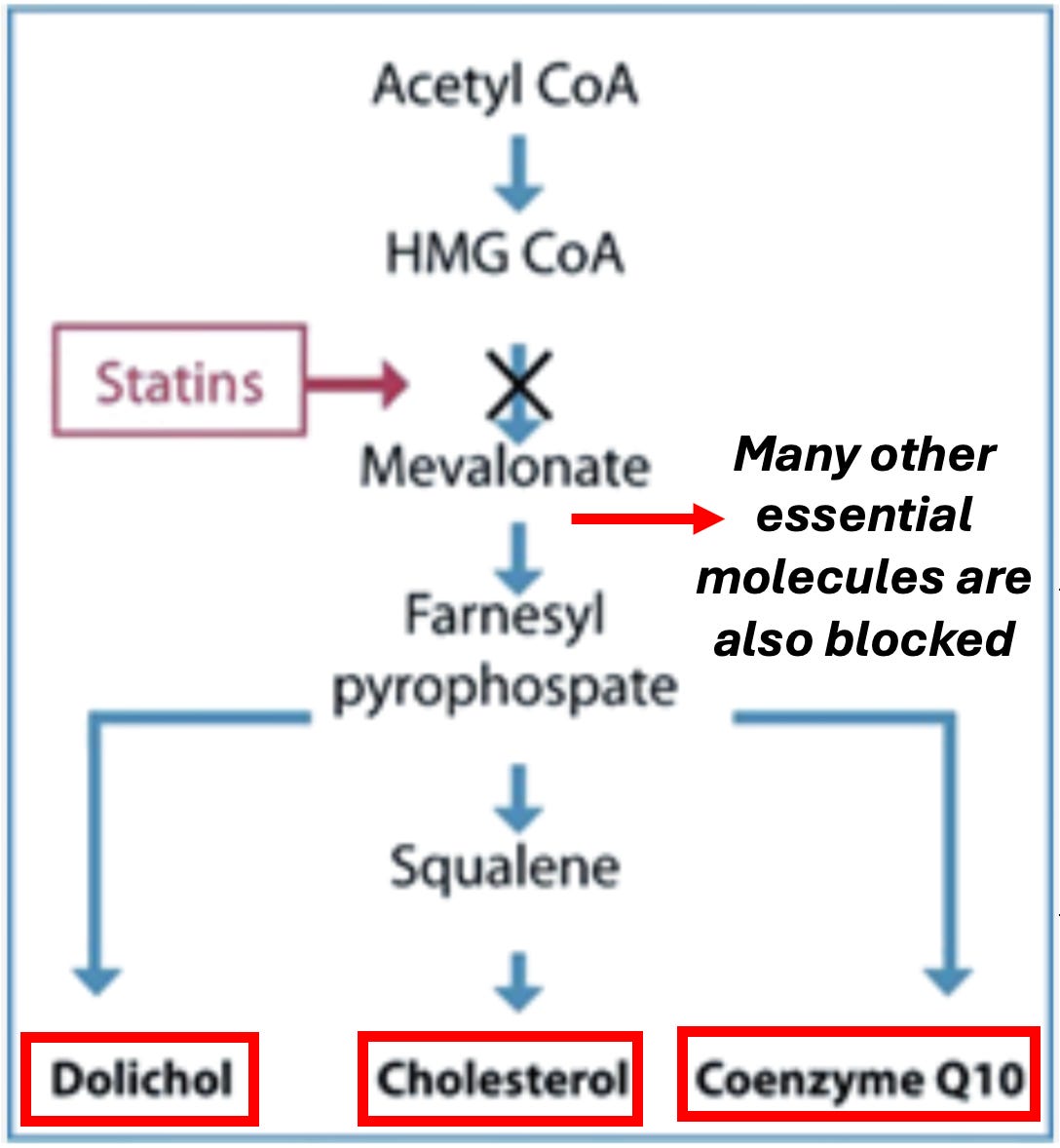
Because of this and other debilitating long-term complications (e.g., previously an extremely fit individual, he developed chronic exhaustion), Graveline became an expert on statin injuries and, in 2014, wrote The Statin Damage Crisis. Many of the points he raised there explain why statins are so dangerous, but unfortunately, are virtually unknown within the medical field. Statin Mechanisms of HarmStatins work by inhibiting an easy to target enzyme that is necessary for the production of cholesterol. Unfortunately, blocking that enzyme disrupts a variety of other vital physiologic processes. Let’s review what that enzyme does:
As these compounds are essential for the body, understanding statin toxicity hence requires us to understand what happens when each of these goes missing. CholesterolCholesterol has a few different essential functions in the body. These include: •It is the precursor to many different hormones. •The brain’s synapses (which, amongst other things, form memories) require cholesterol to function. Since cholesterol is too big to enter the brain, glial cells (support cells of the nervous system) synthesize it within the brain. Statins, unfortunately, inhibit glial cell production of cholesterol. •Cognition, in turn, is highly dependent upon cholesterol. For example, one study found that minor cognitive impairment could be detected in 100% of statin users if sufficiently sensitive testing was done (which again illustrates how minor injuries are more common than severe ones). Likewise, a variety of more severe adverse effects on cognition are also observed such as amnesia, forgetfulness, confusion, disorientation, and increased senility.
