|
“Turbo cancer” is now a popular term. In four articles since May 2022, I documented evidence that the incidence rate of certain cancer-involved deaths, especially lymphoma, began increasing months after covid vaccines were released. Links to the articles are in footnotes 1 - 4.¹²³⁴
Article Thesis
There appear to be two different aspects of “turbo” cancer. 1) Greater incidence rates of cancers are theorized to be caused by immune mechanism impairment. 2) Faster growth rates are theorized to be caused by the promotion of angiogenesis.
In this article, questions are posed; data or case evidence follows.
Is there evidence of excess malignant neoplasms since Covid vaccines were introduced?
 |
Figure 1
Figure 1 depicts the numbers of death records involving the ICD-10 Code prefix
“C77,” which means, “Secondary and unspecified malignant neoplasm of lymph nodes.” Calendar year totals are represented in the left graphs and fiscal year totals are on the right. The top two graphs represent Minnesota. The middle two represent Massachusetts. The lower two represent Connecticut.Yes. Clearly, greater instances of lymph node cancer involved deaths are occurring since the covid era began. One can argue that, in Massachusetts and Connecticut, excess lymph node cancer involved deaths began before the covid vaccines were introduced. However, the excess C77 involved deaths may be the result of a massive wave of all-cause excess deaths that occurred in the spring of 2020 in those two states. The elderly have many co-morbidities listed on their death records. Some people may have died from a different cause such as pneumonia, but died with cancers, thus artificially increasing the C77 total in 2020.
SIDE NOTE
Notice the 2023 numbers in each state. Massachusetts is 2X the population of Connecticut, but 4X the purported incidence rate of deaths involving C77 lymph node cancer. Minnesota is nearly 20% smaller than Massachusetts. Yet, Minnesota lymph node cancer involved deaths are greater than 2X those of Massachusetts. The population-adjusted C77 lymph node cancer involved death rate in Minnesota is ~6.9 times the rate of Connecticut.
The point of this SIDE NOTE is to show that each state’s personnel exhibit different behaviors in how death records are effectively completed. The actual incidence rate in-fact may be very different from the recorded incidence rate, likely due to the disparate custom and practice of medical examiners state by state. This will be highlighted in the coming months in subsequent articles and the world will know that data integrity is not what scientists and readers think it is.
END SIDE NOTE
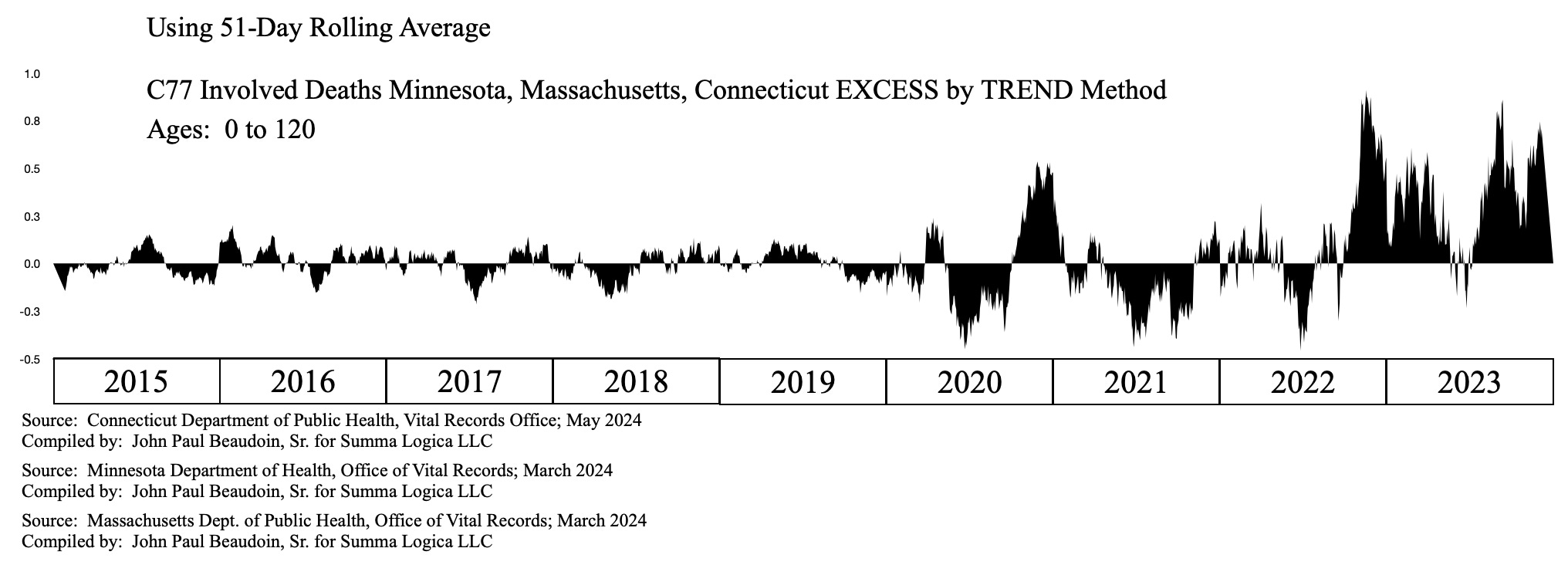 |
Figure 2
Figure 2 depicts a 3-state aggregated excess of C77 lymph node cancer involved deaths over a nine-year span from 2015 through 2023.
Methodology —“EXCESS by TREND” is calculated by first taking the 51-day rolling average of each year and state. Then sum the three states for each day. Then use 2015 - 2019 as the base years to determine a linear approximation using SLOPE and INTERCEPT functions in a spreadsheet. For example, (March 18, 2020 expected value) = INTERCEPT(value(March 18, 2015 … March 18, 2019)) + 5 * SLOPE(value(March 18, 2015 … March 18, 2019)). 2021 would use 6 as a multiplier for the SLOPE and so forth. Then calculate the excess for each day by subtracting expected from actual.
Clearly, Figure 2 depicts tremendous excess in late 2022 and throughout 2023, except a couple months in the summer.
