The HPV Vaccine Tragedy Was A Test Run For COVID-19
A review of the incredible dangers of the HPV vaccine and the unscrupulous campaign that forced it upon the world

Story at a Glance:
•Two decades ago, Merck pushed Vioxx, a lucrative NSAID onto the market despite knowing it would caused a large number of heart attacks. Merck eventually faced so many lawsuits they had to withdraw it, at which point they rushed, Gardasil, a lucrative HPV vaccine to market to cover their losses.
•Gardasil was extremely dangerous. However, just like Vioxx, both Merck and the FDA ignored that data and did all they could to promote it. This continued even after Gardasil brought forward a wave of crippling injuries unlike anything that had previously been seen for a vaccine.
•Remarkably many of Gardasil’s issues (e.g., autoimmunity, POTS, infertility, death) are identical to those seen with the COVID-19 vaccines. In turn, there are remarkable parallels to how they were approved (e.g., doctored trials covered up a wave of injuries) and how far the FDA and CDC went to protect those products from scrutiny.
•In this article we will review the dangers of the HPV vaccine, why it was so dangerous, how it frequently caused rather than prevented cervical cancer, and how the immense malfeasance of the FDA and CDC provides critical lessons for understanding what unfolded during COVID-19.
Prior to the COVID-19, I considered Gardasil (for HPV) to be the most dangerous and unjustifiable vaccine on the market. In turn, it’s truly remarkable how many parallels can be found between it and how the COVID-19 vaccines were handled so I feel it’s critically important for this forgotten story to be unearthed.
Help Pay for Vioxx (HPV)
Before there was Gardasil, there was Vioxx,” said Mr. Kennedy after filing a Gardasil lawsuit with Wisner Baum in 2020. “Merck paid billions to settle civil allegations that it purposely hid Vioxx’s cardiovascular risks. The company also paid $950 million in fines as a result of their criminal conduct. When Gardasil came along, the boardroom at Merck joked that its HPV vaccine could ‘Help Pay for Vioxx.’ Sure enough, some of the same shadowy cast of characters who were involved in the Vioxx scandal worked on Gardasil, and they employed the very same methods of manipulating science and obscuring risks as they did with Vioxx. And just as with Vioxx, Gardasil has left a calamitous health disaster in its wake.
The default strategy in Medicine for any type of pain or injury is to throw NSAIDs at it—making the drugs immensely profitable. Unfortunately, they typically don’t help that much (which actually increases their sales since this marginal efficacy results in people perpetually using large amounts of them), and they are fairly dangerous (e.g., NSAIDS kill tens of thousands of Americans each year and seriously injure far more).
Note: a major reason why I’ve been trying to expose the DMSO story is because DMSO can be used in virtually every situation where an NSAID is, but is significantly more effective at treating the problems and unlike the NSAIDs, is not dangerous.
Since one of the most common reasons NSAIDs lead to hospitalization is the drugs causing (sometimes fatal) gastric bleeds, an attempt was made to make NSAIDs less toxic by having them being more selective in what they targeted—which made them less likely to cause gastric bleeding but simultaneously much more likely to cause heart attacks and strokes (and did not change the rates of kidney injuries—another common and serious complication of NSAIDs).
As a result, from the start, evidence began emerging that the COX-2 selective NSAIDs (Merck’s Vioxx—approved in 1999 and Pfizer’s Celebrex—approved in 1998) had a huge stroke and heart attack risk. Yet, all of that evidence was ignored (e.g., Dr. Mercola warned the public about this risk in 1999 and each year thereafter even more evidence accumulated showing Vioxx had the cardiovascular risk).
However, rather than pull the drug, Merck (with the FDA’s complicity) kept on finding ways to cover that data up,
and ultimately only withdrew Vioxx in 2004 once so much data had
emerged it become impossible to continue covering it up Vioxx was
estimated to have killed 120,000 people, while Celebrex (which was never taken off the market) to have killed 75,000.
This sets an important context. First, consider the congressional testimony of the FDA scientist who was largely responsible for getting Vioxx from the market. In it, he notes that the FDA is incredibly resistant to withdrawing bad drugs it approved to the market, and in the case of Vioxx, repeatedly swept evidence of it’s harm under the table and repeatedly silenced agency scientists who tried to warn of its dangers. The most important aspect of this testimony was his conclusion, where he stated it was inevitable future highly dangerous drugs (e.g., those causing blood clots and heart attacks) would also be kept on the market by the FDA.
The second is that a lot of lawsuits were subsequently levied against Merck (ultimately resulting in a 5 billion dollar settlement) which put them in a bit of a pinch where they needed to find a new source of (liability free) revenue.
Note: the year Vioxx was pulled (2004), Merck’s stock dropped by 28% but its CEO nonetheless received a $37.8 million “performance based” bonus.
That solution after decades of work
had at last made a long term goal of vaccinologists possible, a vaccine
that could prevent human papilloma virus infections—an incredibly
lucrative market since 85% of the population gets HPV and it was linked to cancer—thereby making it possible to sell a vaccine against cancer!
Note: there were also decades of failed attempts to make a SARS (coronavirus) vaccine.
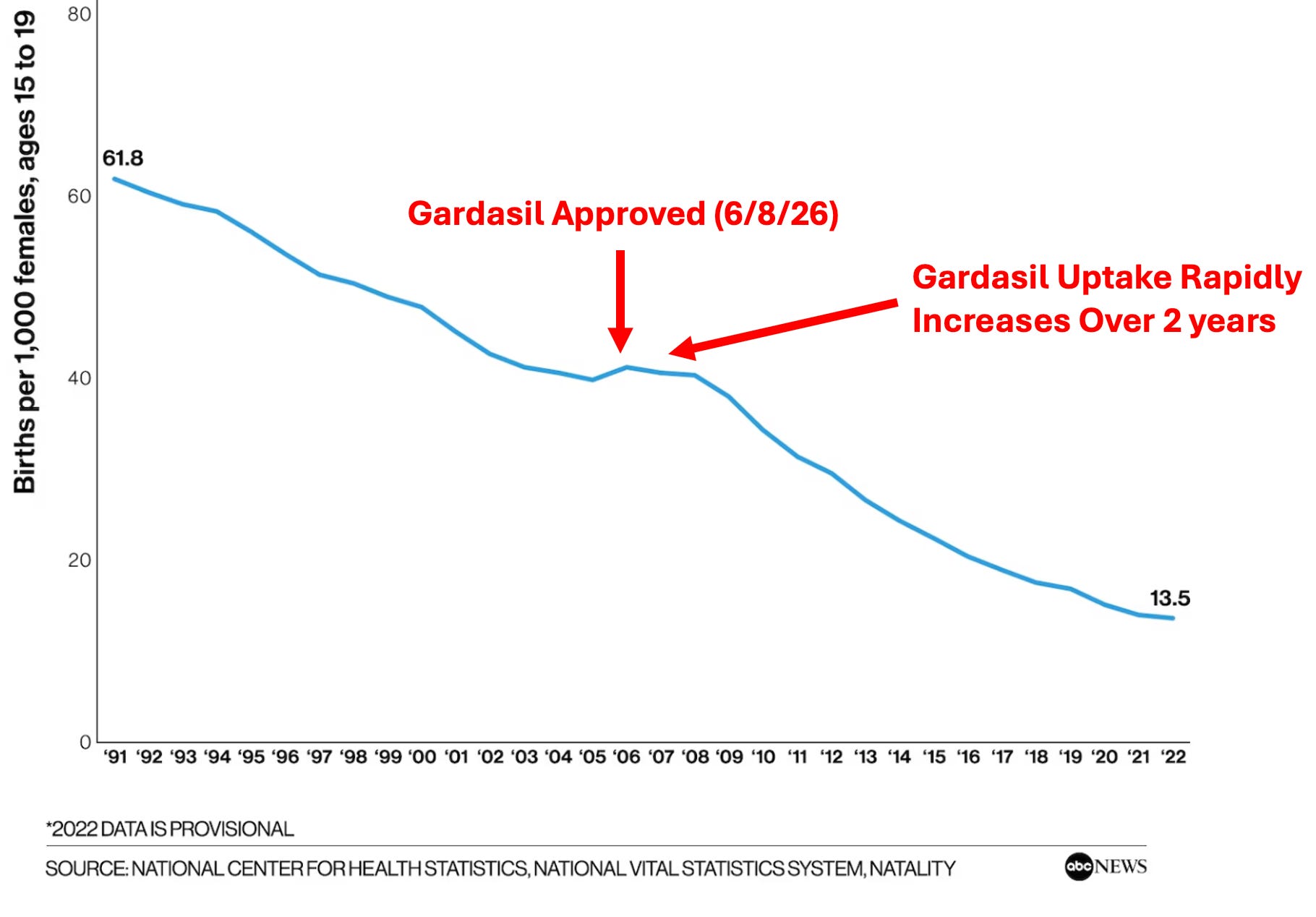
In turn, once Gardasil (Merck’s HPV vaccine) was approved in 2006, it was immediately added to the vaccine schedule, and an advertisement blitz was done across America to convince everyone they needed to be scared to death of HPV and needed the vaccine.
