Dermatology's Disastrous War Against The SunThe forgotten side of skin health and the necessity of sunlightStory at a Glance: •This is unfortunate because sunlight is arguably the most important nutrient for the human body, as avoiding it doubles one’s rate of dying and significantly increases their risk of cancer. Likewise, sunlight has many critical but relatively unknown functions in health. •A strong case can be made that this dynamic was a result of the dermatology profession (with the help of a top PR firm) rebranding themselves to skin cancer fighters, something which allowed them to become one of the highest paying medical specialities in existence. Unfortunately, despite the billions that is put into fighting it each year, there has been no substantial change in the number of skin cancer deaths. •In this article, we will also discuss the dangers of the conventional skin cancer treatments, the most effective ways for treating and preventing skin cancer, and some of the best strategies for having a healthy and nourishing relationship with the sun. Note: many readers found an earlier version of this article to be one of the most helpful articles on this Substack. This is a revised and improved version of it. Ever since I was a little child something seemed off about the fact everyone would get hysterical about how I needed to avoid sunlight and always wear sunscreen whenever we had an outdoor activity—so to the best of my ability I just didn’t comply. As I got older, I started to notice that beyond the sun feeling really good, anytime I was in the sun, the veins under my skin that were exposed to the sun would dilate, which I took as a sign the body craved sunlight and wanted it to draw into the circulation. Later still, I learned that sunlight has many remarkable but almost unknown critical functions such as: 1. Many of the primary rhythms in the body (e.g., the circadian rhythm) are regulated by regular sunlight exposure (both on the skin and into the eyes), and we frequently find having patients go outside and expose their face to natural sunlight first thing in the morning is immensely helpful for a variety of conditions (e.g., insomnia and depression). 2.
Sunlight drives blood circulation (which is critical for health as
when, impaired microcirculation impairs many chronic degenerative
conditions). Specifically, when water is exposed to a polar surface and
an ambient energy source (particularly infrared light), it will assume a state where it behaves like a liquid crystalline gel and displaces protons, transforming from H2O to a H3O2 (H1.5O) lattice. 3. A pioneering researcher found
biological systems were exquisitely sensitive to light spectrums and
that an excess or deficiency of key wavelengths created a wide range of
issues (e.g., poor plant growth, impaired fertility, different sex
ratios of offspring, greatly increased susceptibility to infectious
diseases and cancers, significantly increased aggression and
hyperactivity etc.). Since standard glass blocks these wavelengths and
most lights do not emit them, in addition to increasing agricultural
productivity, he was able to greatly improve people’s health
(including cancer patients) by putting them on light “diets.” In this,
one of his most interesting discoveries was that the eyes are the
primary place light enters the circulation (as the eyes are completely
translucent and contain very then blood vessels), and as such, he
frequently saw dramatic improvements in chronic illnesses (e.g., chronic
arthritis) once he replaced an individuals eye glasses with full spectrum glasses. 4. One of the most effective therapeutic modalities I’ve come across is ultraviolet blood irradiation (UVBI), which works by creating a direct line of blood from a UV light source to the blood stream—something I now believe works because people are not getting enough sunlight for sufficient amounts to enter the blood stream. UVBI (discussed further here) was originally used to treat a wide range of otherwise terminal infectious illnesses (at a time when only the earliest antibiotics existed), then quickly observed to also greatly autoimmune illnesses (e.g., asthma), surgical complications and many complex neurological and circulatory conditions—much of which was due to it greatly increasing circulation and reawakening cells or organs that had shut down. Note: typically I use UVBI either for someone who just does not feel well (e.g., due to fatigue), someone who is struggling with an acute infection like a flu (as it will often rapidly eliminate them), for a chronic viral condition like EBV or shingles (as it is one of the most effective options for these types of illnesses), to prevent the complications of chemotherapy, or for a myriad of other illnesses (e.g., a variety of autoimmune disorders) when it is not feasible to get a more targeted treatment for the disorder. Once I became a medical student (at which point I was familiar with the myriad of benefits of sunlight), I was struck by how neurotic dermatologists were about avoiding sunlight—for instance, in addition to hearing every patient I saw there be lectured about the importance of avoiding sunlight, through my classmates, I learned of dermatologists in the northern latitudes (which had low enough sunlight people suffered from seasonal affective disorder) effectively require their students to wear sunscreen and clothing which covered most of their body while indoors. At this point my perspective on the issue changed to “this crusade against the sun is definitely coming from the dermatologists” and “what on earth is wrong with these people?” A few years ago I finally learned the last piece of the puzzle through Robert Yoho MD and hence was inspired to write this entire article.