Note: one of the sadder side effects we have frequently observed from the COVID-19 vaccines has been a rapid cognitive decline in the elderly (who cannot often advocate for themselves). When this happens, like statin damage, it is always assumed to be due to “their age” and ignored. In addition to cognitive impairment, numerous studies have found a significant association between low or lowered cholesterol levels and violence. Likewise, statin dementia is often characterized by aggression. Finally, one of the most concerning side effects of statins is their tendency to cause ALS (a truly horrible rare disease—curiously also seen in association with the COVID-19 vaccines). This correlation is further supported by many reports of statin ALS improving once the statin is stopped. Unfortunately, while statin cognitive decline frequently improves when the statin is stopped, in many cases, it instead persists. CoQ10CoQ10 is an essential nutrient that both the mitochondria (which power the human body) and the stability of our cell walls depend upon. CoQ10 deficiency caused by statins is generally considered the most common cause of their side effects. This is really sad because those side effects could have been prevented if CoQ10 had been given with the statin. Unfortunately, this is unlikely ever to happen, as doing so would be equivalent to an admission statins could cause harm—in fact Merck patented statin formulations containing CoQ10 (as this would prevent major statin side effects) but ultimately chose not to bring it to market. Note: the best parallel I know to this is that the primary cause of childhood vaccine toxicity is
too many vaccines being given too close together for a child's
developing circulatory and nervous systems. Most of the harm can be
avoided if vaccines are spaced apart and given later in a child's
life—but sadly doctors who promote this approach are routinely targeted
(as it is tantamount to an admission vaccines are not 100%
safe). Fortunately, while most of the population blindly followed the
CDC’s recommended vaccine schedule, we now live in a new era where only 37% of young parents intend to. •Mitochondrial damage •Lack of Energy •Chronic Fatigue Syndrome •Congestive Heart Failure and Fluid Retention •Shortness of Breath •Gout Some of the side effects of statin CoQ10 deficiency weakening cell wall integrity include: •Hepatitis (interestingly, Graveline noted that the enzyme threshold needed to diagnose statin-induced liver damage was significantly raised after this issue began being commonly reported following statin usage). •Pancreatitis •Rhabdomyolysis (rapid breakdown of skeletal muscle tissue) •Tendon and ligament inflammation and rupture. Two of the most common consequences of statins CoQ10 depletion are myopathy (muscle pain, tiredness, weakness, and cramps) and peripheral neuropathy (numbness, tingling, or burning sensations, particularly in hands and feet). Although myopathy is the