Note: Merck’s One Less Campaign (which has many more advertisements than just these 3) won numerous awards for being the “best advertising campaign of the year.”

This campaign was incredibly effective (e.g., before long, I started encountering many children and parents who were terrified of HPV) and resulted in 25.1% of adolescent girls getting it in 2007, by 2011, 53.8% and by 2023, 79.3%. This was great for Merck, since beyond requiring 2-3 doses, at the time the vaccine was launched, it was the third most expensive vaccine on the market (with the two more expensive ones also being made by Merck).
Lastly, a lot of money was spent on alternative advertising approaches (e.g., the HSS spent 40 million funding grants to come up with research to give doctors talking points and scripts to push more parents to vaccinate). Similarly, many campaign paid girls to get the HPV vaccine (e.g., one targeted women ages 16-18). This is similar to how the HSS paid major media networks hundreds of millions to advertise the COVID vaccines and how an endless number of absurd gimmicks or cash prizes were offered to get the COVID vaccine (which included a few that were so unbelievable I had to compiled them here).
Note: with a current wholesale cost of $307.61 for each injection, the HPV vaccine is now the second most expensive vaccine (with a newer RSV vaccine being number one). Likewise, Gardasil’s sales continue to grow, and in 2023, at 1.87 billion in total revenue, it was Merck’s second highest selling pharmaceutical (with the number one spot going to a cancer drug). Because of it’s high cost, it frequently required state or federal financial support for doctors to offer it (not unlike what happened with the COVID vaccines).