The Monopolization of MedicineThroughout my life, I’ve noticed three curious patterns in the medical industry: •They will promote healthy activities people are unlikely to do (e.g., exercising or smoking cessation). As best as I can gather, much of this is rooted in the scandalous history of the American Medical Association, when in 1899, George H. Simmons, MD took possession of the floundering organization (MDs were going out of business because their treatments were barbaric and didn’t work). He, in turn, started a program to give the AMA seal of approval in return for the manufacturers disclosing their ingredients and agreeing to advertise in a lot of AMA publications (they were not however required to prove their product was safe or effective). This maneuver was successful, and in just ten years, increased their advertising revenues 5-fold, and their physician membership 9-fold. At the same time this happened,
the AMA moved to monopolize the medical industry by doing things such
as establishing a general medical education council (which essentially
said their method of practicing medicine was the only credible way to
practice medicine) which allowed them to then become the national
accrediting body for medical schools. This in turn allowed them to end
the teaching of many of the competing models of medicine such as
homeopathy, chiropractic, naturopathy, and to a lesser extent,
osteopathy—as states would often not give licenses to graduates of
schools with a poor AMA rating. After Simmons and Fishbein created this monopoly, they were quick to leverage it. This included blackmailing pharmaceutical companies to advertise with them, demanding the rights for a variety of healing treatments to be sold to the AMA, and sending the FDA or FTC after anyone who refused to sell out (which in at least in one case was proved in court since one of Fishbein’s “compatriots” thought what he was doing was wrong and testified against him). For example, when UVBI was discovered, it rapidly swept through America’s hospitals as it saved many patients who would have otherwise died and was featured throughout the media (e.g., The New York Times and Time Magazine). The AMA then offered to “validate” Knott’s device for $100,000 plus the rights to the therapy, with Knott getting a small sales cut in return. Knott refused and the AMA conducted a study designed to fail and then reported UVBI offered no benefit (despite many of the patients in the study improving) after which hospitals rapidly abandoned the “debunked” practice (whereas UVBI is still used in the hospitals of other countries like Russia due to the phenomenal results it provides for “incurable” illnesses). Similarly, around this same time, the AMA approached the inventors of many alternative cancer therapies (such as Krebiozen, Hoxey’s remedies and the Koch Catalysts) and pressured them to sign away almost all of the rights for the treatment to the AMA or be blacklisted. In each case, the inventor refused because they wanted it to remain affordable to everyday people (e.g., the AMA had initially used Hoxey’s remedy but massively inflated the cost for it). So, following their refusal, the AMA launched a blitz against the therapy, and then with the help of the FDA, buried it (which was later corroborated by court cases and a 1953 Congressional investigation). In
short, because of the power the AMA wielded, a single fraudulent
negative study could immediately erase large bodies of independent
research showing otherwise. Because of this, many remarkable medical
innovations were successfully erased from history and part of my life’s
work and many of the things I use in practice are essentially the