most commonly reported side effect of statin usage, much of it (e.g., myositis) goes undetected. This is because the symptoms are often not accompanied by blood work showing muscle enzyme elevations and can only be detected by biopsies (which are rarely done relative to blood work). In many cases, this condition is permanent (one expert in statin injury found it was permanent for 68% of her patients, while Graveline found it was for 25% of his). Sadly, in some cases, like statin neuropathies, the myopathies will continue to progress even if the statin is stopped. One of the sadder things about statins is how aggressively they are pushed on diabetics (under the logic that since diabetics have an increased risk of heart disease, it is critical they take a statin to prevent them from having a heart attack). To highlight the absurdity of this, statins are well known to significantly increase your risk of diabetes (multiple studies have found this), which I suspect is again due to them impairing mitochondrial function. Similarly, peripheral neuropathy is a condition diabetics are well known to be at a high risk of. In one study, it was found that the risk of neuropathy (i.e., burning pain with tingling or numbness of the extremities) was increased by 14 to 26 times (depending on the type) for long-term users of statins. Furthermore, other nerve issues, such as neurodegeneration, can be caused by statins. Combinations
of myopathy and neuropathy also occur in statin users, such as
progressive pain, weakness, and incoordination throughout the body,
alongside trouble rising from a seated position, unsteadiness, and a
tendency to fall. Muscles are also observed to develop a distinctive
weakened and mushy characteristic and gradually shrink. DolicholVery few physicians know of the dolichols, which are a necessary structural component of the cell membrane and play a pivotal role in synthesizing certain proteins (specifically they facilitate N-Glycosylation and O-mannosylation). Graveline in turn argued they were responsible for the synthesis neuropeptides throughout the body, and hence that statins blocking dolichol production would lead to many neuropsychiatric issues. While I was never able to find research supporting this contention (their role in neuropeptide synthesis), genetic dolichol deficiencies have been linked to neurological changes such as developmental delay, seizures, ataxia, and intellectual disability. Additionally, lower dolichol levels have been linked to Alzheimer’s, brain aging, and the part of the brain where Parkinson’s disease develops has a very high concentration of dolichols (hence potentially making it more susceptible to dolichol deficiences). Note: Graveline also theorized that statins would increase the production of neurodegenerative Tau proteins and decrease the production of essential selenoproteins, but I was not able to find any evidence to substantiate these arguments. Nuclear Factor-Kappa BThe
