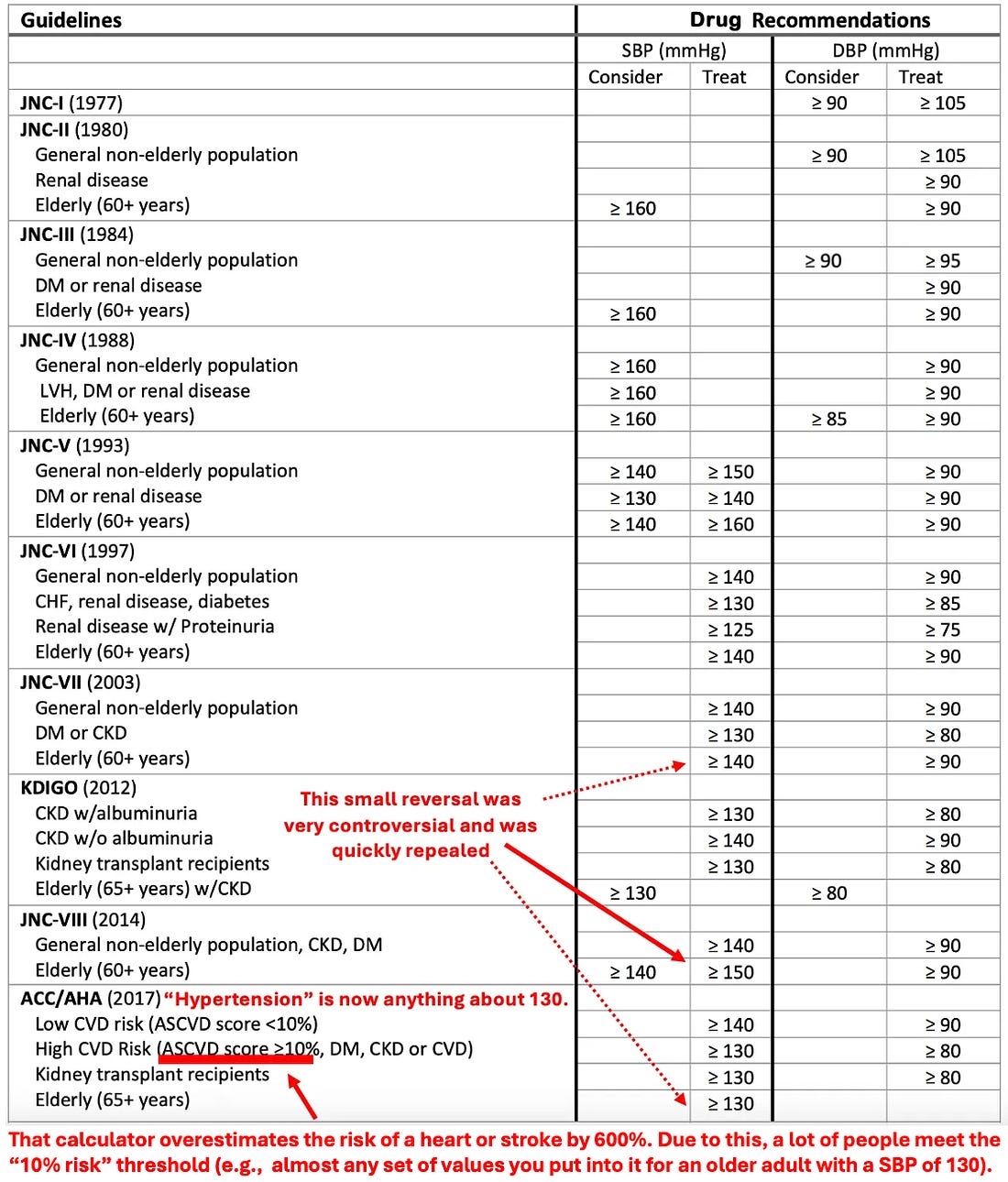
This newsletter exists to help others, and as a result, I frequently receive correspondences from individuals with pressing questions I want to answer. Unfortunately, due to how long each article takes to write (e.g., I’ve spent the last month putting together the last major part of the DMSO series and it’s still not quite done) I don’t have the time respond to all of those correspondences. I wish that I did, so the best solution I’ve been able to come up with is to have monthly open threads where anyone can ask whatever is needed (e.g., any lingering questions from the previous month) and I would make a point to always reply to them (as having them all in a single place makes it easier to get to them and also possible for others with the same question to see that answer). Each time I do a monthly thread, I try to tag it to a topic I’ve wanted to write about but I do not quite feel is enough for its own article. In this article, I will focus on one my major frustrations with the medical system—the war against salt. Note: the war against salt began in 1977 when a Senate Committee published dietary guidelines arguing for reduced sodium consumption despite the existing evidence not supporting this. Since then, like many other bad policies, it has developed an nearly unstoppable inertia of its own. Is Salt Bad For You?Many people you ask, particularly those in the medical field will tell you salt is bad, and one of the most common pieces of health advice given both inside and outside of medicine is to eat less salt. Over the years, I’ve heard two main arguments for why salt is bad for you. First, salt raises blood pressure, and high blood pressure is deadly, so salt is too and should be avoided. Second, with individuals who have heart failure, eating too many salty foods will create exacerbations of their condition, and as a result, after holidays where people eat those foods (e.g., the 4th of July) more heart failure patients will be admitted to hospitals for heart failure exacerbations. Note: excessive sodium causes these exacerbations because an excess