Thank you for reading and sharing Bailiwick News by email and social media. To support Bailiwick with a paid subscription: Question from Jessica Hockett:
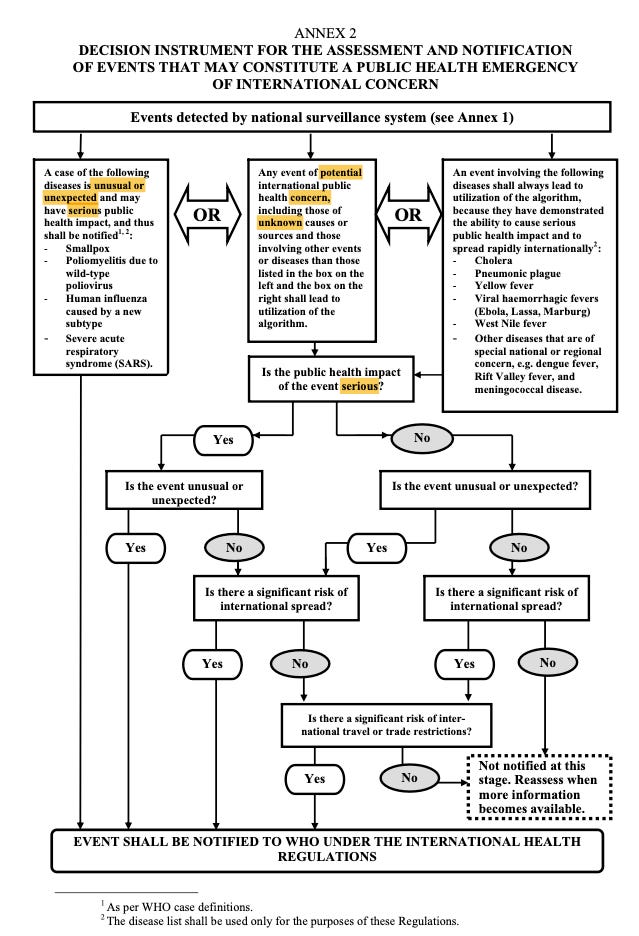
My reply: Another person to ask about this is James Roguski I have spent far less time studying the WHO International Health Regulations than Roguski has. I think the WHO-IHR is probably the legal instrument whose contents would address this question. I've focused on studying American federal and state law, because the WHO-IHR, in itself, has limited enforcement mechanisms. My understanding is that the enforcement mechanisms the WHO-IHR does have come mostly by reference to other treaties and trade agreements, that can be used to financially penalize non-compliant countries. (Other enforcement mechanisms include the terms of vaccine supply contracts that prohibit third-party testing of delivered products and designate state assets as collateral to be forfeited in the event the purchasing government violates contract terms.) WHO-IHR directs or requires participating member-states to adopt and implement their own domestic laws for pandemic surveillance, reporting and response measures, and subjects them to financial penalties if they don't adopt those implementing laws. For example, Article 56, Section 4: "Nothing in these Regulations shall impair the rights of States Parties under any international agreement to which they may be parties to resort to the dispute settlement mechanisms of other intergovernmental organizations or established under any international agreement." I looked briefly last night and this morning at the WHO-IHR, as of the 2005 amendments, with your questions in mind. In the definitions section, the WHO-IHR defines a PHEIC as "an extraordinary event which is determined as provided in these Regulations i. to constitute a public health risk to other States through the international spread of disease and ii. to potentially require a coordinated international response." There's a schematic diagram at Annex 2, called a "decision instrument for the assessment and notification of events that may constitute a public health emergency of international concern." One of the three potential pathways mentions an "algorithm" but I haven't located any other references to an algorithm in a keyword search of my files. (That doesn't mean there isn't an algorithm. I just don't have more information about it currently.) In a Federal Register notice Feb. 6, 2020 (85 FR 7874) about quarantine and airline reporting requirements, HHS-CDC used the WHO-IHR definition in a footnote: "Under the International Health Regulations, a public health emergency of international concern is 'an extraordinary event' that constitutes a 'public health risk to other States through international spread of disease and to potentially require a coordinated international response." Screenshots of the decision diagram from Annex 2 of WHO-IHR 2005 below; link to the 82-page WHO-IHR, Third Edition in which the Annex is located. The 2005 WHO-IHR language is general, circular, or self-referential: "unusual" or "unexpected," cases of disease, events "of potential concern" or events of "unknown causes or sources," with cases identified "as per WHO case definitions." I also located a July 22, 2022 WHO document about case definitions, which uses general clinical symptoms (cough, fever) or epidemiological criteria (contact with probable or confirmed cases), or positive-result from non-validated diagnostic tests. There may be other provisions in the 2022, 2023 or 2024 amendments that Roguski would be able to describe and explain their applicability to your question. My provisional understanding is that the WHO-IHR framework is the same unilateral, no-physical-evidence-required, no-validated-case-or-causality-validation-methods-required framework as the US federal framework that centers on the unfounded, unilateral assertions of the HHS Secretary. To the extent there are no firm, physical criteria or requirements for validated physical/analytical methods capable of validating the stable identity of an allegedly disease-causing pathogen and its capacity to cause disease, and no procedures in the WHO-IHR for challenging claims that a PHEIC is occurring, I don't think there are any legal bases or venues on or in which the falsity or invalidity of such claims could be brought for review and reversal. In other words, my interpretation of the PHEIC legal instruments is that, like the US federal and state laws, the WHO-IHR is also written so that no one can be found in legal violation of a rule they were never required to comply with, nor can anyone be found to have failed to meet an evidentiary standard they were never required to meet. Deception, fraud, misrepresentations, mischaracterizations, etc. are legal, because there are no legal obligations to provide evidence, and no standards of evidence against which claims can be tested, and no procedures or venues through which claims can be challenged and tested. Sometimes I think of it in terms of criminal prosecutions in a context in which framing a human suspect has been legalized. It's as if criminal prosecutors were not required to present any evidence that a crime occurred, nor any evidence that the human suspect had means, motive or opportunity to commit the crime, nor that he or she actually committed the crime. And it's as if the prosecutor were not required to go before any fact-finding tribunal (judge or jury), because evidence and evidentiary-review are both irrelevant to the prosecution and conviction process. The conviction occurs simultaneous to the allegation. In the public health emergency context, allegedly stable, allegedly-disease-causing pathogens are framed, and they are not entitled to any due process. They're convicted as of the allegation, and all the pandemic management policies and programs unfold from that point in time onward.
Related:
All content is free to all readers. All support — reading, sharing and financial — is deeply appreciated.
|

No comments:
Post a Comment