Is the HPV Vaccine Effective?
The reason Merck had to aggressively market the fear of cervical cancer was because it was much less of a danger than it had been in the past.

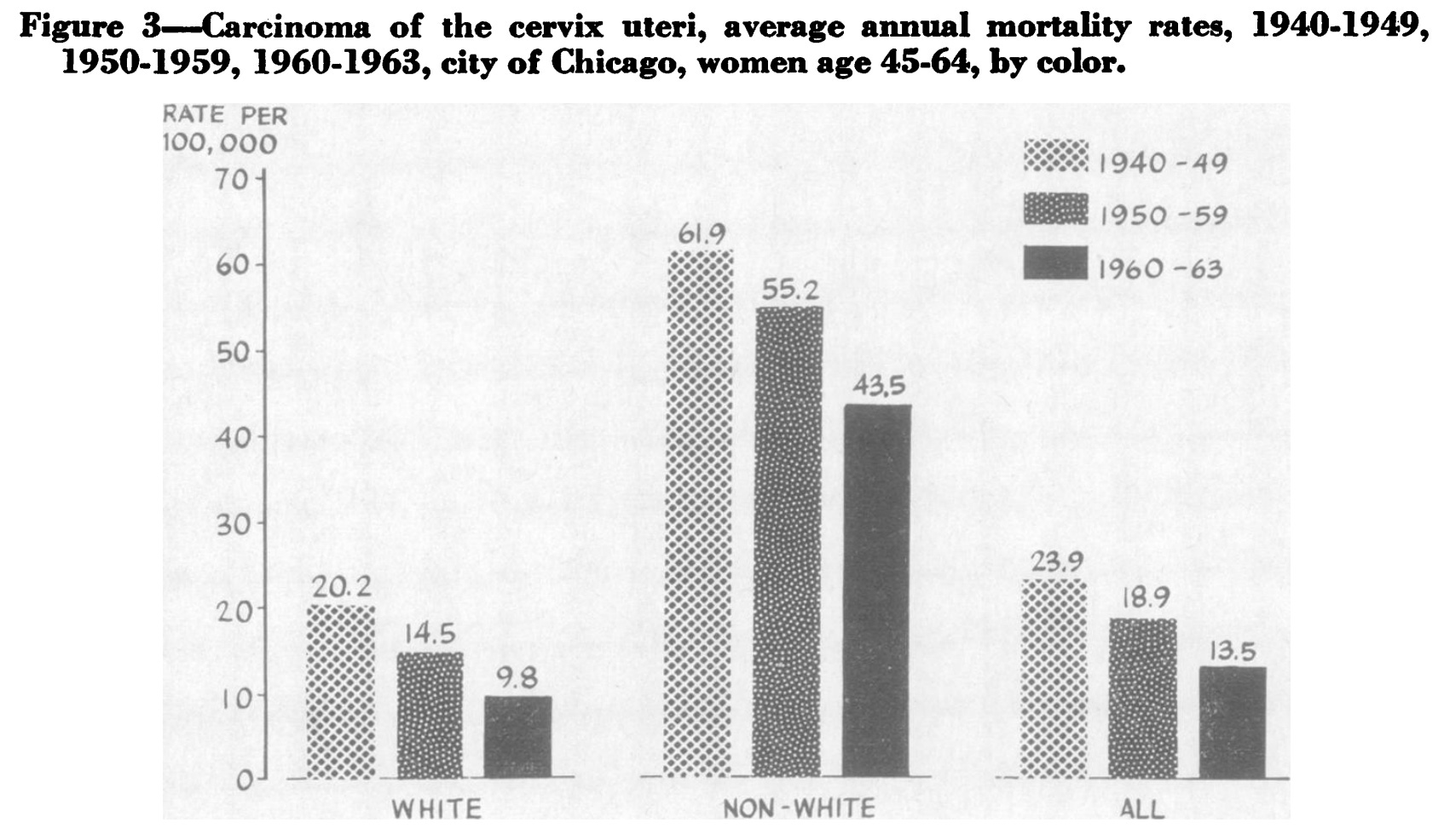
Note: while clear cervical cancer statistics prior to 1970, are harder to find, they essentially show there’s been a steady decline since the 1940s, and that the death rate used to be at least double what it was in the 1970s. This for example is part of a data set for the cancer rates in New York and Chicago:
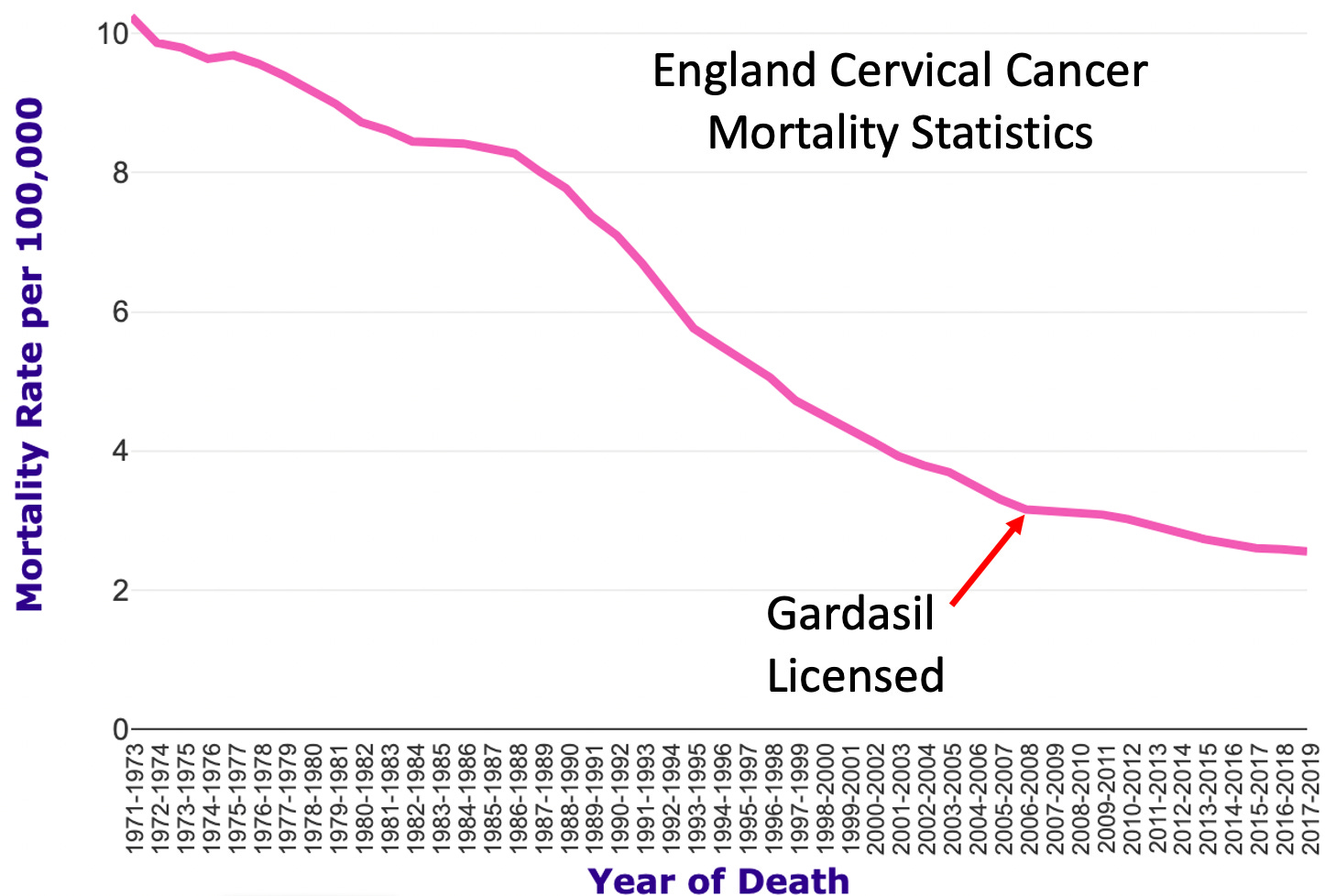
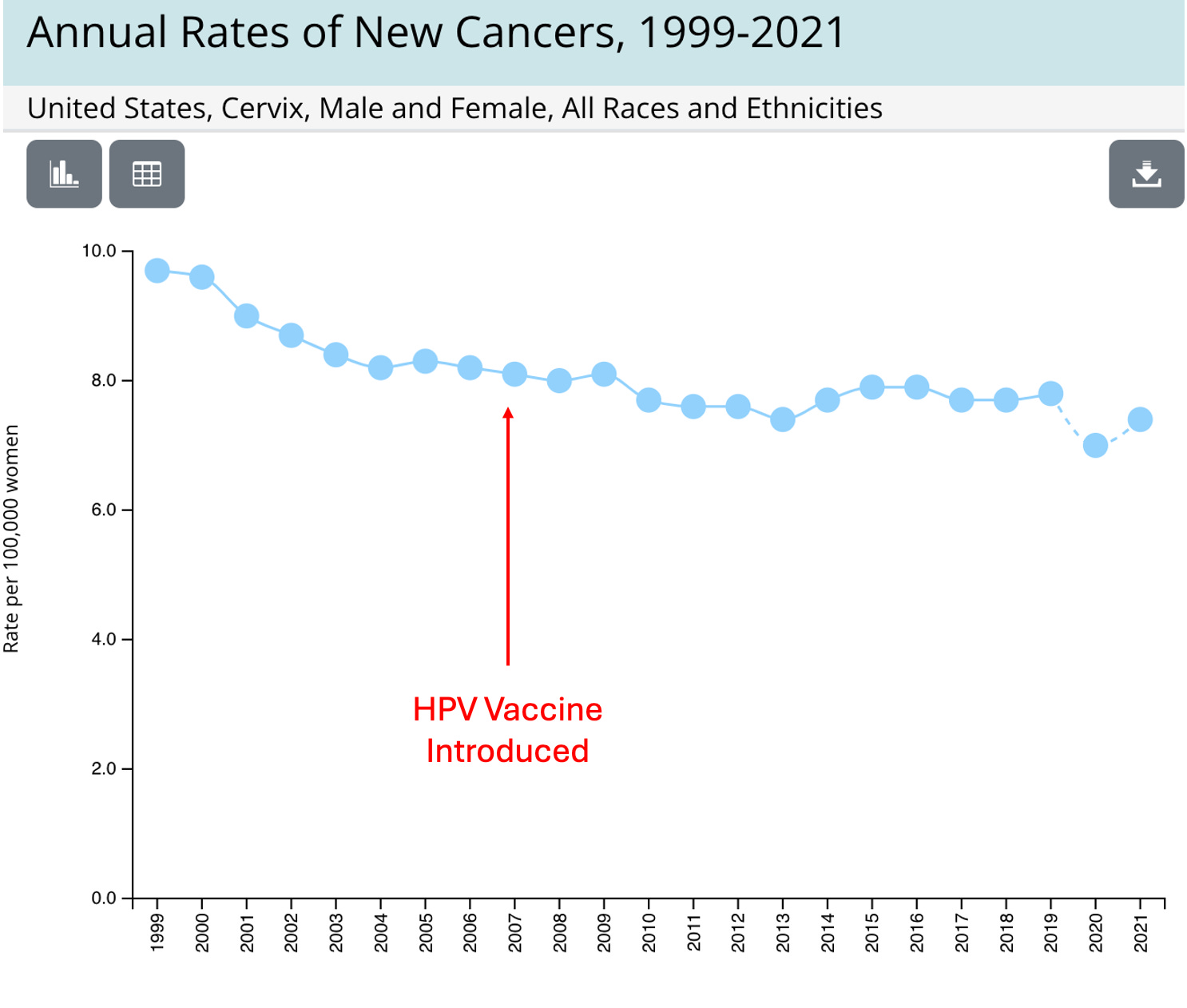
While a variety of factors accounted for this decline, much of it is credited to pap smears (which entered use in 1941 and are often considered to be the most significant advance in the control of cancer in the 20th century). In turn, you see a remarkably similar pattern with the HPV vaccine’s adoption that you see with many other vaccines, where most of the decline they are credited with actually began long before the vaccine was introduced:
According to the Annals of Medicine: “At present there are no significant data showing that either Gardasil or Cervarix (GlaxoSmithKline) can prevent any type of cervical cancer since the testing period employed was too short to evaluate long-term benefits of HPV vaccination.”