amount of fluid accumulates in the body (e.g., because the weakened heart can’t move enough blood to the kidneys to eliminate it), which then overloads other parts of the body (e.g., causing swelling and edema, which, if in the lungs, can be life threatening). Because of these two things, many in the medical field assume that salt must be bad for you and hence strongly urge patients to avoid it (to the point you often see an elderly patient who loves her salt be aggressively pushed into abandoning it). Unfortunately, the logic behind those two arguments logic is less solid than it appears. Blood PressureMany things in medicine resulted from what approach to patient care was the most profitable, not the most helpful. In turn, since recurring revenue is a foundational principle of successful businesses, a key goal in medicine often ends up being to have as many patients as possible be on lifelong prescriptions. In most cases, the drugs that are developed and approved have real value for specific situations, but those situations are not enough to cover the exorbitant cost it requires to get a drug to market. As a result, once drugs are approved, the industry will gradually come up with reasons to give them to more and more people and in turn quickly arrive at the point where many of their customers have greater harm than benefit from the pharmaceutical. One classic way this is done is by creating a drug that treats a number, asserting that the number has to be within a certain range for someone to be healthy, and then once that is enshrined, narrow and narrow the acceptable range so less and less people are “healthy” and hence need the drug (e.g., this happened with cholesterol once statins were invested). Likewise, this characterizes the history of blood pressure management:
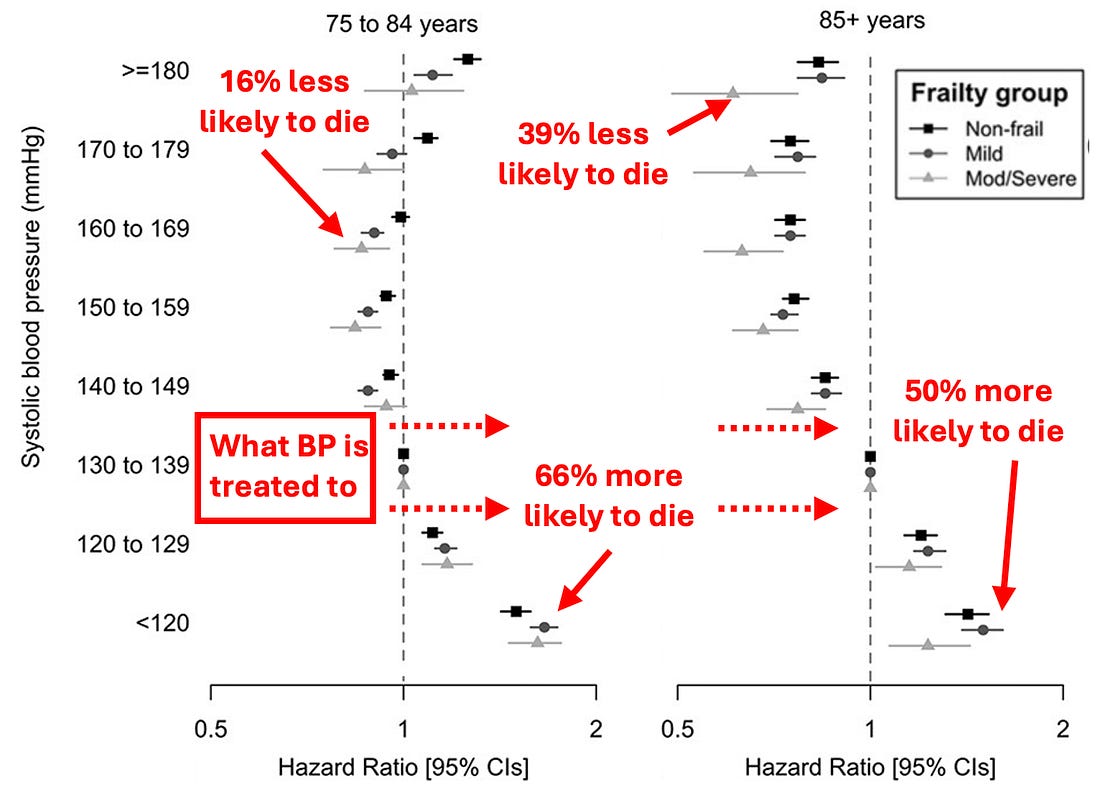