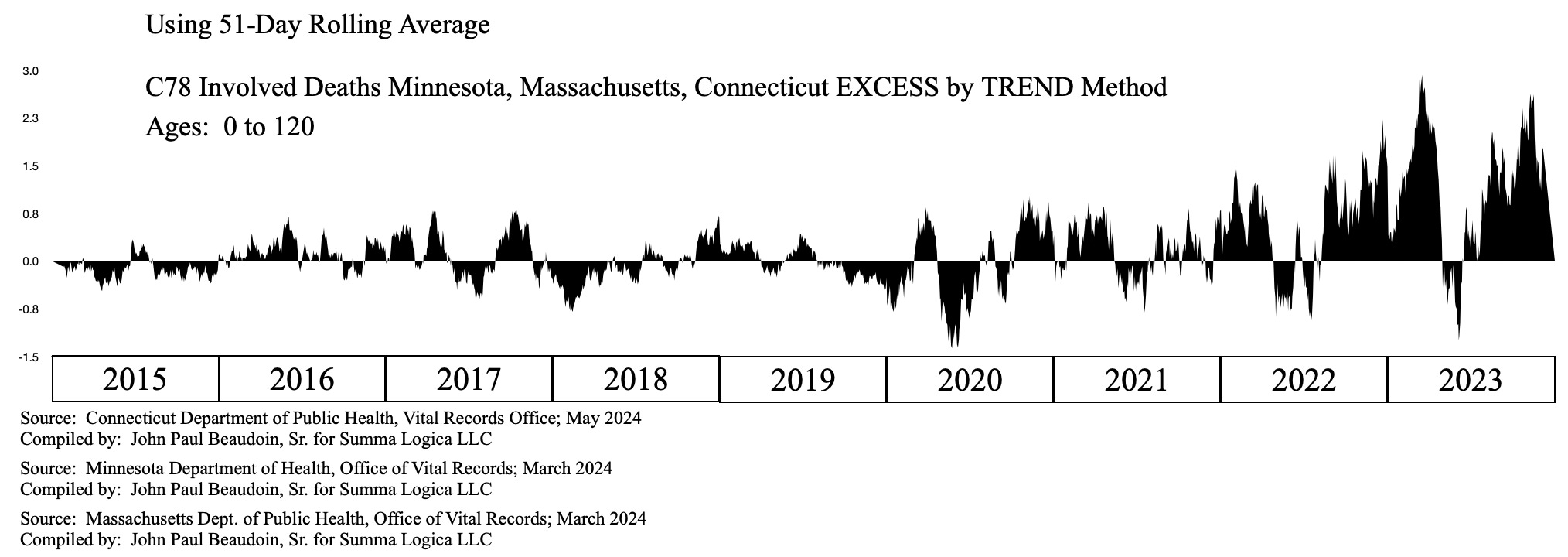 |
Figure 3
Figure 3 depicts the excess for C78, which is “Secondary malignant neoplasm of respiratory and digestive organs.” Again, Figure 3 shows the same pattern of cancers in great excess beginning in 2022 and ramping through 2023, except the summer.
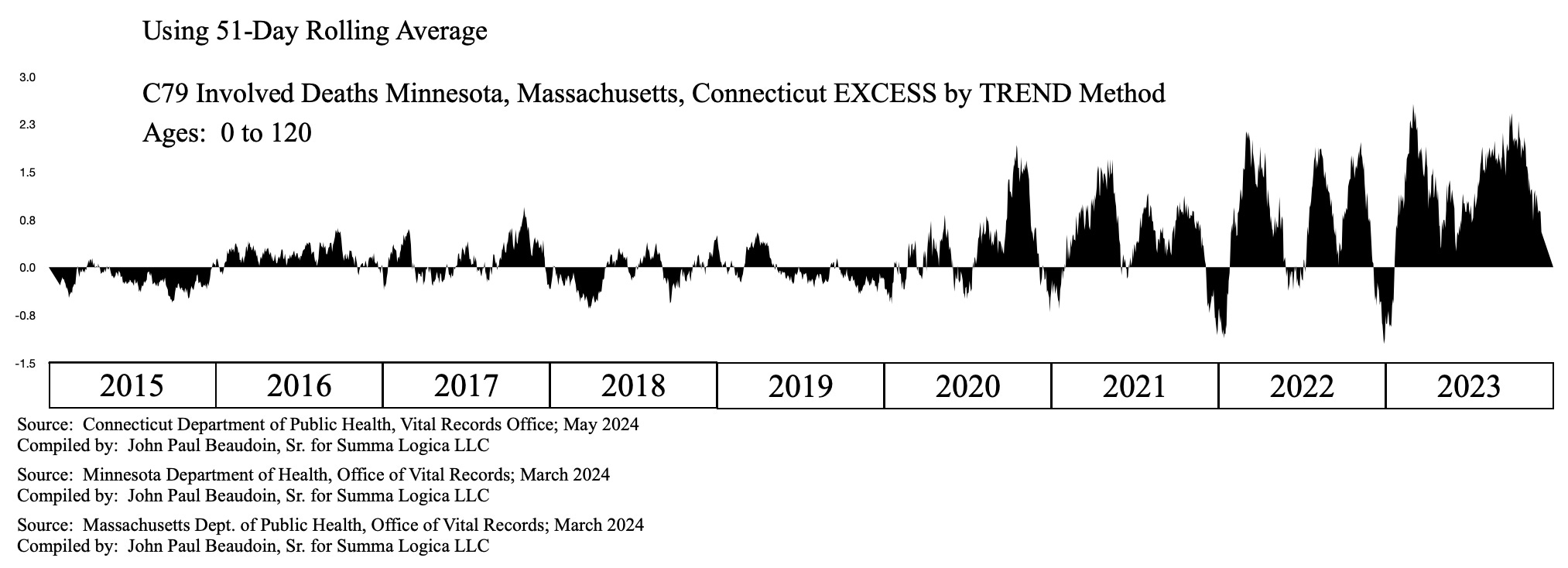 |
Figure 4
Before moving to the immune mechanism, Figure 4 depicts the excess for C79, which is “Secondary malignant neoplasm of other and unspecified sites.” Year 2023 has significantly more excess than all other years, probably close to double. 2022 was also substantially in excess.
Beyond reasonable doubt there is a malignant neoplasm issue in states 1,300 miles apart.
The Immune Mechanism
The common wisdom is that the immune system is down-regulated or dysregulated by the covid vaccine, thus allowing cancer cells to survive and multiply. Cancer cells form in every person every day. The immune system usually destroys them. If the immune system is impaired, then cancers will grow. This makes sense. I do believe the increase in the incidence rate of cancers is caused by an impaired immune system that was, in turn, set to be impaired by Covid gene drugs called “vaccines.”
Are the immune system involved deaths anomalously in excess?
The ICD-10 Code prefix “D8” represents, “Certain disorders involving the immune mechanism.”
 |
Figure 5
Figure 5 depicts a 3-state aggregated excess of D8 involved deaths. Something is clearly wrong with the immune mechanism since near the end of 2020.
However, even if I agree that immune dysregulation causes more instances of cancers, that does not explain the “turbo” aspect, which is a much faster growth rate than normal. People who were told they had 10 years to live died in 5 months or were told they had 9 months and died in 9 weeks. People who were in remission 15 years suddenly went stage 4 metastatic and died in months.
Angiogenesis is the formation of new blood vessels. Immune dysregulation may be the cause of greater instances of cancers, but angiogenesis is likely the cause of the “turbo” aspect of cancers. There can be two things happening at once. Both may be from Covid vaccines, but each may be caused by a different coincident Covid vaccine-caused mechanism.