therapies Simmons and Fishbein largely succeeded in wiping off the
Earth. Most infamously, Big Tobacco became one of the AMA’s biggest clients, which led to countless ads like this one being published by the AMA which persisted until Fishbein was forced out (at which point he became a highly paid lobbyist for the tobacco industry):
Note: because of how nasty they were, investigators gradually discovered how unscrupulous and sociopathic both Simmons and Fishbein were. Unfortunately, while I know from first-hand experience this was the case (e.g., a friend of mine knew Fishbein’s secretary and she stated that Fishbein was a truly horrible person she regularly saw carry out despicable actions and I likewise knew people who knew the revolutionary healers Fishbein targeted), I was never able to confirm many of the abhorrent allegations against Simmons because the book they all cite as a reference did not provide its sources, while the other books which provide different but congruent allegations are poorly sourced. The Benefits of SunlightOne of the oldest “proven” (but un-patentable) therapies in medicine was having people bathe in sunlight (e.g., it was one of the few things that actually had success in treating the 1918 influenza, prior to antibiotics it was one of the most effective treatments for treating tuberculosis and it was also widely used for a variety of other diseases). In turn, since it is safe, effective, and freely available, it stands to reason that unscrupulous individuals who wanted to monopolize the practice of medicine would want to cut off the public’s access to it. Note: the success of sunbathing was the original inspiration for ultraviolet blood irradiation. 1. Sunlight is critical for mental health. This is most well appreciated with depression (e.g., seasonal affective disorder) but in reality the effects are far more broad reaching (e.g., unnatural light exposure destroys your circadian rhythm). 2. A large epidemiological study
found women with higher solar UVB exposure had only half the incidence
of breast cancer as those with lower solar exposure and that men with
higher residential solar exposure had only half the incidence of fatal
prostate cancer. •Overall
60% more likely to die, being roughly 50% more likely to die than the
moderate exposure group and roughly 130% more likely to die than the
group with high sun exposure. Skin CancerAccording to the American Academy of Dermatology:
Likewise according to the Skin Cancer Foundation:
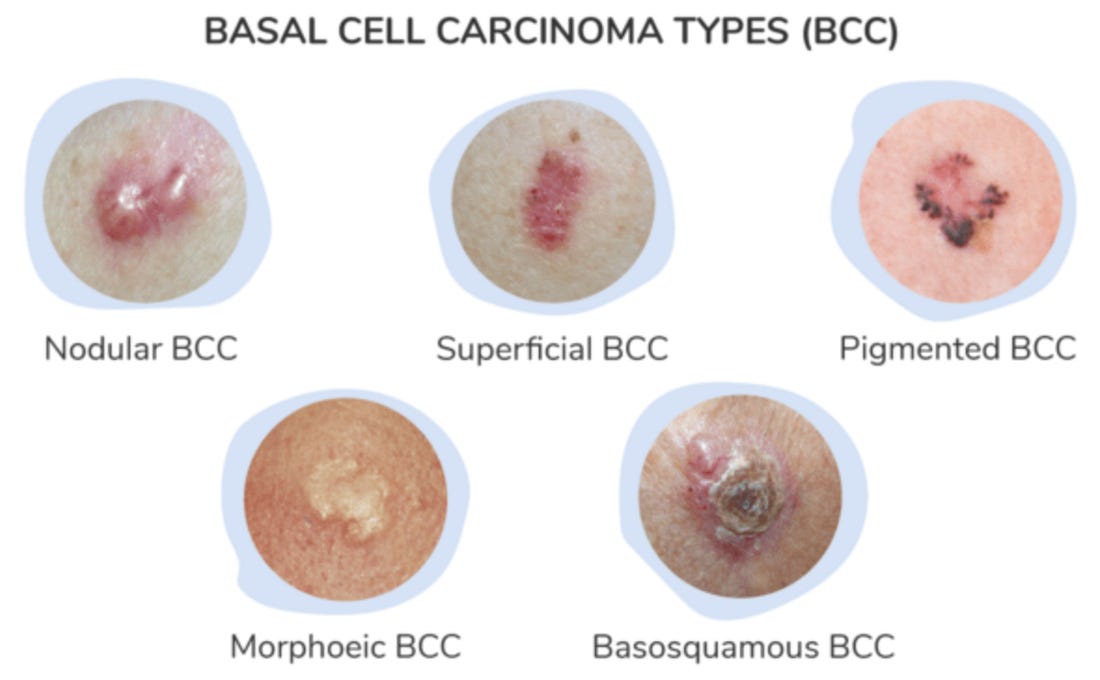
That’s sounds pretty scary. Let’s now break down exactly what that means. Note: fortunately, there is much more awareness of the vast benefits of vitamin D now (which comes from sunlight exposure). However, since many of the sun's benefits come from things besides creating vitamin D (e.g., consider the benefits of light I cited at the start of the article), the current position dermatology is beginning to pivot to (that you can substitute “unsafe” sunlight exposure with vitamin D) is not advice I can at all support. Basal Cell CarcinomaBy far the most common type of skin cancer is basal cell carcinoma (comprising 80% of all skin cancers), which for reference looks like this:
The exact incidence of BCC varies greatly, ranging from 14 to 10,000 cases per million persons, and within the United States, it is generally believed that around 2.64 million people get one per year (with around 4.32 million total cancers occurring since some people get more than one). The three primary risk factors for BCC are excessive sun exposure, fair skin (which makes you more susceptible to excessive sunlight penetrating your skin), and a family history of skin cancer. Because of this, the widely varying incidence of BCC is largely due to how much sunlight exposure people have, and typically you find it in areas with frequent sunlight exposure (e.g., the face). The important thing to understand about BCC is that because it almost never metastasizes, it is not very dangerous. Most sources say it has a 0% fatality rate. Instead, it’s normally evaluated by how likely it is to recur once it's removed (which ranges from 65% to 95%, depending on the source). Note: we feel one of the biggest shortcomings in the excision based approach to skin cancer is that it does not address the underlying causes of cancer, it can frequently lead to skin cancers recurring and more and more skin needing to be cut off (which becomes problematic as more of it is removed). This in turn is particularly problematic when a potentially deadly one recurs. However, while BCC’s never kill you, in some cases, if left alone for years, they can slowly grow to be quite large, at which point, removing them can become disfiguring (this is a common issue dermatologists in poorer areas run into). In turn, when it is clear you have a BCC, you do want to do something about it, however its not at all urgent. Fortunately, there are instances (discussed below) of the alternative therapies for BCCs still working when the tumor had grow quite large and was no longer possible to remove surgically without it being disfiguring. Note: while BCC’s are almost universally benign, I have now heard of two cases in vaccinated patients where they metastasized. Squamous Cell CarcinomaThe second most common type of skin cancer, cutaneous Squamous Cell Carcinoma (SCC) looks as follows:
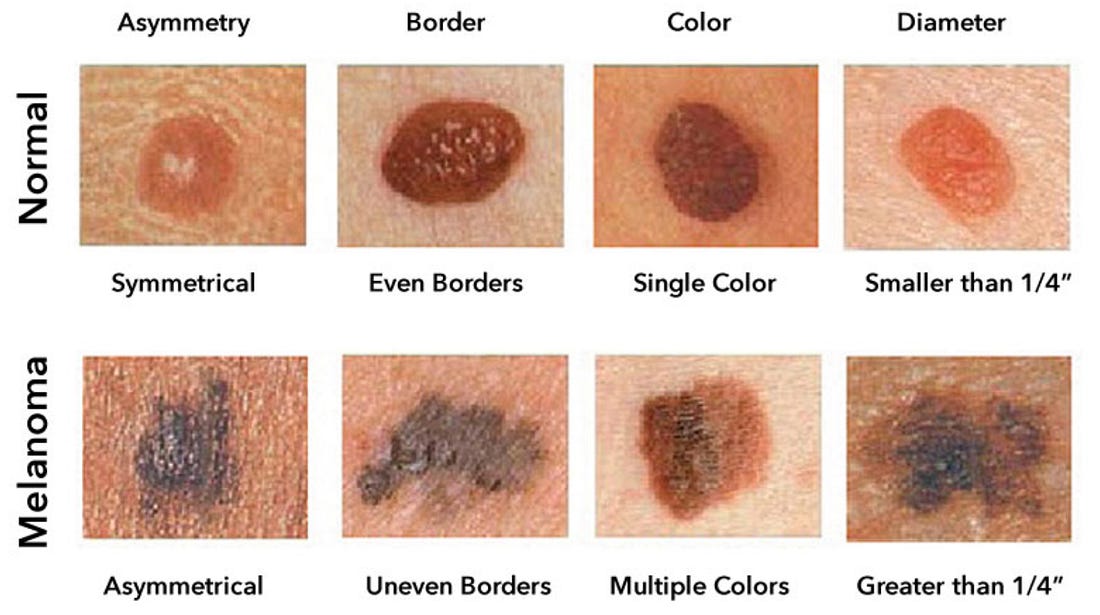
Since it is also caused by sunlight, its incidence varies greatly, ranging from 260 to 4970 per million person-years, with an estimated 1.8 million cases occurring each year in the United States. Previously, BCC was thought to occur around 4 times as often as SCC, but now that gap has closed to it only being twice as common. Unlike BCC, SCC can be dangerous, as it does metastasize. In turn, if it is removed prior to metastasizing, it has a 99% survival rate, but if removed after metastasis, this drops to 56%. As SCC is typically caught before this happens (in 1-2 years, 3-9% of them will metastasize), the average survival rate for this cancer is around 95%, and around 2000 people (although some estimates go as high as 8000) are thought to die from SCC each year in the United States. Note: since BCC and SCC are unlikely to kill people, unlike the other skin cancers, doctors are not required to report them, and there is hence no centralized database tabulating how many of them occur. As a result, the BCC and SCC numbers are largely estimates. MelanomaMelanoma is estimated to occur at a rate of 218 cases per million persons in the United States each year (with the risk varying by ethnicity). However, despite only comprising 1% of all skin cancer diagnoses, Melanoma is responsible for most of the deaths from skin cancer. Since survival is greatly improved by early detection, many guides online exist to help one recognize the common signs of a potential melanoma:
The five year survival rate for melanoma depends upon how far it has spread at the time of its diagnosis (ranging from 99% to 35% and averaging out to 94%),
which again makes it important to correctly identify—but likewise, some
cases are aggressive and metastasize quickly (so they often don’t get
caught in time) and those variants have between a 15-22.5% survival