Because of this, many people (particularly the elderly) are frequently pushed to excessively low blood pressures which reduces critical blood perfusion for the organs . This then makes them significantly more likely to get a variety of significant issues (e.g., kidney injuries, cognitive impairment, macular degeneration), the most studied of which is lightheadedness or fainting leading to (often devastating) falls. Additionally, blood pressure medications also often greatly reduce one’s quality of life (e.g., by causing fatigue or erectile dysfunction). Note: for those interested in learning more about the great blood pressure scam (a lot of what we’re taught about blood pressure is less than accurate), it can be read here.
Low SodiumA corner stone of cementing the blood pressure market has been to make everyone terrified of salt (much in the same way making people terrified of the sun is a cornerstone of the lucrative skin cancer treatment market—despite the fact the deadly skin cancers are actually due to a lack of sunlight). Remarkably, much like the great dermatology scam (which has been able to make a massive amount of money from removing cancers that almost never become life threatening) the link between blood pressure and salt consumption is actual quite tenuous. For example, the most detailed review of this subject found that drastic salt reduction typically results in less than a 1% reduction in blood pressure. Likewise, doctors rarely recognize that patients in the hospital are routinely given large amounts of IV 0.9% sodium chloride, in many cases receiving ten times the daily recommended sodium chloride we are supposed to consume—yet their blood pressure often barely rises. Note: some people and certain ethnicities are salt sensitive and will experience greater increases in blood pressure consuming salt (but this does not apply to the majority of the population). Despite this, patients are often pushed to eliminate all (or almost all) salt from their life. Beyond this significantly reducing their quality of life (as people like salty foods) it can be dangerous. For example: •A study of 181 countries found countries with lower salt consumption have shorter life expentancies. •Low
sodium levels (hyponatremia) are strongly correlated with a risk of
dying (e.g., the salt consumption target we are recommended to follow increases one's risk of dying by 25%).