Assume that a tumor grows beyond the size of a grain of rice. Can it grow faster than normal without a good blood supply? The tumor generally cannot grow fast without angiogenesis that provides a good blood supply.⁵ Scientists consider the interaction of the P53 tumor suppressor gene in angiogenesis as found in Ravi, R. (2000).⁶ Scientists also discuss the effects of the “semian virus 40 large T (SV40T) oncogene” in angiogenesis in Lugano, R. (2020).⁷ Lugano references the “angiogenic switch” that turns on “tumor vascularization” found in Hanahan, D. (1996).⁸
Coincidentally, back in early 2023, Kevin McKernan rocked the science world when he found the SV40 promoter in the Pfizer Covid gene drug therapies called “vaccines.” McKernan and many others have been writing about the SV40 since then.⁹
I had an idea to look at all tissue growth requiring angiogenesis and not just malignant neoplasms. If the SV40 promoter is involved in angiogenesis causing faster tissue growth, then it will also manifest in benign neoplasm and granulation tissue.
Is there evidence of excess benign neoplasms since covid vaccines were introduced?
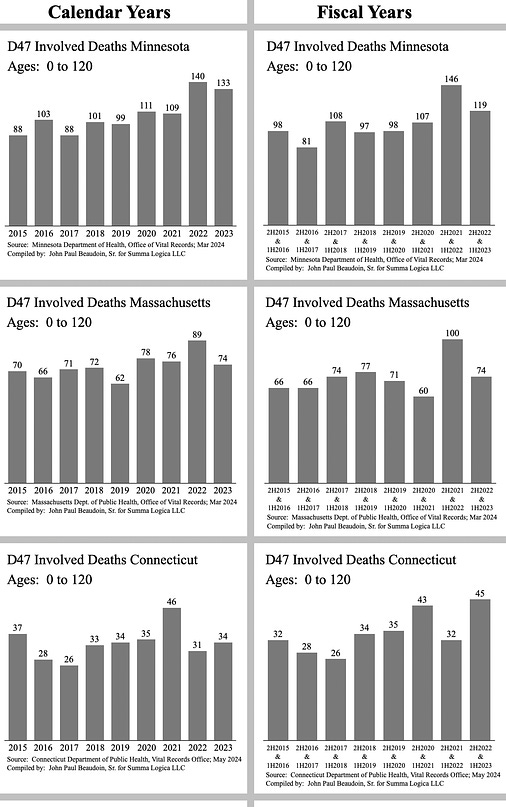 |
Figure 6
Figure 6 depicts deaths involving D47 prefix, which is, “Other neoplasms of uncertain or unknown behavior of lymphoid, hematopoietic and related tissue.” D47 prefix includes: D47.0 Histiocytic and mast cell tumors of uncertain and unknown behaviour, D47.1 Chronic myeloproliferative disease, D47.2 Monoclonal gammopathy of undetermined significance (MGUS), D47.3 Essential (hemorrhagic) thrombocythaemia, D47.4 Osteomyelofibrosis, D47.5 Chronic eosinophilic leukaemia [hypereosinophilic syndrome], D47.7 Other specified neoplasms of uncertain or unknown behavior of lymphoid, hematopoietic and related tissue, D47.9 Neoplasm of uncertain or unknown behavior of lymphoid, hematopoietic and related tissue, unspecified.
Figure 6 shows interesting patterns of excess for different years in different states. Perhaps the excess 9-year graph will depict more in Figure 7.
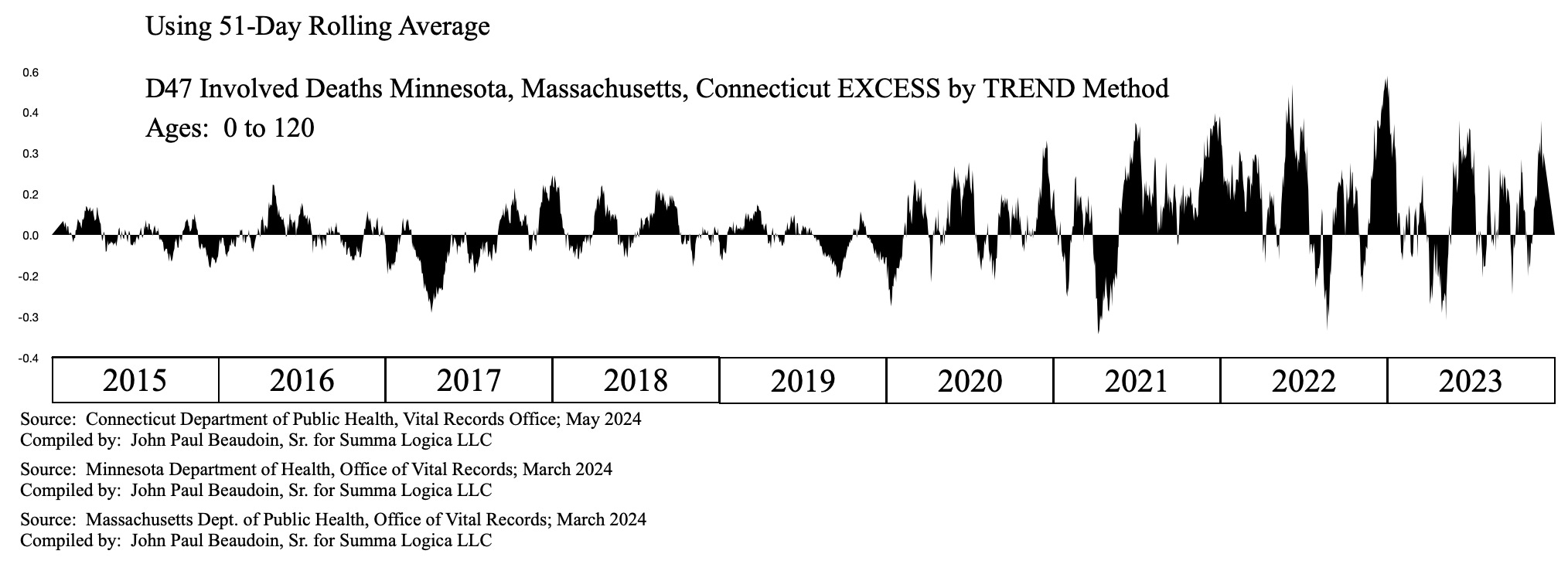 |
Figure 7
Figure 7 depicts excess prefix D47-involved deaths on a 9-year time window. Significant excess began mid-2021 and continued through mid-2022 with some nominal excess in 2023. Since benign neoplasms are generally not fatal, the waveform makes sense in that the excess would occur during acute fatal issues. People might die with benign neoplasms rather than from benign neoplasms. Of course, this is speculation. The point here is that D47 involved deaths are clearly in excess from mid-2021 through mid-2022.