small cardiovascular benefit observed from statins may not be because
they reduce cholesterol but rather because they have anti-inflammatory
properties (inflammation causes heart disease), as they inhibit NF-kB, a
vital part of the immune system. Since this suppresses the immune system, it leads to various potential issues such as reduced protection from infectious disease. For example, many common infectious organisms target NF-kB to assist in infecting their host. However, the more significant issue is that Nf-kB inhibition appears to be linked to cancer.
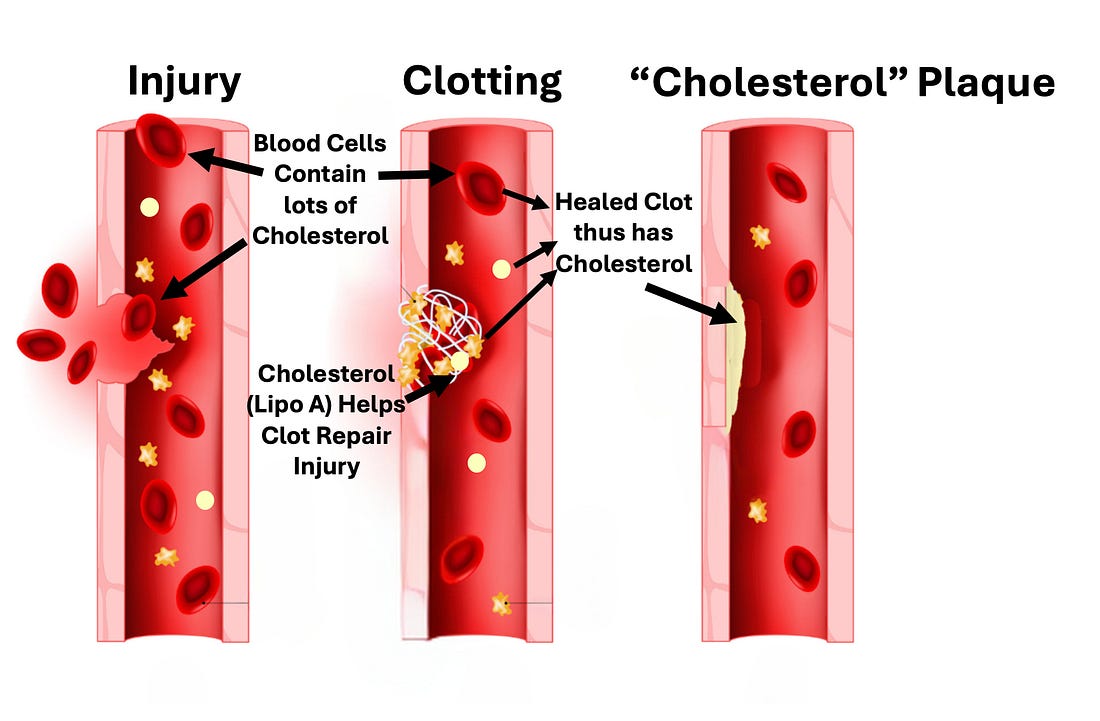
In addition to this arguing that some of the benefit of statins “preventing heart attacks” is due to them causing a fatal cancer before you have time to have a natural heart attack, this situation is somewhat analogous to what was seen with the COVID vaccines (which also cause cancer). There, the “benefit” of the COVID vaccines preventing COVID was outweighed by them causing serious conditions such as heart attacks and strokes, but if one only focused on them preventing COVID (which many did), the vaccines could be portrayed as life-saving, even though they overall did the opposite. Note: although statins appear to increase cancer, one of the few benefits I have seen a lot of evidence for is their prevention of fatal prostate cancer. My best guess is that this is due to them blocking the production of hormones in the body, and that outweighs the effects of them inhibiting NF-kB. “Cholesterol” PlaquesOne of the tricks to creating a lucrative drug market is to instill a belief throughout the population that everyone can relate to which sells your product. For example, the antidepressant industry spent years convincing the public depression was due to a “chemical imbalance” and because of how successful this campaign was, many sincerely believe it to be true even though it is a complete and utter fabrication. One of the cleverest campaigns I’ve seen within the medical industry is the widespread belief that heart disease is due to fat clogging the arteries much like they do for a drain pipe.
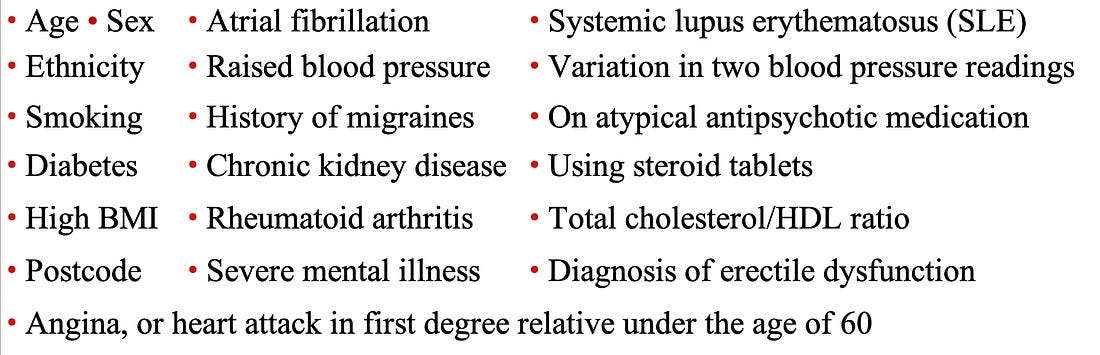
This marketing slogan in turn is remarkably persuasive as it is easy to understand (to the point that people without a medical background will feel confident repeating it to others), easy to visualize, and highly likely to elicit an immediate sense of disgust. However, given that there is no link between cholesterol and heart disease, is it necessarily true? As one of my favorite authors in this field (Malcolm Kendrick) was pondering this question, he looked at another mystery of cardiology—the fact that there is no common thread between the well-known risk factors for heart disease. For example, to calculate the risk of heart disease, England uses a calculator that combines the adjustable risks for heart disease (e.g., age) with the conditions commonly associated with causing heart disease.