Likewise, a common reason for hospital admissions, are symptoms
resulting from hyponatremia (as once sodium levels get too low, it can
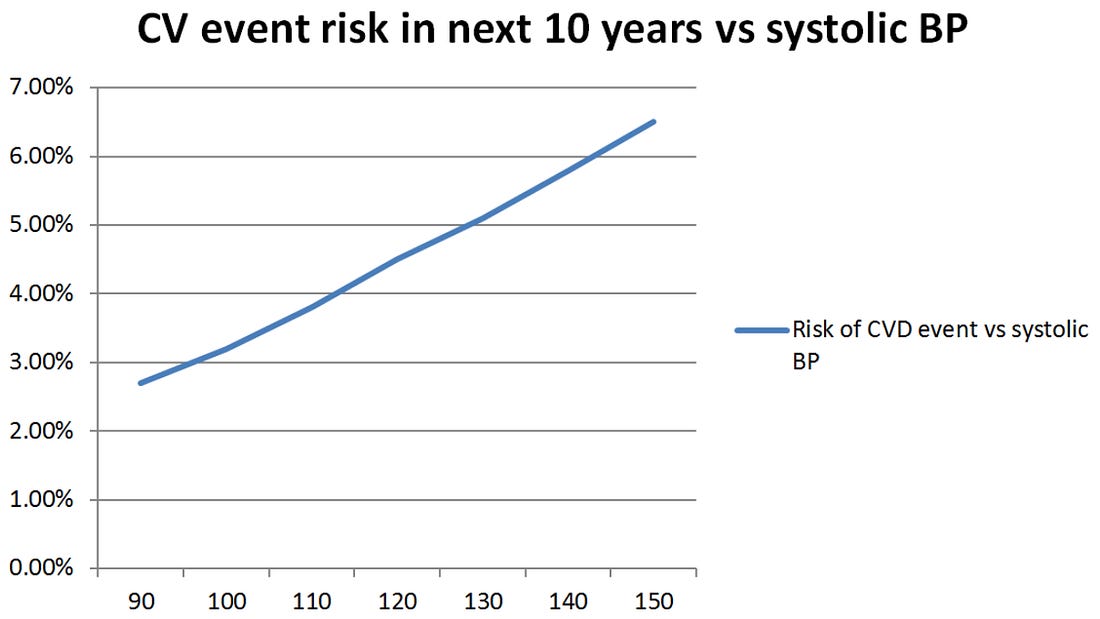
be very dangerous), and 15-20% of hospitalized patients have low sodium levels at admission. • Low dietary sodium intake causes a 34% increase in cardiovascular disease and death. •Chronic sodium depletion has been linked to fatigue and insomnia. Note: a variety of other health issues (e.g., worsening of diabetes or a stomach hydrochloric acid deficiency) have also been linked to insufficient dietary sodium. U-Shaped CurvesFrequently in physiology, a number will be observed which, when improved, appears to correlate with improved health, leading to the assumption as much as possible should be done to improve that number. In many cases however, at some point, the effect reverses, and it becomes harmful to further increase or decrease that number. For example, with blood pressure, a few data points showed that if it’s too high, it increases one’s risk of death, so this was used to create a linear model which extrapolated that trend to much lower blood pressure values.
Yet, in real life, once blood pressure gets too low, the trend reverses and one’s risk of dying increases rather than decreases.
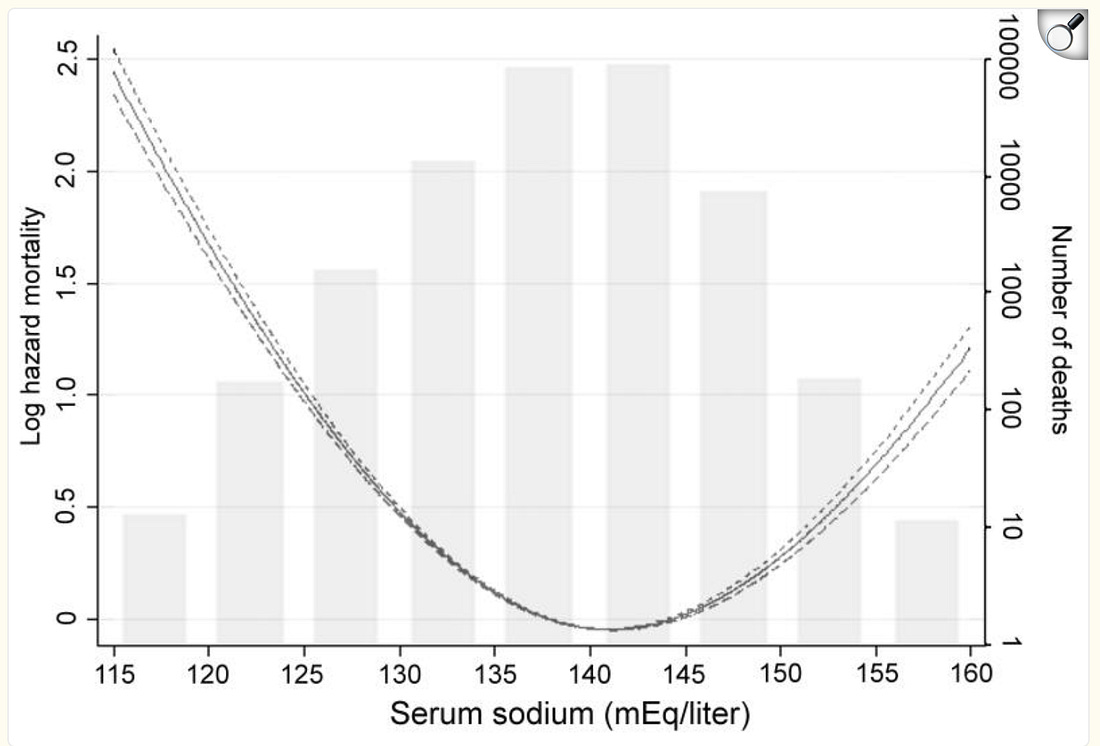
Likewise, both high and low sodium diets have been shown to increase the risk of death. This U-shaped curve was best demonstrated in a study of chronic kidney disease and heart failure patients:
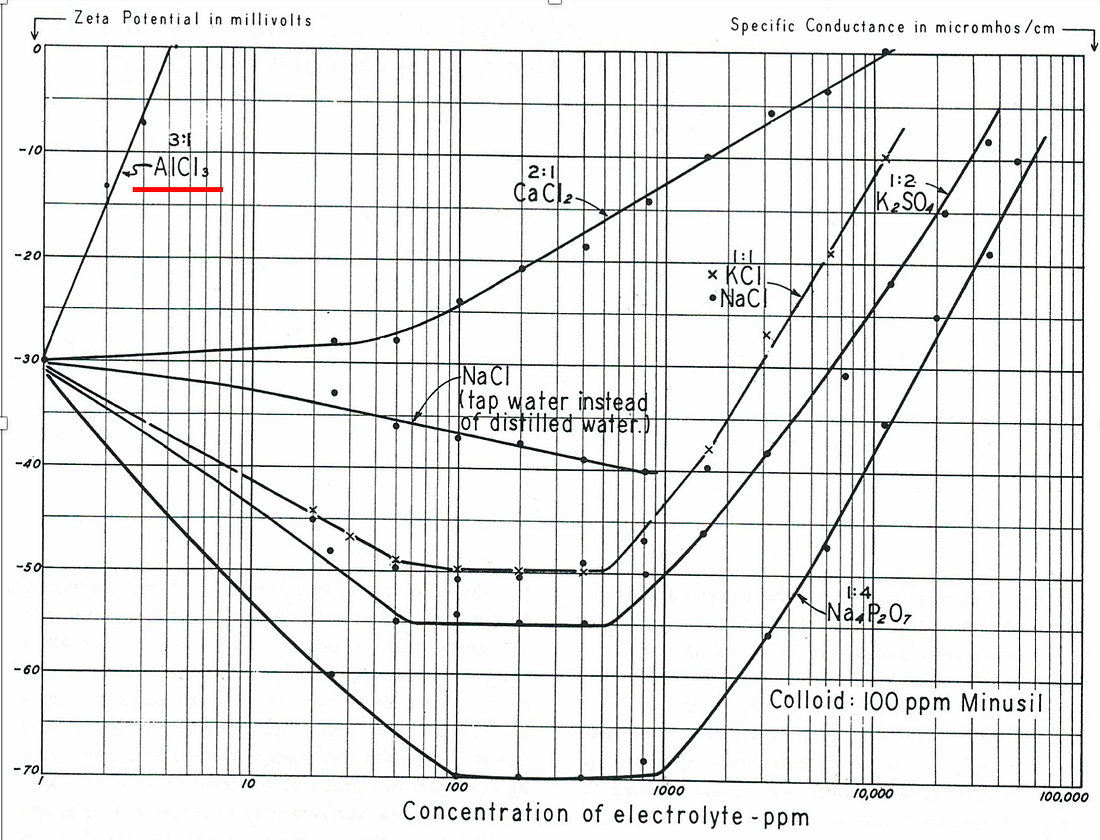
Note: due to excessive sodium consumption causing HF exacerbations, those patients are often told to avoid dietary sodium, yet there are many cases of them improving once they add some salt back into their diet (as they had been on the left side of this curve). While this has long been known within the integrative health field, in the last few years, data at last is emerging to support this,1,2,3 and Europe is beginning to rescind salt restriction recommendations for heart failure