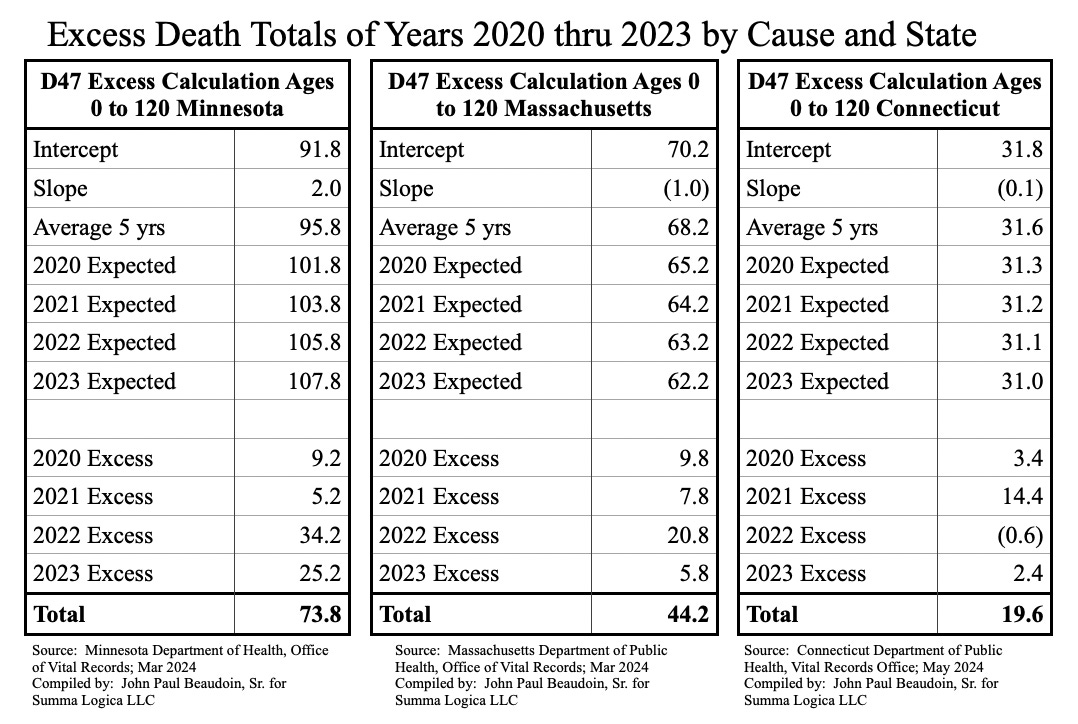 |
Table 1
Table 1 displays the number of excess deaths involving prefix D47. These are substantial numbers even when you subtract the 2020 numbers.
D37 “Neoplasm of uncertain or unknown behavior of oral cavity and digestive organs” includes lip, oral cavity, pharynx, stomach, small intestine, appendix, colon, rectum, liver, gallbladder and bile ducts, other digestive organs, and digestive organ, unspecified.
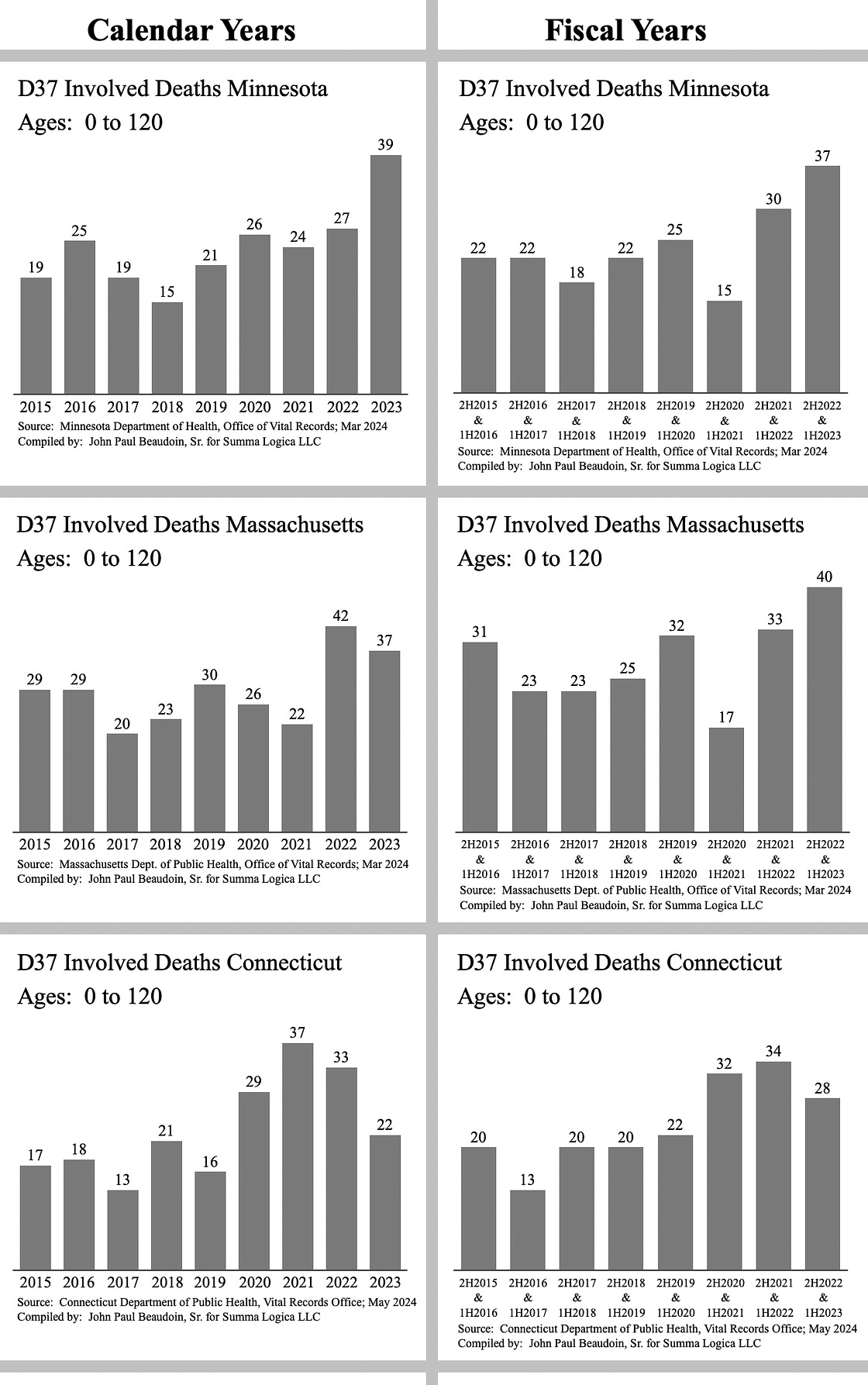 |
Figure 8
In Figure 8, Minnesota and Massachusetts depict significant 2022 and 2023 D37-involved excess deaths. Connecticut depicts 2021 and 2022 excess, but not 2023.