The basic issues with the HPV vaccine were:
•The
belief HPV was responsible for cervical cancer originally arose from
observing HPV associated cancers emerge in severely immune suppressed
individuals (e.g., those with AIDS). In contrast, most people get HPV
and and clear it (e.g., 85% of the population gets an HPV infection
whereas 0.008% of women get cervical cancer each year).
•In
the clinical trials that got Gardasil’s approval, Merck argued that the
decrease of the rates of precancerous lesions would translate to a
reduction in cervical cancer (which as the above data shows never
appeared in the general population—and rather you can potentially argue
it increased the cancer rates as the existing decline slowed once it was
introduced).
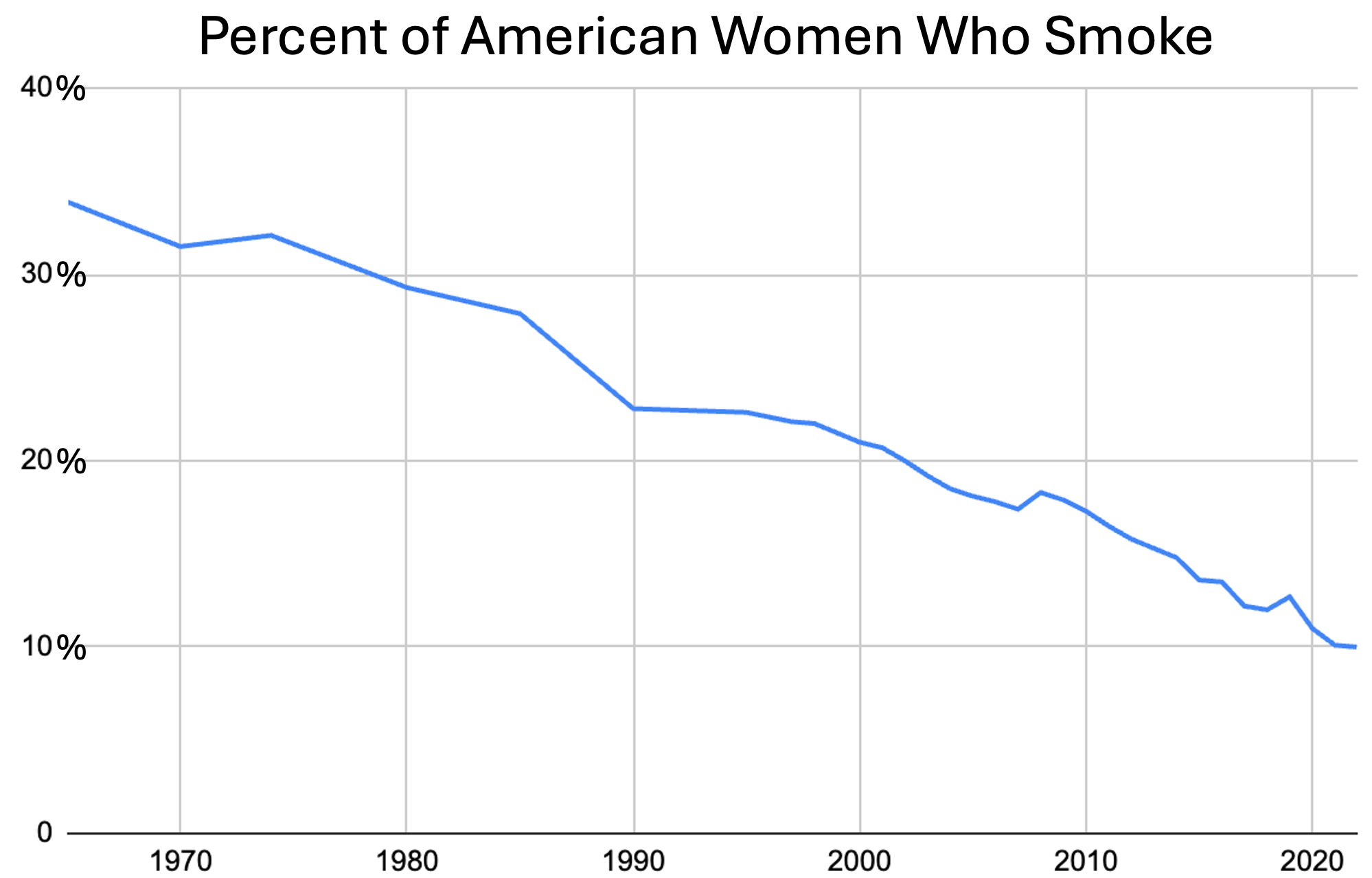
•Two of the primary risk factors for cervical cancer are smoking and using birth control pills (which both roughly double your risk for cervical cancer). The recent focus on HPV unfortunately has largely removed these major risk factors from the discussion, or for example noticing the decline in cervical cancer (e.g., the previously cited English cervical cancer mortality statistics) directly parallels the decline in female smoking rates:
Conversely, there are numerous data sets that show those who get the HPV vaccine are less likely to get cervical cancer (e.g., this recent one showed a 30% decrease in cervical cancer in those who were vaccinated). Presently, I am not sure if this reduction is due to the vaccine reducing cervical cancer, cherry picking data, or those who vaccinate being healthier in general (e.g., not smoking), as the overall decrease that would be expected to appear in cervical cancer rates from an “incredibly effective vaccine” never actually did.
Note: it’s so easy to rearrange data that on controversial topics, it’s often necessary to look at the overall data which is hard to distort rather than specific pieces of it (e.g., the COVID vaccines “prevented COVID deaths” but simultaneously, after they were deployed there was a massive spike in COVID cases and in many cases deaths as well).
Disease Provocation
Vaccines place the body under stress and divert the immune response to addressing the vaccine’s stimulus. If the immune system is already attempting to contain another infection, this can be quite problematic and allow the existing infection to spiral out of control. This phenomenon has been known about since at least 1893, demonstrated with many different infections (which I compiled here), was responsible for numerous disease outbreaks (e.g., polio outbreaks often followed diphtheria or pertussis vaccination campaigns), and was even used by militaries to test for silent typhus infections so those outbreaks would not spread through an army (as those already infected with typhus would become severely ill after receiving a typhus vaccine).
I’ve long suspected this also applies to the influenza vaccine as it has the optimal design for causing disease provocation (a small number of antigens alongside a zeta potential disrupting adjuvant) and I have lost count of how many times I’ve the people around me (e.g., my classmates in medical school) get ill with the flu after receiving the a flu shot. In turn, it has always been extremely frustrating for me to see those concerns to be dismissed in a condescending manner that states the flu vaccines do not contain any live influenza viruses and thus “cannot give you the flu.”
Note: this review, this study, this study, and this study show individuals who get a flu shot for a strain different than the circulating one (which is what typically happens) are more likely to get a viral respiratory infection (e.g., the flu).
Likewise, during COVID-19, I began running into numerous reports of individuals in my social circle becoming severely ill with COVID-19 immediately after receiving a COVID vaccine (and sometimes dying from the infection in the hospital). In addition to my direct observations, I also found a report from a survey Steve Kirsch had me evaluate of a paramedic who had a PCR confirmed COVID infection, felt fine, got the vaccine, immediately crashed and then had a severe illness along with this report:
Similarly, in vaccine injury reporting datasets, COVID-19 was one of the most cause of death reported after a COVID vaccine.
Note: disease provocation used to be a widely recognized concept in vaccinology, but was essentially buried, something I suspect resulted from it getting in the way of vaccine sales (since the acknowledgment this could occur shatters the “safe and effective” narrative, and makes it impossible to rapidly vaccinate whoever is in front of you as they first must be tested for the disease). The entire concept and history of vaccine provocation is immensely interesting and hence was summarized here.