patients. Zeta Potential CurvesWhen fluid contains suspended particles (which is true for most fluids in nature), those colloids can either have finely dispersed or clumped together particles. One of the primary determinants of this is the electrical repulsion or attraction between the particles, something quantified by a system’s zeta potential and heavily influenced by the charges present in a solution (e.g, too many positive charges will make fluid components like blood cells clump together and is why the aluminum in vaccinations frequently trigger microstrokes of varying severity). In turn, many diseases result from poor zeta potential, including poor circulation and fluid congestion or edema (e.g., that seen in heart failure). One critical aspect of zeta potential is that it follows a U-shaped curve in relationship to the amount of a charged ion present, with both too little or too much of it being problematic.
Note: giving IV sodium infusions to hospital patients will frequently greatly improve their condition, something nonchalantly attributed to everyone being “dehydrated” but more accurately due to their blood sodium being too low to adequately support the physiologic zeta potential. Likewise, many people often feel much better after getting outpatient saline infusions at concierge hydration clinics. This in turn helps to explain why too little salt (e.g., through intentional sodium restriction or unintentional sodium restriction through a diet that puts you into ketosis [which increases sodium excretion]) can be problematic while at the same time high salt diets can be problematic as well. With high salt diets, I believe a few points are particularly important to recognize: 1.
I’ve had multiple cases where I ate fairly salty foods right before
bed, then woke up feeling extremely dry throughout my body with a fast
heart rate. Through trial and error I figured out drinking reverse
osmosis water would help me feel better. Later, from reading Thomas Riddick’s work on zeta potential,