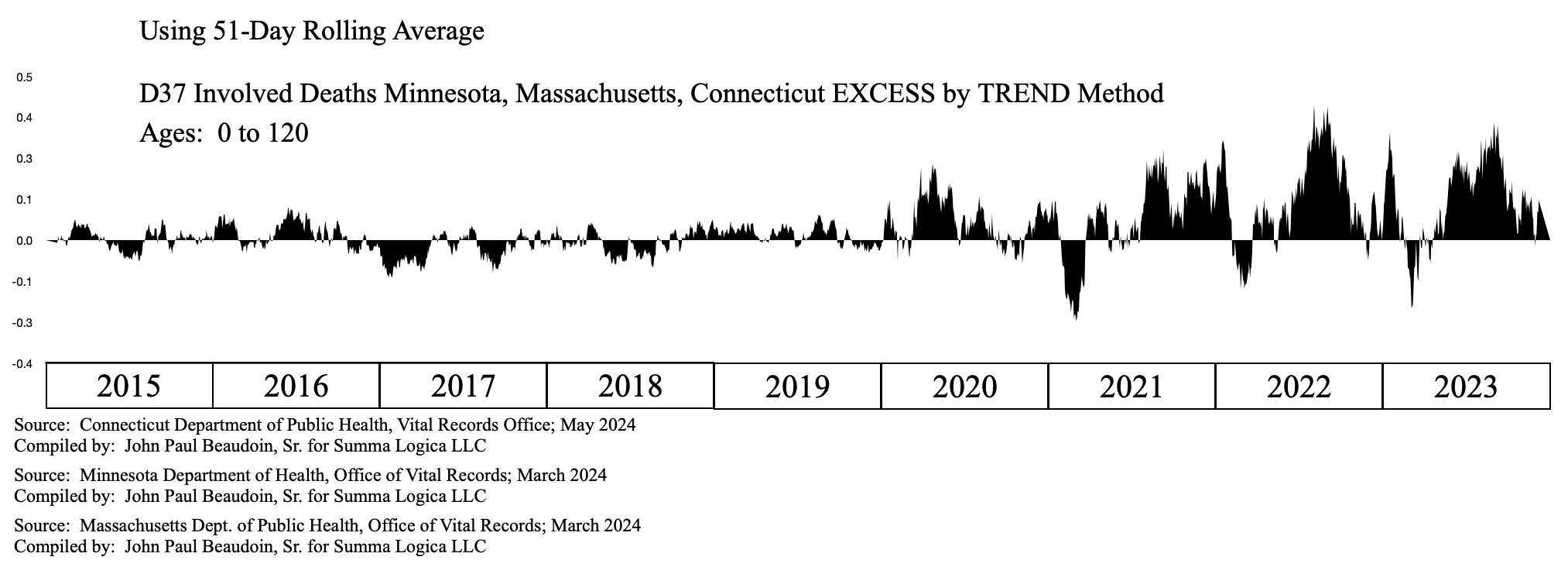 |
Figure 9
Figure 9 depicts the combined three states D37-involved deaths significant excess beginning in the middle of 2021.
 |
Table 2
Table 2 clearly shows excess D37-involved deaths in 2022 and 2023 in Minnesota and Massachusetts. An investigation of the words on the death record that lead to the ICD-10 codes generated by the CDC must be done to really understand the integrity of the data. It seems yet again that there are different customs and practices in each state.
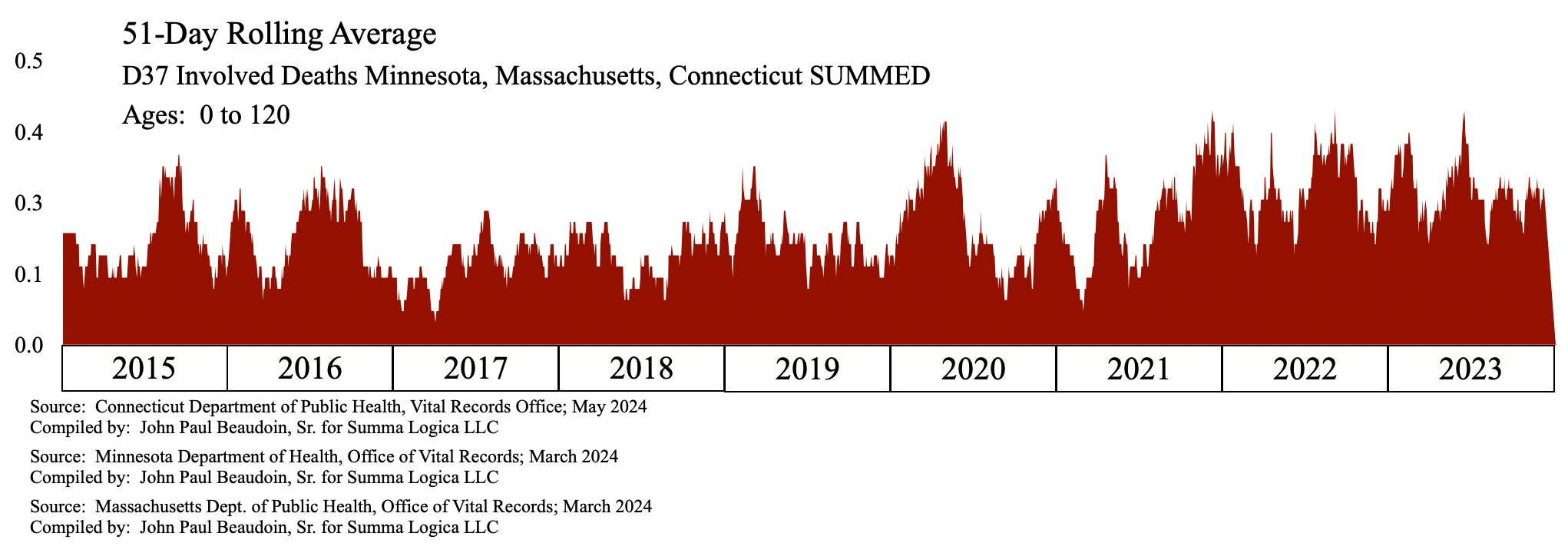 |
Figure 10
Figure 10 is an interesting view of 3-state aggregated daily deaths involving D37. Sometimes raw data can elucidate a signal if you have an eye for it. Notice the excess from mid-2021 through the end of 2023. There are a mass of solid red and higher levels of trough points after mid-2021.
D481 “Neoplasm of uncertain or unknown behavior: Connective and other soft tissue” includes connective tissue of the ear and eyelid, but not cartilage of the articular, larynx, nose, and connective tissue of the breast.