One of the major issues with the HPV vaccine was it provoking infections of the most dangerous (cancer causing) types of HPV, which for example, was shown in the data Merck submitted to the FDA.

Note: an identical effect was also found with GlaxoSmithKline’s competing HPV vaccine Cervarix. In a previous article on the subject of disease provocation, I took a deeper dive on the HPV vaccine data.
Likewise, after the vaccine came out, I ran across a few people (e.g., a close friend) who either developed an HPV infection (one of whom had never had sexual intercourse) or had already existing genital warts rapidly become much much worse. Similarly, when Judicial Watch investigated the HPV vaccine, they identified 78 VAERS report where this had happened. For example:
Two days after receiving the first dose of Gardasil, the patient developed groin warts. There is no known history of these warts. The patient came back in about a month later and was given the second dose of Gardasil. A few days after receiving the second dose, the patient had a huge outbreak of warts.
Information has been received from a consumer concerning her 17-year-old daughter with no medical history and an allergy to sulfa, who on 28-SEP-2007 was vaccinated with a first dose of Gardasil . . . Prior to being vaccinated with Gardasil the patient was tested for HPV and genital warts and all her test came back negative. On 15-OCT-2007 the patient experienced a fever, and broke out with white bumps that were diagnosed as genital warts.
Furthermore, wart outbreaks (that were sometimes quite severe) also occurred on the face, hands, and feet and sometimes were from other papilloma virus strains. For example:
A 16-year-old female . . . was vaccinated with Gardasil. Subsequently, on an unspecified date the patient developed warts on hands after receiving Gardasil. Medical attention was sought. The patient's warts on hands persisted.
My daughter began to have facial (flat) warts on her face and chest after the 2nd dose of Gardasil. There are many warts on her face and chest at least 20 or more. She has never had this problem before receiving the vaccine. She was treated for warts by her Doctor and now has been referred to Dermatology. She has not recovered yet.
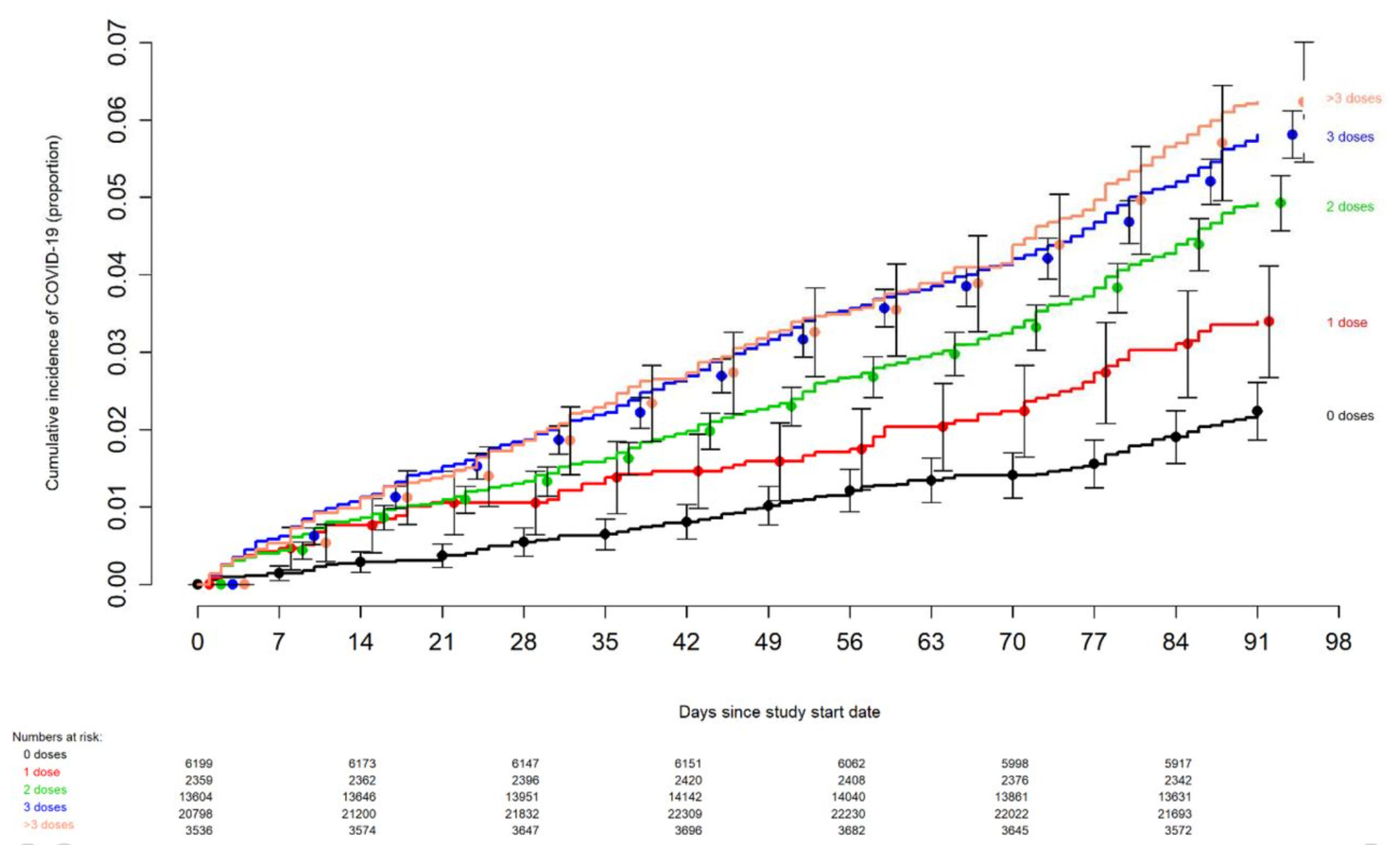
A vaccine making you more likely to get an infected (hence defeating the point of the vaccine) is euphemistically called negative efficacy, and remarkably is never cited as a reason to stop mass vaccinating. For example, the Cleveland clinic study of 46,496 people clearly demonstrated negative efficacy and should have ended the COVID vaccine program immediately (but of course was ignored):
Note: there are other mechanisms besides OAS which may also explain why individuals who got the COVID vaccine keep on getting COVID. For example, another major problem with vaccines (discussed further in this paper on “strain replacement”) is that when they actually work, they rapidly trigger the evolution of variants the vaccine doesn’t cover (e.g., as predicted, countless COVID variants emerged after the vaccine hit the market and before long created the absurd situation where were mandating a vaccine for an extinct virus). This helps to explain why no matter how many people get vaccinated, herd immunity can never be reached, and likewise why the HPV vaccine campaign has led to new strains emerging, and likewise why each successive HPV vaccine (which are often pushed on those who already vaccinated) must cover more and more strains.
In the case of the HPV Vaccine, to get around the negative efficacy issue, rather than acknowledge it or test for an infection before vaccinating, the solution found was to lower the age of vaccination, as it was believed that if girls were vaccinated before being exposed to HPV they could be protected. As a result, the vaccine is now advised to be given to children as young as 9 years of age (despite the youngest girls in the HPV vaccine trials being 11-12 years old).
Sadly, to this day, the FDA and CDC do not recommend prescreening before vaccination. The American College of Obstetricians and Gynecologists, a leading US professional association, goes even further. It recommends that physicians not prescreen patients. In a 2017 opinion, it stated:
Testing for HPV DNA is not recommended before vaccination. Vaccination is recommended even if the patient is tested for HPV DNA and the results are positive. Even if a patient previously has had an abnormal Pap test or history of genital warts, vaccination is still recommended.
Note: ACOG’s 2017 guidelines can be found here, while the current ACOG ones can be found here. As you might guess, ACOG “strongly recommends that pregnant individuals be vaccinated against COVID-19,” and in their guidelines state that vaccination should occur as soon as possible regardless of where they are in their pregnancy and that patients should be repeatedly pressured to vaccinated.