rate. In total, this works out to a bit over 8000 deaths each year in the United States. What’s critically important to understand about melanoma is that while it’s widely considered to be linked to sunlight exposure—it’s not. For example: •A study of 528 patients with melanoma found those who had solar elastosis (a common change in the skin that follows excessive sun exposure) were 60% less likely to die from melanoma. •87% of all SCC cases occur in regions of the body that have significant sunlight exposure, such as the face (which in total comprises 6.2% of its surface area), while 82.5% of BCC occur in those regions. Conversely, only 22% of melanomas occur in these regions. This indicates that SCC and BCC are linked to sun exposure, but melanoma is not, and this is congruent with the fact that we constantly find them in areas that get almost no sunlight exposure
•Outdoor workers get 3–10 times the annual UV dose
that indoor workers get, yet they have lower incidences of cutaneous
malignant melanoma and an odds ratio (risk) that is half that of their
indoor colleagues. •Existing research
has found using sunscreen either has no effect on the rates of
malignant melanoma or increases it, which makes it quite frustrating
that governments around the world always parrot the advice to wear more
of it, especially whenever melanoma rates are rising (in other words,
exactly what we also see with the COVID-19 vaccine drives). •A (now forgotten) 1982 study
of 274 women found that fluorescent light exposure at work caused a 2.1
times increase in their risk of developing malignant melanoma, with
this risk increasing with more fluorescent light exposure, either due to
the exposure at their job (1.8X with moderate exposure jobs, 2.6X with
high exposure jobs) or the time spent working at it (i.e., 2.4X more
likely for 1-9 year of work, 2.8X for 10-19 years, and 4.1X for over 20
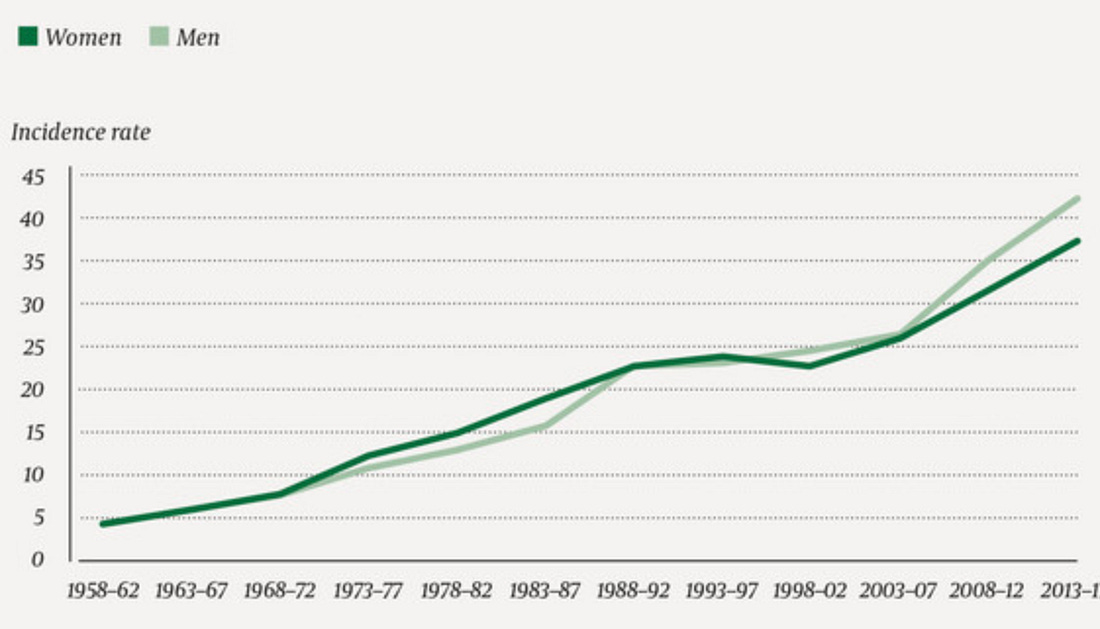
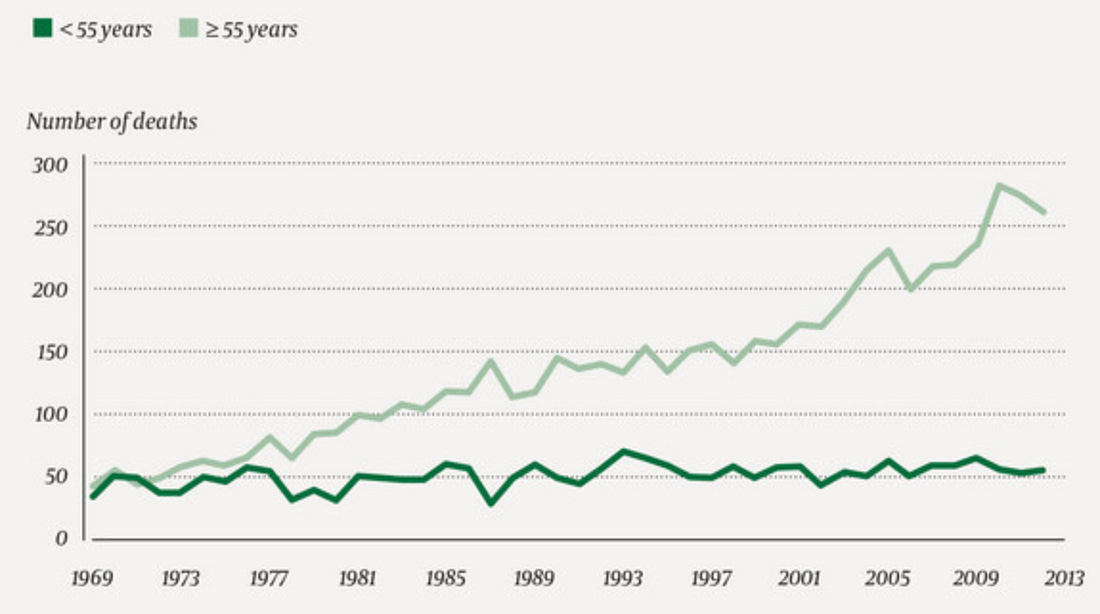
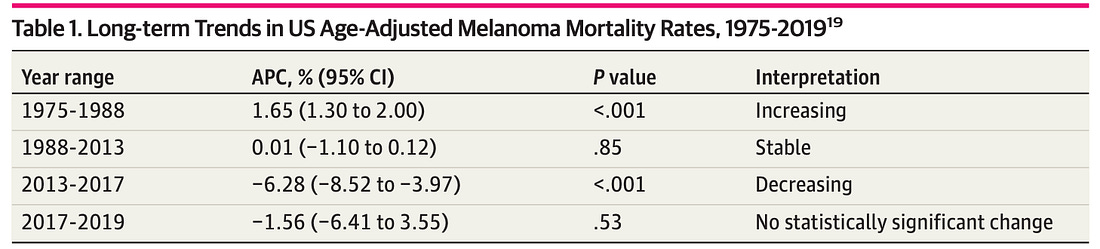
years). •There has been a significant increase in many areas from melanoma, something which argues against sunlight being the primary issue as it has not significantly changed in the last few decades. For instance, consider this data from Norway’s cancer registry on malignant melanoma:
Note: there is also some evidence linking sunlight exposure to an increased risk of developing melanoma is more conflicting, as some data points show a small reduction, while others show a small increase (e.g., this study found sunlight exposure caused the risk of melanoma to increase by approximately 20%). However, while a small increase in melanoma is seen, the opposite occurs with respect to melanomas being larger in size (e.g., one study found those on the trunk were over twice as large as those on the arms) or how likely they are to kill someone (which is what actually matters). Rare Skin CancersThis section as not important to read, I’m primarily including it as a reference to support the primary point and to be complete. Merkel cell carcinoma—7 cases per million person-years in the USA, 52-78% survival rate. Possibly link to sunlight. Kaposi Sarcoma—3 to 6 per million people in the USA, 41-81% survival rate, primarily due to immune suppression (e.g., AIDS, organ transplantation, possibly COVID vaccines). A possible but small link to sunlight. Cutaneous T-cell lymphoma— 6.4 to 8.55 per million people in the USA, 39.4-67.4%, primarily due to immune suppression and specific infections (there are also numerous noteworthy cases of it happening after COVID vaccination—including one of the participants in Moderna’s clinical trial). Dermatofibrosarcoma Protuberans—0.8 to 4.5 cases per million persons per year, 99.1% survival, risk factors not known. Acral lentiginous melanoma—1.8 cases per million person-years, 67.5%-80.3% survival rate, risk factors unknown but