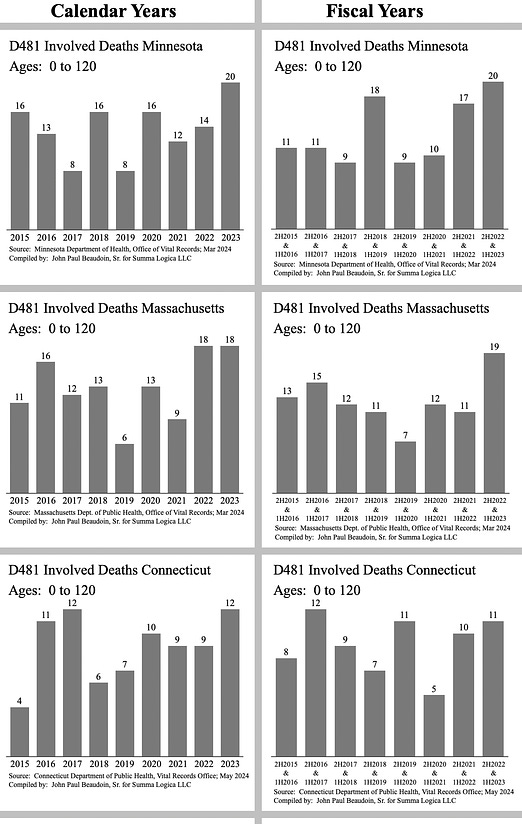 |
Figure 11
Figure 11 indicates 2023 excess D481 involved deaths in all three states and 2022 excess in Massachusetts. The years 2016 and 2017 are also anomalously high in Connecticut.
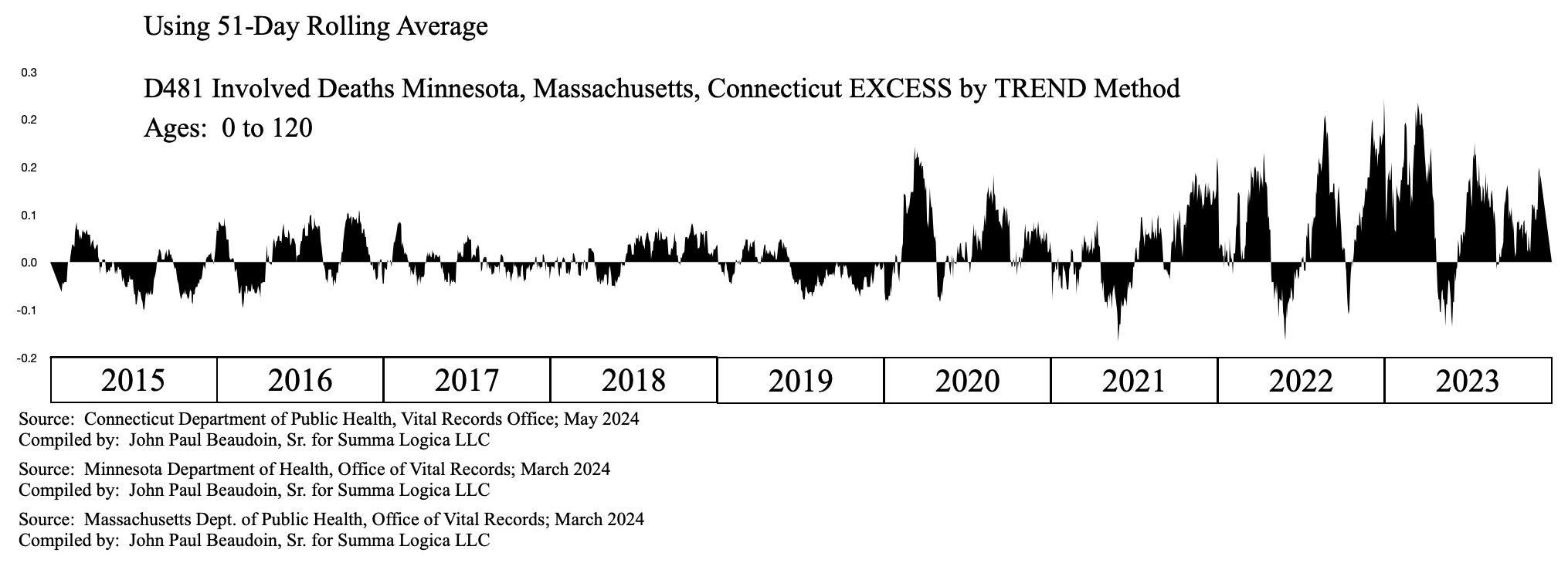 |
Figure 12
Figure 12 depicts significant D481 involved deaths excess in the 2022 to 2023 turnover.
 |
Table 3
Table 3 clearly quantifies excess D481 involved deaths in 2022 in Minnesota and Massachusetts and in 2023 in all three states.
The answer for whether there are benign neoplasm involved deaths in excess in the post-Covid-vaccination years is answered marginally, but not starkly, in the deaths involving ICD-10 Codes D47, D37, and D481.
Is there evidence of excess granulation tissue in the post-Covid-vaccination years?
Granulation tissue is defined in biology dictionary as:
Granulation tissue is reddish connective tissue that forms on the surface of a wound when the wound is healing. Clinicians observe how granulation tissue is forming on a wound in order to assess how well the injury is being repaired by the body. When too much granulation tissue forms, it is called “proud flesh”.¹⁰
The ICD-10 Code L92.8 relates to “Other granulomatous disorders of skin and subcutaneous tissue.”
 |
Figure 13
Hardly definitive, Figure 13 depicts four L92.8 involved deaths in the year 2022 across all three states whereas there were only three across all three states in seven years from 2015 through 2021. That is a ratio of 4 : 3/7ths, or 4 : 0.429, or 9.33 : 1.
The ICD-10 Code L92.9 relates to “Granulomatous disorder of skin and subcutaneous tissue, unspecified.”