DNA Contamination
Thus far, I’ve argued that the reasons vaccines can make you “become sick” is because they weaken the immune system and make you more susceptible to catching the actual infection or having an already existing infection spiral out of control. While I believe that is the primary issue, there is also another problem—manufacturing vaccines is an inherently dirty process. Because of this contaminated “hot” lots will inevitably get released that sicken or kill many and as I show here, there are many examples of that occurring (a problem which was ultimately “solved” by the government giving legal immunity to the manufacturers).
Many of the newer vaccines are genetically engineered, which in turn requires first creating synthetic DNA (plasmids), then somehow turning that DNA into large amounts of the desired antigen and then finally removing the DNA from the final product so that none of it is there (and can’t infect the recipient). Unfortunately, it’s nearly impossible to get all of it out, so “maximum allowable DNA levels” were created by the drug regulators, and then repeatedly get raised. Worse still:
•That synthetic DNA often contains the SV40 promoter,
a key component of the (cancer causing) SV40 virus which contaminated
the early polio vaccines that likely was responsible for hundreds of
thousands of cancer cases (if not more). This promoter causes genes
it’s nearby to get stuck in an “on” position, which leads to continually
produce proteins making it very helpful for mass producing a desired
antigen but unfortunately also makes cells more likely to turn cancerous (as cancer is uncontrolled growth).
Note: the SV40 promoter also happens to bind to the primary protein cells use to prevent cancer.
•The genetically engineered vaccines all contain adjuvants that coincidentally also happen to excel at bringing foreign DNA into cells (which normally cells prevent from happening). Furthermore, SV40 happens to have another unique property—it causes proteins inside cells to be brought into the nucleus (where they can they become part of genome and create a wide range of permanent harms to the body).
In short, the current technology we use to make vaccines ensures that a certain fraction of it will get into a cell’s nucleus and likely its DNA. This is important to understand because vaccine proponents always argue that there is none of the live pathogen present in the vaccine (unless it’s a live vaccine) so if you “believe” you got the infection from the vaccine, you are misguided and unscientific (e.g., many vaccine “experts” argued this through COVID-19).
For example, many people were afraid the COVID-19 vaccines could change your DNA so countless articles were written which ridiculed that notion without providing evidence to disprove it. This was done by instead repeating a few logical arguments which sounded nice and were deemed to be “true” because the “experts” had espoused them (e.g. consider these frequently cited pronouncements by Paul Offit and Anthony Fauci). Those arguments were as follows:
The vaccines cannot enter the nucleus of the cell
mRNA from the vaccines breaks down rapidly in the cell, so it does not have time to enter the nucleus and change your DNA.
mRNA is not DNA, and hence believing mRNA can change DNA represents a fundamental lack of knowledge of biology.
Yet, it’s now been conclusively proven that the synthetic DNA (plasmids) used to create vaccines was also present in the vaccines and that the COVID vaccines do get into the DNA of cells they transfect. Furthermore, it’s also been shown that the spike protein is drawn to the nucleus of a cell and that the spike protein draws plasmids in its vicinity into the nucleus. In turn, this contamination issue likely explains why many patients continue to produce the spike protein more than a year after vaccination (as its integrated into their genome) and that the higher their levels are, the more likely the vaccines were to injure individuals.
In the case of the HPV vaccine, after it came out, in addition to minor infections becoming much worse, cases also began emerging of girls having HPV DNA in their bodies who had been vaccined but had never had any sexual contact (e.g., I know someone this happened to). While I initially thought this was due to disease provocation and the previously infection having been missed, some of the cases I came across (e.g., one where an 18-year old woman died suddenly) argued strongly against that possibility. Once the HPV vaccines were tested, DNA was found in all them and both the government and Merck reversed their position from “no DNA is in the vaccines” to “the amount there is of no concern.”
One of the most concerning aspects of the SV40 promoter contamination is that the actual virus it came from was known to cause cancer, and after SV40 contaminated polio vaccines were released (despite the governments own scientist warning against the danger of doing so), it triggered a massive spike in cancer that lasted for 40 years. However, sadly as the author of this chart points out, the increase we are seeing now dwarfs the SV40 catastrophe.

Note: the most reliable method we’ve found for addressing what appear to be SV40 related cancers requires signalivng the pleomorphic cycle within the body to normalize (discussed within this article).
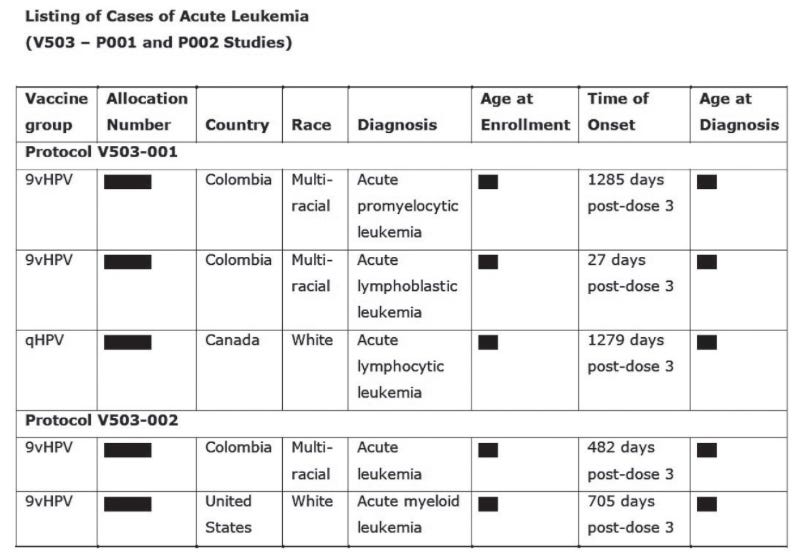
Sadly, with Gardasil 9, in the trials there was also a safety signal the regulators essentially ignored (other than than Europe’s FDA asking for more information in 2014).
Note: it is quite unfortunate a carcinogenic vaccine was able to be marketed to prevent a (fairly rare) cancer.
Safety vs. Efficacy
Much of the medical profession believes that vaccines are “safe and effective,” and that vaccine efficacy is primarily a product of how many antibodies the vaccine can produce inside the body. Since the body often does not want to produce a narrow spectrum of antibodies (e.g., because that leaves it unable to defend against infections that differing from those antibodies or because those antibodies are too similar to human tissue and hence create autoimmunity), this problem is often solved by excessively stimulating an immune response to the target antibody without any concern for the potential harms of doing so (since all vaccines are “safe”).
For example, a major challenge with the COVID vaccines was that the immune system broke the mRNA down too quickly for enough spike protein to be produced to generate a satisfactory antibody response, and likewise, that since the spike protein had a significant overlap with human tissue, it frequently created autoimmunity (especially when it coated the outside of normal tissue—which is exactly what the vaccines caused to happen as that was where the spike protein produced within the cells ended up). To “solve” this problem, the mRNA was modified so the body could not break it down, which resulted in the vaccine effectively creating an antibody response, but simultaneously, many people having mRNA in their body which has continued to produce spike protein for months if not years after vaccination (which has been demonstrated by both clinical testing of vaccine injured patients and research papers evaluating the persistence of the vaccine’s mRNA in living systems).
Note: one of the most surprising facets of this story was Moderna (who was desperate for a successful product so the company did not go under) choosing to use an even higher mRNA dose than Pfizer (3.3x as much)—which resulted in the vaccine being 1.5-3 times as likely to kill the recipient as Pfizer’s (along with being much more likely to cause adverse events and terminate pregnancies). Remarkably however, despite this red flag existing throughout the population level data, no drug regulator recognized it or recommended against using Moderna’s vaccine—which again illustrates how deeply the faith in vaccines always being “safe” is for our regulatory bodies.