generally agreed not to be linked to sunlight exposure. Sebaceous carcinoma—2.43 cases per million person-years, 50-78% survival rate, linked to immune suppressing drugs, radiation therapy and an existing genetic defect. Extramammary Paget disease—0.4-0.7 cases per million people,81.6%-91.8% survival rate, not linked to sunlight exposure. The Great Dermatology ScamIn short: As such, there’s no way to justify “banning sunlight” to “prevent skin cancer,” as the “benefit” from this prescription is vastly outweighed by its harm. However, a very clever linguistic trick bypasses this contradiction—a single label, “skin cancer,” is used for everything, which then selectively adopts the lethality of melanoma, the frequency of BCC, and the sensitivity to sunlight that BCC and SCC have. This has always really infuriated me, so I’ve given a lot of thought to why they do this. Note: Dr Malcom Kendrick helps provide some perspective on how this game is played throughout the medical industry by sharing a story from Michael Baum MD:
The Most Desired SpecialtyMuch of the medical education process is providing medical students with carrots (incentivizing rewards) they can obtain if they work incredibly hard, are highly compliant, and demonstrate an above-average degree of aptitude. This in turn motivates premeds to work very hard in college (e.g., giving up their social life), and then for medical students to keep on working very hard (even though they “made it” and already got into medical school) and then often for medical residents to keep on doing that (so they can get into a prestigious fellowship). One of the key incentives here is to be able to get into a prestigious specialty, as those typically command more respect and pay more. Dermatology is commonly seen as the most desired specialty as it: It’s
hence remarkable the dermatology profession was able to pull this
economic niche off, and as a result, their field tends to attract the
most competitive students who really want the incredible lifestyle and
salary a private dermatology practice can offer (even though during the
application process everyone typically claims they want to be an
academic research since that’s what gets you in). Likewise, one of the
smartest doctors I know (who had a good heart and the capacity to
improve medicine) ultimately went into dermatology for those reasons,
and as a result an incredible amount of potential was wasted and
similarly I believe a major reason why innovative research has been so
slow in dermatology is that its compensation model attracts the gifted
physicians who are not interested in research. The Transformation of DermatologyNot too long ago, dermatology was one of the least desired professions as much of what they did was essentially just dealing with acne and pimples in the era before accutane (which unlike most pharmaceuticals actually works—but unfortunately is incredibly toxic, and has permanently disabled a few people I knew quite well). A relatively unknown blog by Dermatologist David J. Elpern, M.D. (that Robert Yoho unearthed) at last explained what happened:
A 2021 journal article provides additional context to Dr. Elpern’s remarks:
Note: this article also shares that the American government has long been extremely doubtful of the value of these screenings and the dermatology field has faced continual challenges to surmount this obstacle they’ve had to lobby for solutions to. In
short, as has happened many times in America, a remarkably
sophisticated public relations campaign was launched to transform
society for the benefit of an industry. I am relatively certain a few of the core components of this campaign were: •Allow
them to piggyback onto the fear the medical industry has marketed