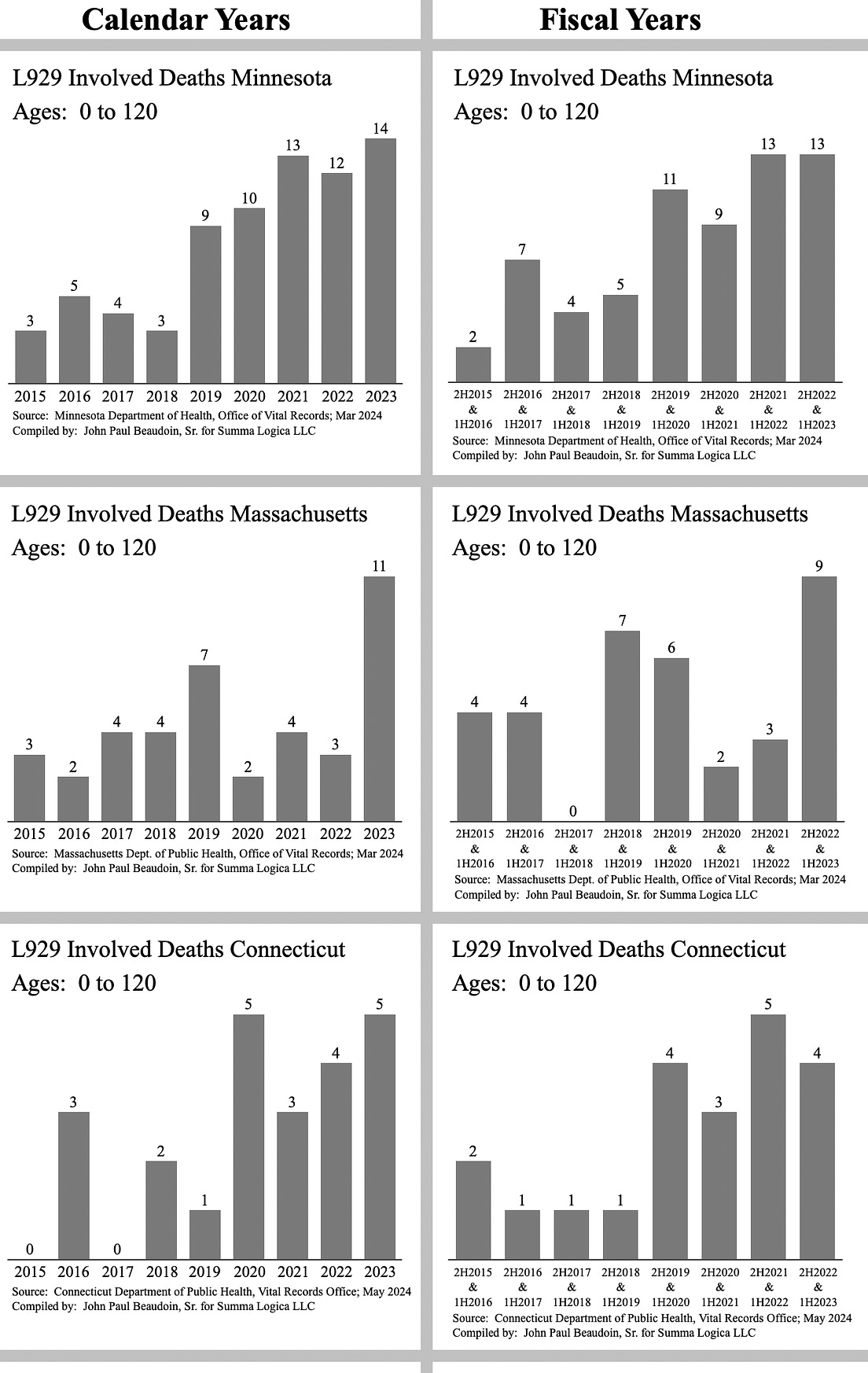 |
Figure 14
Figure 14 depicts Massachusetts excess L92.9 involved deaths in 2023. The other two states are left to the eye of the reader. These low numbers are not candidates for statistical analyses or even simple trend analysis. However, my eye sees an issue in the past few years.
One of the great values of having record-level source data (RLSD) is the ability to inspect each record individually. What are the death certifiers writing on the death records that cause the CDC’s software, TRANSAX and ACME, to generate the ICD-10 codes that they do? When the annual quantities of deaths involving a code are low, as in L92.8 and L92.9, individual inspection only takes a few more hours to complete. The results of L92.9 for Massachusetts follow.
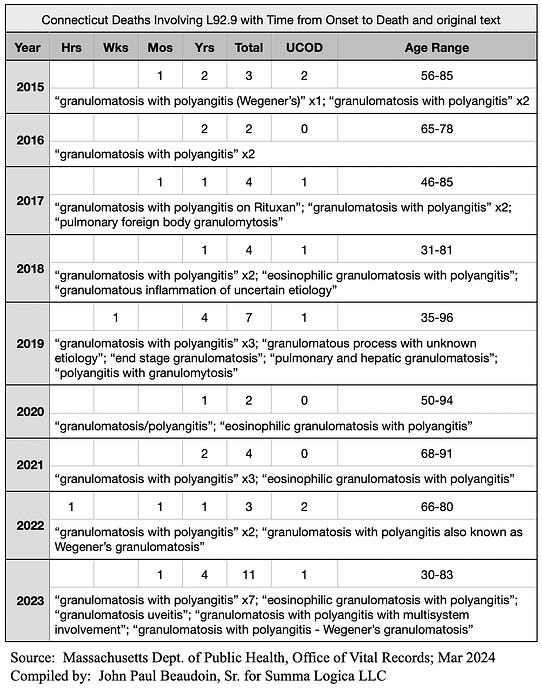 |
Figure 15
Figure 15 is a table that represents some key fields for all L92.9 involved deaths in Massachusetts from 2015 through 2023. I wanted to see if there were more instances of shorter time periods post-Covid-vaccination. There are 6 total that are under a year. Three are in years 2022 and 2023, a 2-year span. Three are in years 2015 through 2021, a 7-year span.
The words used for each record that resulted in “L92.9” are concatenated into a text field for each year. The phrases used are separated by semicolons. The number of records that contain an exact same character string, or phrase, is listed by an “x” before a number. If there is no number or “x” after the phrase, then it was found one time.
It is interesting how many times “eosinophilic granulomatosis” occurs and when. There was one each in years 2018, 2020, 2021, and 2023. Eosinophilic granulomatosis is an extremely rare autoimmune condition. Wouldn’t it be great if we had the vaccination records of all 4 of the decedents listed here. Imagine if the CDC or NIH or FDA actually their job and tracked down causality of anomalous deaths. Please remember that 2.5 years ago I proposed an easy, cheap, elegant solution to the vaccine debate. State and federal governments have all the answers on their servers. It would take about one man-week to settle the issue. But they keep the data hidden from the public. Few people demanded data from governments. Instead, health freedom people debate 4-year-old Pfizer trial data or some recent research paper.
Evidence of increased incidence rates of malignant neoplasms, benign neoplasms, granulomas, and immune mechanism impairment are depicted earlier in this article. There are no confidence intervals, p-values, or other inferential statistical methods variables. Rather than debate statistics, please simply employ human discernment, id est — think. Look at C77 involved deaths in Figure 1 and decide if there is excess.
If you agree that there is an increased incidence rate in all three types of tissue growth, then read on. You will now be confronted with the coup de grâce of evidence herein evinced.
C'est le COUP DE GRÂCE de l’évidence
Consider now evidence that has nothing to do with statistics … evidence that any human with a functional brain can see is directly linked to the Covid vaccine and very clearly required angiogenesis for it to grow so rapidly.
Is the “turbo” aspect in turbo cancer a function of the SV40 promoter’s involvement in angiogenesis? Is the “angiogenic switch” involved in benign neoplasms and granulation tissue growth?