The HPV vaccine (which also had a significant overlap with human proteins) faced a similar issue, as it was difficult to reliably generate an immune response to the HPV antigen. This problem was eventually solved by using a stronger aluminum adjuvant (which was never tested for safety but nonetheless was assumed to be safe), and in turn was able to meet the FDA’s criteria of efficacy. Unfortunately, it also led to an unprecedented level of autoimmunity from the vaccines.
For example, in Merck’s trial data, they disclosed to the FDA that 49.6% of vaccine participants developed a “New Medical Condition,” (many of which were likely quite severe), 2.3% of which were categorized as “potentially indicative of a systemic autoimmune disorder.” For reference, this is what is stated in Merck’s package insert for the vaccine, which discussed all the (reported) autoimmune disorders which developed throughout its clinical trials.
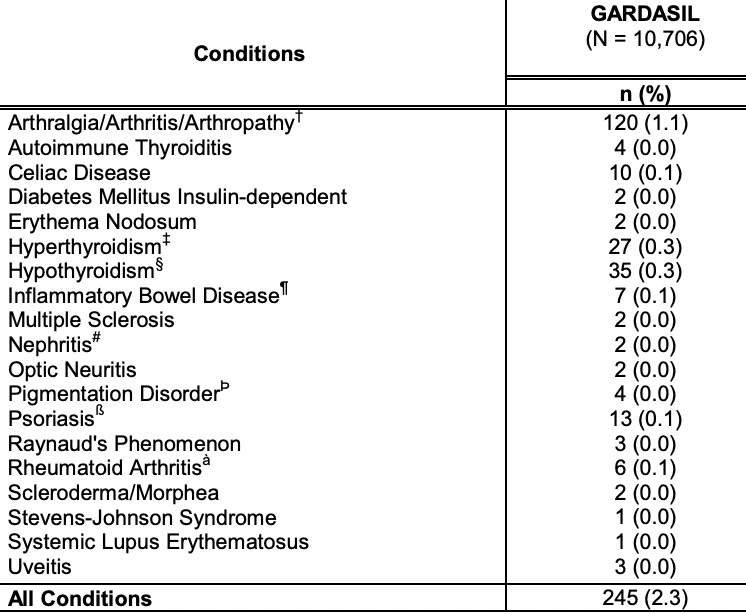
In turn, some of the autoimmune disorders which have been linked to Gardasil since it hit the market include Guillain – Barré syndrome, other demyelinating neuropathies (multiple sclerosis, MS; acute disseminated encephalomyelitis, ADEM; transverse myelitis, TM), postural orthostatic tachycardia syndrome (POTS), systemic lupus erythematosus (SLE), primary ovarian failure (POF), pancreatitis, vasculitis, thrombocytopenic purpura, autoimmune hepatitis and complex regional pain syndrome (a condition which happens to respond quite well to DMSO).
Note: one of key mechanisms of injury behind most vaccines is them collapsing the physiologic zeta potential of the body—causing blood cells to clump together, which in turn triggers microstrokes throughout the body. In turn, the most harmful vaccines that have hit the market were uniquely potent agents for doing this (which in Gardasil’s case came from the novel aluminum adjuvant it used and for COVID-19 was due to the [mass-produced] spike protein’s positive charge density), and in many cases, we find their injuries require restoring the physiologic zeta potential. Likewise, zeta potential disrupting adjuvants (and positively charged lipid nanoparticles) are well-suited for bypassing a cell’s defenses and bringing foreign DNA into them. Additionally, those with hypermobility (e.g., Ehlers-Danlos syndrome) are particularly vulnerable to pharmaceutical injuries (e.g., because their weakened blood vessels can no longer counteract a weakened zeta potential and often also require targeted nutritional supplementation to restore their ligaments and health).
It’s important to emphasize that this is the most important section of the article as this extraordinarily high rate of autoimmunity caused large numbers of Gardasil recipients to become seriously and sometimes permanently disabled from the vaccine. In turn, I could provide pages of heart wrenching stories not that different from the COVID vaccine injuries of how Gardasil ruined many people at the prime of their lives (which would unfortunately make this article too long).
Note: one of the most common side effects of Gardasil (and COVID vaccination) was POTS (a debilitating disorder where severe lightheadedness occurs when standing up which can sometimes trigger fatal car accidents—and which coincidentally were a common cause of death in the Gardasil trials). Many have since concluded this disease was in part an autoimmune disorder as Gardasil victims have been found to have antibodies to the autonomic receptors which are supposed to bring blood to the head (see this article, this case study and this case study), As you might have noticed, POTS never appeared in Merck’s list of reported autoimmune disorders. I will also note that I believe to some degree, POTS appears to be due to an impaired zeta potential (something Gardasil was also notorious for doing), as restoring the physiologic zeta potential often significantly improves POTS.
If
you take a step back, it’s completely unconscionable a vaccine which
provides almost no benefit could be approved while simultaneously giving
at least 2.3% of the recipients a serious lifelong autoimmune illness.
Sadly, we also saw a shocking degree of autoimmunity following COVID vaccination, which likewise was supported by datasets such as:
•An Israeli government study
finding that 24.2% of those receiving a booster developed an
exacerbation of a pre-existing autoimmune condition (along with 26.4% of
those with anxiety or depression having an exacerbation of their
psychiatric condition).
•A rheumatologic database showed
that 37% of patients had an adverse response to COVID vaccination, and
4.4% of those vaccinated experienced an exacerbation of a pre-existing
autoimmune condition.
•A test of inflammatory markers
that predict the risk of an acute coronary syndrome (e.g., a heart
attack) in the next five years in 566 patients found that before vaccination their risk averaged 11%, while afterward, it averaged 25%.
To get around this issue, Merck doctored the trials by having the “placebo” be the vaccine’s damaging adjuvant. To illustrate:
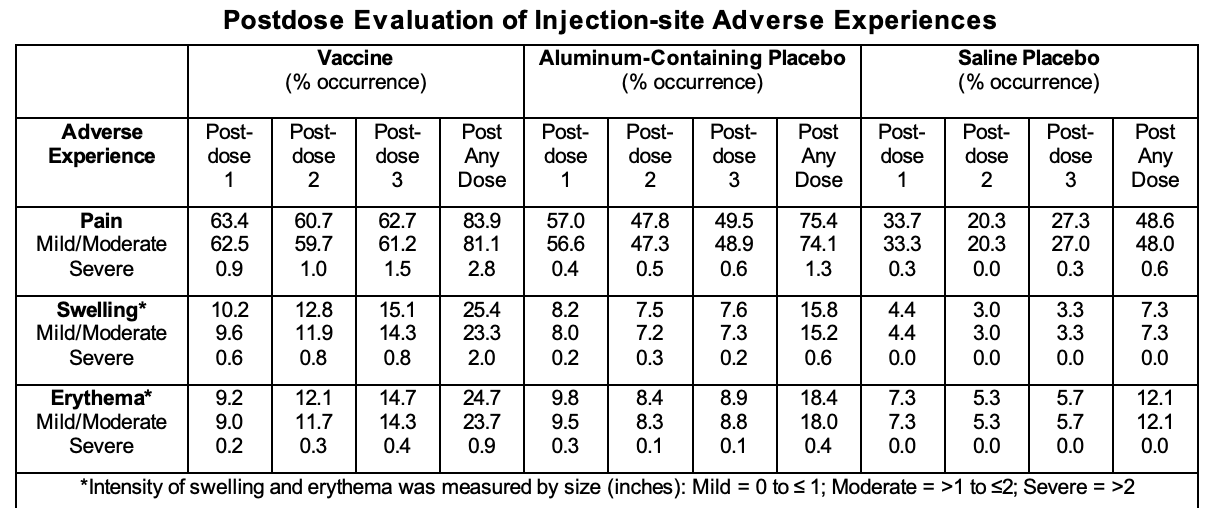
As such, while a massive rate of harm was observed in those who took the vaccine, it wasn’t that much higher than what occurred in the “placebo” group (and thus “by chance”) and like the autoimmune disorders thus was deemed to be “unrelated” to the vaccine.