around cancer to justify charging a lot of money to do something
questionable to prevent cancer and having every patient go along with it
the second they hear the dreaded “c” word. Specifically, their ultimate play was to be able to justify charging a lot of money to surgically remove skin cancers, often being paid more to do this than a surgeon receives from a standard procedure (which to some extent is justified because the surgery also requires a pathologic examination midway through). The procedure for reference is:  The
essential purpose of a Mohs surgery is to be able to have a much
smaller incision (e.g., not cutting away any more than you have to),
which can often make a big deal for a patient since large holes in the
face can be devastating. This in part is accomplished by pausing the
surgery midway through and looking at what was cut out under a
microscope so it can be determined if all of the cancer was extracted
and nothing more needs to be cut away (whereas in conventional surgery a
larger margin is used to be on the safe side). Note: the going rate for a Mohs surgery varies widely, but it is typically at least a few thousand dollars. Unlike other surgeries, most of that money goes to the dermatologist since a hospital that provides an OR, OR supplies, OR staff, and a recovery service doesn’t take a significant amount of the reimbursement. You thus might be able to guess what happened:
Note: Dr. Stern shared with Elisabeth Rosenthal that he was on a 2012 panel convened by the professional dermatology societies to evaluate when it was actually appropriate to use a Mohs surgery (due to Medicare’s concerns over it being overused). Due to the procedural structure of the meeting, the panel ultimately voted to approve 83% of the possible indications for a Mohs surgery, leading to in (Stern’s words) “A lot of us were surprised to see that many things that were quite controversial going in now looked positive and unanimous. How did that happen? It made us really uncomfortable…This was not a medical issue; it was a trade issue.” To show what that change in the guidelines translated to:
Note: this was for 2013 and it has likely risen since then (I couldn’t find a more recent study other than an article noting that in 2015, 5.9 million skin biopsies were performed on Medicare Part B recipients—a 55% increase from a decade earlier). Additionally, keep in mind that Medicare typically accounts for around 40% of dermatologists’ total patient volume and about 30% of their total practice revenue (although I’ve seen revenue estimates range from 30-60%), so this is just a fraction of what they actually make. As
you might guess, before long, this opportunity also attracted the
attention of more unscrupulous parties seeking to cash in on the
bonanza. This in turn led the New York Times to investigate the industry where they discovered: •There has been a big push (e.g., by greedy doctors) to expand this franchise into nursing homes. For example, they covered a mobile practice in Michigan that sends clinicians to 72 nursing homes where they performed thousands of cryosurgeries, along with many steroid injections and minor surgeries. The investigation in turn found that 75% of those patients had Alzheimer’s disease and most of their skin lesions were inconsequential. Furthermore, they cited a healthcare analytics firm that looked at 17,820 done on patients over age 65 in the last year of life, and found that skin biopsies and the freezing of precancerous lesions were performed frequently, often weeks before death. •This was quite unfortunate as:
Note: while cosmetically, dermatologic surgeries typically turn out quite well when performed by a competent dermatologist in a patient who isn’t too far into old age, we often find that the scars from dermatologic surgeries can cause chronic issues (e.g., pain) that requires either prolotherapy or neural therapy to correct. Typically, this is the most common for facial surgeries, which could either be due to the inherent sensitivity of that high nerve region, or due to the skin not liking being stretched and then sutured (which is what Mohs typically requires). After I published this article, numerous readers shared that they developed lifelong complications from a skin surgery (e.g., a Mohs) which didn’t heal well, and likewise a plastic surgeon reached out to say he frequently deals with these cases (something a few other plastic surgeons have also shared with me). Because of all of this, a massive funnel hence exists where patients are first terrorized of the sun and then put into a massive sales funnel to sell these lucrative surgeries. Fortunately, many are now waking up to this. For example, after being pushed through this process at a dermatology clinic, Comedian Jimmy Dore was sent this article and highlighted how he saw the entire thing was a giant scam. As I conclude this section, I will share that one of the things that always bothered me about some of the dermatology practices I shadowed was how “salesy” they felt, as the same scripts would be repeated again and again to move patients through the skin cancer sales funnel and simultaneously, the dermatologists would be very particular about having everything and everyone look as nice as possible (alongside having numerous advertisements meant to cater to their female patient’s physical insecurities). However, I must emphasize that some skin cancers (e.g., many melanomas) require immediate removal. My point here is to encourage you not to avoid dermatologists entirely but to consider seeking a second opinion from another dermatologist if you are unsure about what has been suggested to you as there are many excellent and ethical dermatologists practicing in the field as well. Changes in Skin CancerGiven how much money is being spent to end skin cancer, one would expect some results. Unfortunately, like many other aspects of the cancer industry that’s not what’s happened. Instead, again and again, we see a tendency for more (previously benign) cancers to be diagnosed, but for the most part, no significant change occurring in the death rate.
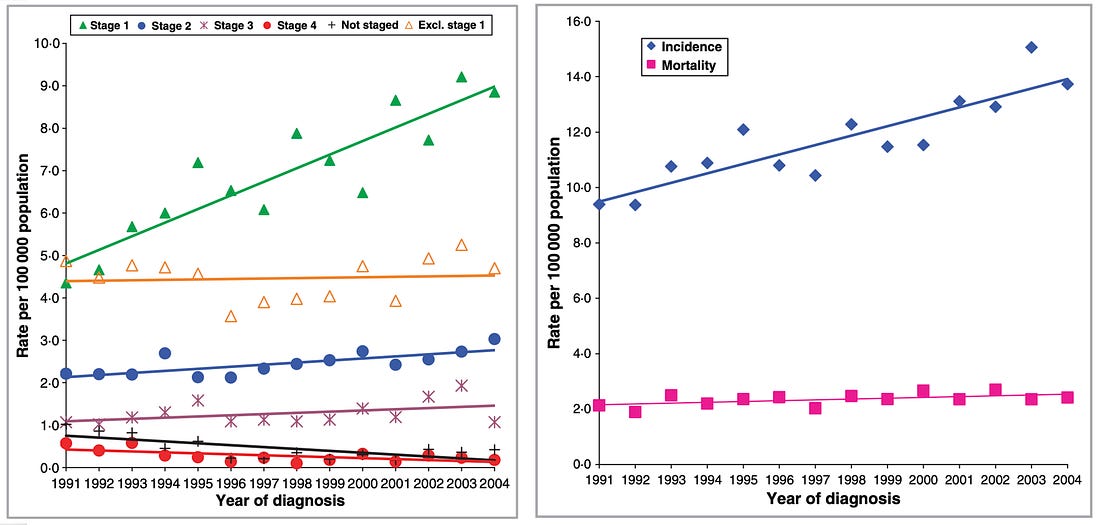
The best proof for this came from this study which looked at what type of malignant melanoma was actually being biopsied, and found that almost all of the increase in “skin cancer” were the stage 1 melanomas which rarely created problems:
This study, in turn, illustrates exactly what the result of our war on skin cancer has accomplished:
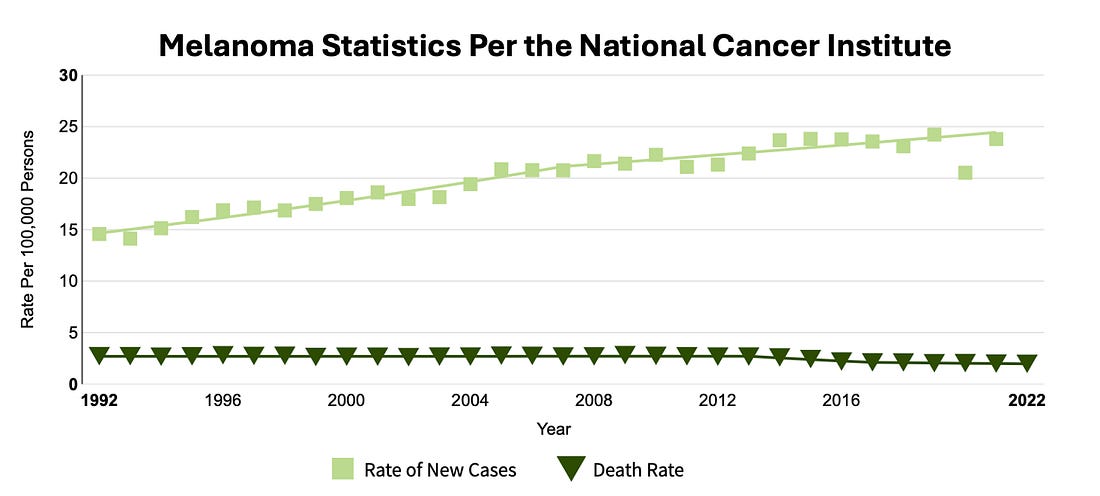
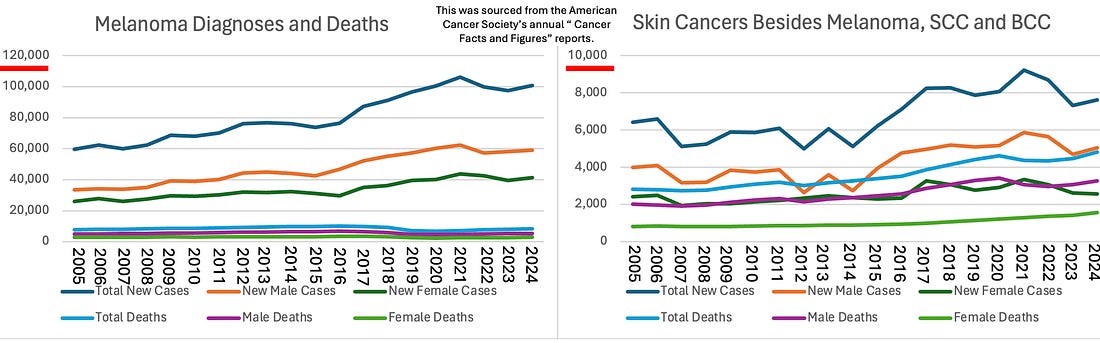
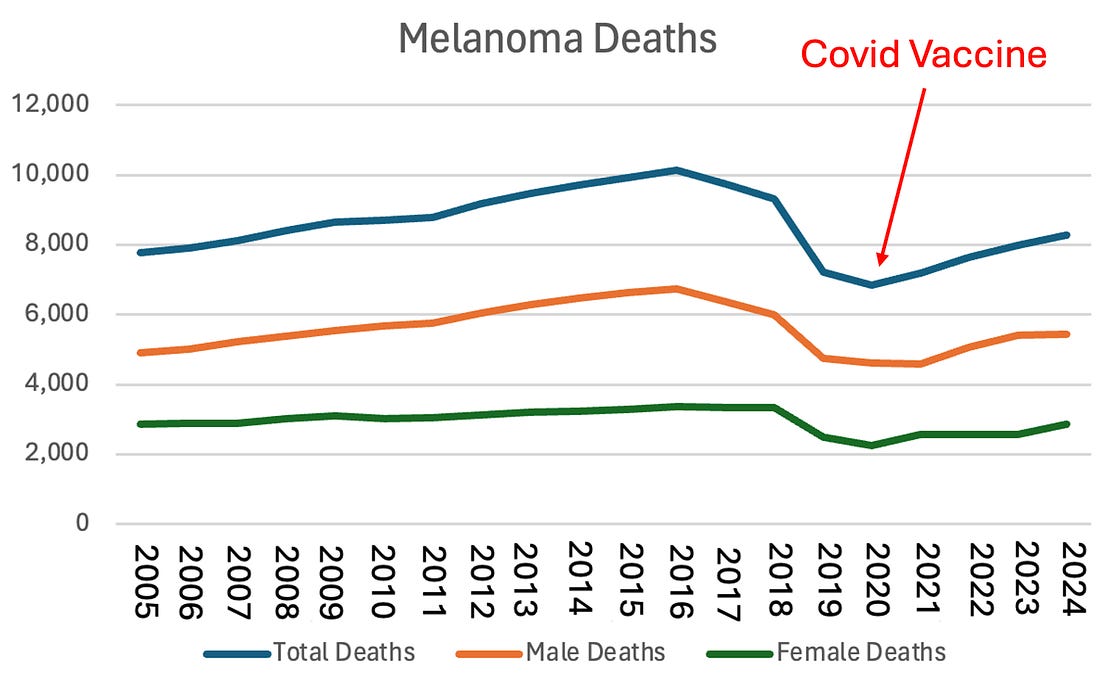
Finally, since many suspected the COVID vaccines might lead to an increase in melanoma (or other skin cancers), and I could not find the statistics for that online, I decided to create them by compiling all the available annual reports from the American Cancer Society into a few graphs:
Managing Skin Cancer and SunlightThe primary purpose of this piece was to empower each of you and get past the fear patients have of cancer dermatology has used to push this lucrative business model along. Nonetheless, I recognize that this article also raises a few obvious questions such as: In the final part of the article I will share our current thoughts on each of those questions... Continue reading this post for free in the Substack app
|



No comments:
Post a Comment