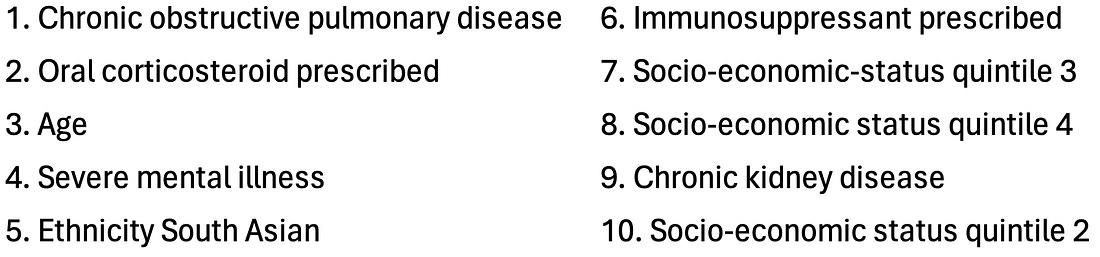
Likewise, in a 2017 study, the records of 378,256 English patients were analyzed by an AI system to determine what characteristics put them at the highest risk for a cardiovascular incident in the next 10 years. From that, they found that the ten greatest risk factors (in order) were:
From
this list, Malcolm Kendrick concluded that the common thread was that
many of these (e.g., lupus or cortisol) are associated with damage to
the blood vessels and impaired microcirculation (a consequence of
damaged blood vessels). Presently, we believe cholesterol somehow
gets into a blood vessel and then damages it, leaving an
atherosclerotic plaque. Kendrick in turn argued that a competing model
(that the medical profession largely buried) provides a much better
explanation of the actual causes of heart disease. It is as follows:
Some of the key points of evidence he uses to support this argument are: Note: another key piece of evidence for the cholesterol hypothesis is that fatty streaks on the lining of healthy blood vessels are thought to serve as the precursors to atherosclerotic plaques. However, when this was extensively researched, that progression was never observed to occur. In
short, a good case can be made that our entire heart disease model is
based on a variety of correlations that were erroneously assumed to
demonstrate causation. Sadly, while the “correlation is not causation”
mantra is frequently used to dismiss anything which challenges the
orthodoxy, you will frequently find overtly false correlations that
support the medical industry’s bottom line being treated as
unquestionable dogmas. The Causes and Treatments of Heart DiseaseKendrick’s model essentially argues the following: •Most
cardiovascular disease is a result of the blood vessel lining becoming
damaged (due to the atherosclerotic lesions) and losing the ability to
perform the normal functions (e.g., nitric oxide secretion) that allow
it to protect the circulation. Furthermore,
since his focus is not on cholesterol, that allowed him to identify
other factors which may be playing an immense (but largely
unappreciated) role in heart disease. Likewise, lead is quite damaging to the endothelium (e.g., see this study and this study), something many of us were exposed to due to it being added to gasoline, and lead rapidly entering the bloodstream once inhaled.
In turn, as lead was phased out between 1975 to 1996 (although its use
is still allowed for certain applications such as aircraft, race cars,
farm equipment, and boats—where it is occasionally used), a variety of
interesting trends exist, such as the fact heart disease exploded in
America after we started using it (and this then happening in other
European nations). Currently, it is estimated that around 400,000 deaths each year in America are due to lead exposure and in a study of 868 men,
it was observed that high levels of lead exposure (assessed by its
presence in the bones) increased their risk of dying by over 700
percent. Sadly, as you cannot sell drugs for any of these causes of heart disease, they rarely get mentioned and instead almost all of the research and discussions on heart disease are directed at cholesterol. Overall, I think Kendrick’s model is accurate, and it is my sincere hope that at some point, the medical profession will begin to seriously consider it (although given how much has been invested into the cholesterol hypothesis, it’s doubtful the industry will ever voluntarily let that market go). However at the same time, I also believe that this model is incomplete. So, in the final part of the article, I will focus on the additional factors I believe play a key role in heart disease and how they tie into our preferred treatments for heart disease (and other conditions such as COVID vaccine injuries or high blood pressure)... Continue reading this post for free in the Substack app
|


No comments:
Post a Comment