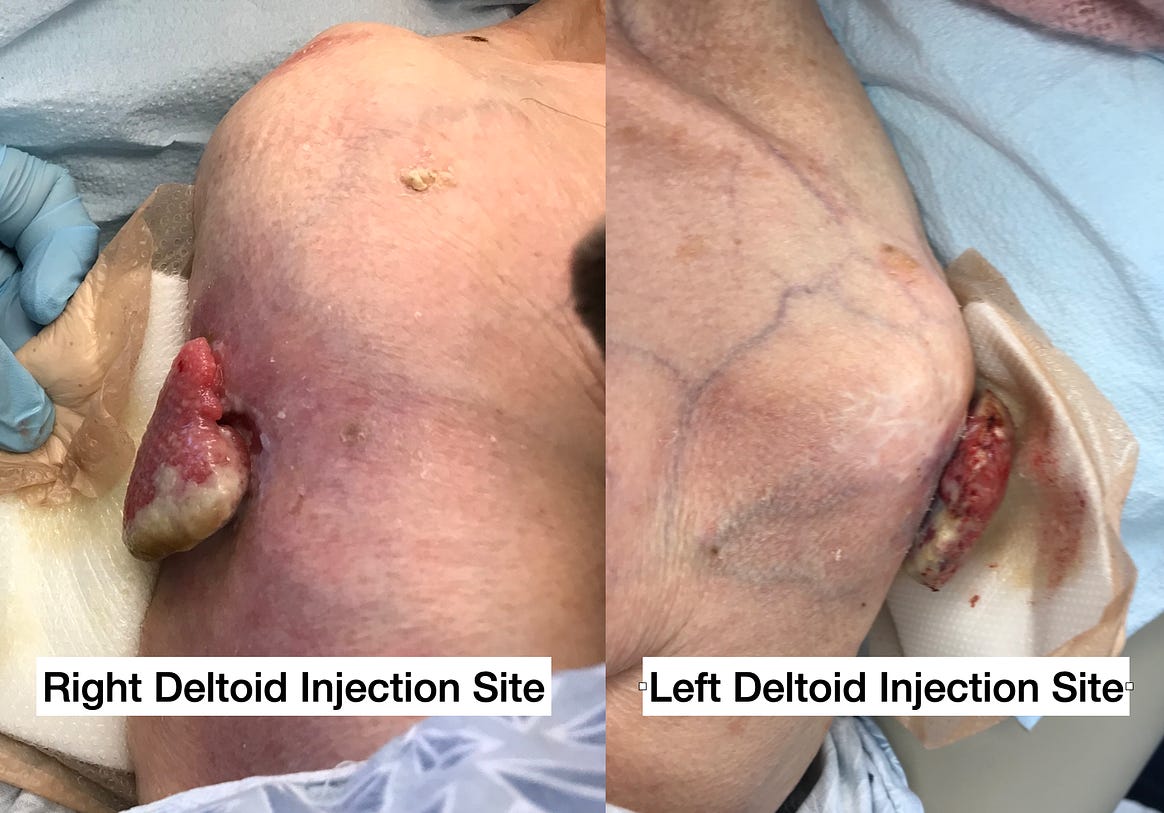 |
Figure 16
Figure 16 comprises the following subject description:
92-year-old Female
COVID-19 “vaccine” Dose 1 - January 2021
COVID-19 “vaccine" Dose 2 - February 2021
Date of pictures - July 28, 2021
Date of death - August 18, 2021
Theory: injection sites granulation tissue from both doses grew at accelerated rates in both arms to produce massive tissue growth each ~4cm diameter x ~1 cm thick in only 5 months. Angiogenesis? Darned right. SV-40 promoter involved? Seems highly likely.
This article is for regular people to understand that it’s not all about statistics and research papers. This information may make it into a research paper at some point. The message, though, is to not wait for studies and papers. Do not wait for science™. Science™ was never meant to be a gating factor in emergency or imminent decision making. Doctors are not scientists despite medical schools trying to con them into believing they are. Patients need treatment, not research papers and science™. The difference between practicing medicine and practicing science™ has been lost thanks to Evidence Based Medicine (EBM).
Conclusions
Incidence rates of cancers, benign tumors, and granulomas increased since Covid vaccinations.
Growth rates of two granulomas at the Covid vaccination sites are evidence beyond reasonable doubt that the Covid vaccination played a part in the formation of the granuloma. The speed of growth was anomalously “turbo.”
In the last four years, it seems that people want to be told what to think rather than receiving facts and forming one’s own opinion. What do you understand from this article? Are you convinced that “turbo” cancer is real and that it is attributed to the Covid vaccinations? Do you wonder if the SV-40 is responsibility for the “turbo” aspect of turbo cancer?
References
Beaudoin, J. (May 28, 2022). Neoplasm to ectoplasm … in months. Coquin de Chien. The Real CdC’s Newsletter. Substack. Found here https://therealcdc.substack.com/p/neoplasm-to-ectoplasm-in-months on September 20, 2024.
Beaudoin, J. (Oct 23, 2022). Hidden CANCER signals = FOUND. Coquin de Chien. The Real CdC’s Newsletter. Substack. Found here https://therealcdc.substack.com/p/hidden-cancer-signals-found on September 20, 2024.
Beaudoin, J. (May 01, 2023). Lymph. Coquin de Chien. The Real CdC’s Newsletter. Substack. Found here https://therealcdc.substack.com/p/lymph on September 20, 2024.
Beaudoin, J. (Sep 01, 2023). Lymph Node Cancer Update. Coquin de Chien. The Real CdC’s Newsletter. Substack. Found here https://therealcdc.substack.com/p/lymph-node-cancer-update on September 20, 2024.
Saman, H., Raza, S. S., Uddin, S., & Rasul, K. (2020). Inducing Angiogenesis, a Key Step in Cancer Vascularization, and Treatment Approaches. Cancers, 12(5), 1172. Found here https://doi.org/10.3390/cancers12051172 on September 29, 2024.
Ravi, R., Mookerjee, B., Bhujwalla, Z. M., Sutter, C. H., Artemov, D., Zeng, Q., Dillehay, L. E., Madan, A., Semenza, G. L., & Bedi, A. (2000). Regulation of tumor angiogenesis by p53-induced degradation of hypoxia-inducible factor 1α. PMC PubMed Central. Found here https://www.ncbi.nlm.nih.gov/pmc/articles/PMC316350/ on September 29, 2024.
Lugano, R., Ramachandran, M., & Dimberg, A. (2020). Tumor angiogenesis: causes, consequences, challenges and opportunities. Cellular and molecular life sciences : CMLS, 77(9), 1745–1770. Found here https://doi.org/10.1007/s00018-019-03351-7 on September 29, 2024.
Hanahan, D., Folkman, J. (1996). Patterns and Emerging Mechanisms of the Angiogenic Switch during Tumorigenesis. Cell, Volume 86, Issue 3, 353 - 364. Found here https://www.cell.com/cell/fulltext/S0092-8674(00)80108-7?_returnURL=https%3A%2F%2Flinkinghub.elsevier.com%2Fretrieve%2Fpii%2FS0092867400801087%3Fshowall%3Dtrue on September 29, 2024.
McKernan, K. aka Anandamide. (Apr 10, 2023). Sequencing of bivalent Moderna and Pfizer mRNA vaccines reveals nanogram to microgram quantities of expression vector dsDNA per dose. Nepetalactone Newsletter. Substack. Found here https://anandamide.substack.com/p/sequencing-of-bivalent-moderna-and on September 29, 2024.
(2024). Granulation Tissue. biology dictionary. Found here https://biologydictionary.net/granulation-tissue/ on October 3, 2024.
The Real CdC’s Newsletter is free today. But if you enjoyed this post, you can tell The Real CdC’s Newsletter that their writing is valuable by pledging a future subscription. You won't be charged unless they enable payments.
![]()
![]()
No comments:
Post a Comment