I understood what was happening and measured the conductivity in my
urine, showing that my kidneys indeed were trying to dump a large amount
of sodium and restore my zeta potential. Riddick, tracked many cases
where more severe versions of what I experienced resulted in
cardiovascular incidents (as poor zeta potential causes blood to clot
together and triggers heart arrhythmias as the heart struggles to push
this congested blood). 2
Riddick (and those who followed him) found that processed foods and
many restaurant meals tended to be problematic for zeta potential and
hence advised reducing the frequency of their consumption (e.g., I try
to minimize eating out because of the congestion I feel after restaurant
meals). 3.
Riddick believed one of our key issues with salt was that potassium was
better for zeta potential than sodium, so by switching our potassium
based sources of salt (e.g., vegetables) for highly salted foods, we
were creating an unhealthy balance between the ions. Likewise, modern
research has shown adequate potassium alongside sodium is critical for cardiovascular health (e.g., normalizing blood pressure). 4.
In general, I noticed most of the salt overload issues individuals run
into come from eating foods high in refined salt (e.g., salty processed
foods) rather than those consuming natural salts. This has led me to
suspect that a major issue with salt is either something else present in
the processed foods or something specific to processed salts. At this
point, my best guesses is that is due to refined salts: Healthy SaltSince salt is such an integral part of our life, I frequently receive a variety of questions on which type of salt we should consume. In the last part of this article (which exists as an open forum for you to ask any questions you have), I will share what I’ve learned from years of exploration on this topic, which brands of salt we prefer, and the other critical steps for ensuring salt is compatible with health... Continue reading this post for free in the Substack app
|


No comments:
Post a Comment