Infertility
Sadly, autoimmunity wasn’t the only issues. For example, since this vaccine was meant to be given to every woman in the world shortly before they became able to have children, the number one reason to not bring it to market would be if it had a fertility risk. Yet, consider what Merck’s original clinical data showed:
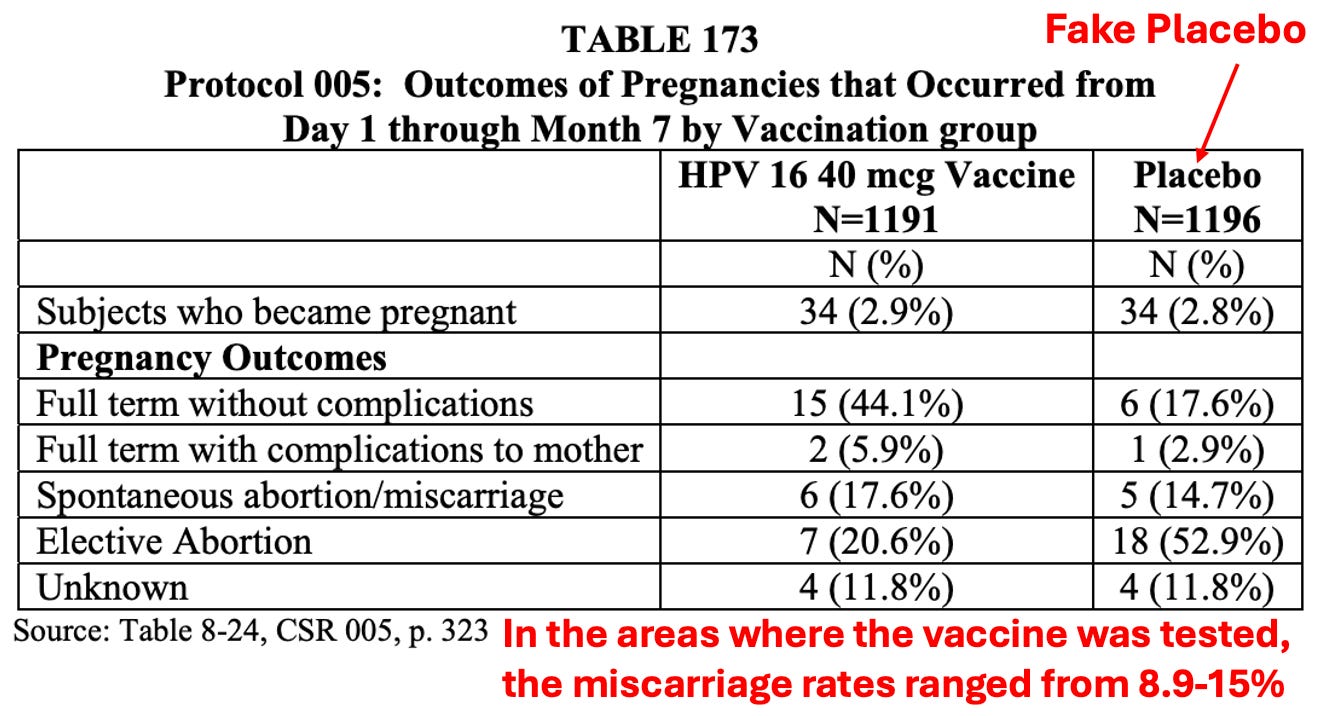
For Gardasil 9 (a newer HPV vaccine with more strains), 17 of the 62 clinical trial pregnancies (27.4%) resulted in a miscarriage.
Note: for Gardasil, the miscarriage rate was even greater if vaccination occurred within 30 days of conception.
In contrast, when GSK’s HPV vaccine was tested (which did not use a fake placebo), a large difference was seen between the two groups.
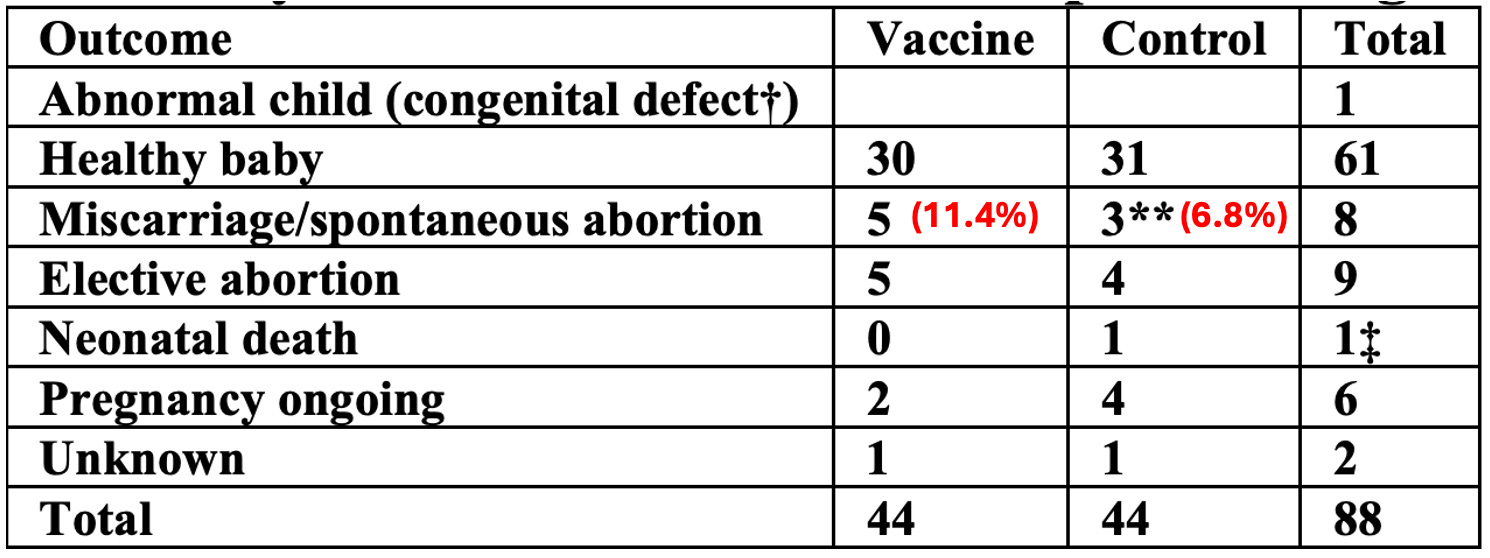
Note: the 6.8% miscarriage rate in GSK’s placebo group is likely representative of what would have been expected in the trials, (especially as the trials were biased towards recruiting healthy young women (who thus were less likely than the average individual to miscarry). For example, this review of the subject finds the average miscarriage rate is around 5.4%. Remarkably, the FDA was far more concerned about GSK’s miscarriage rate (because it was greater than placebo) than they were about the 27.4% rate seen in Merck’s trial—which again illustrates the lack of critical thinking with drug regulators (or a desire to keep this information from being seen by the pro-life community).
Similarly, prior to Gardasil, unexplained premature ovarian failure (POF) was very rare (2 cases were identified by researchers from 1998 to 2008, while 13 were found from 2008 to 2013 following Gardasil’s initial entry to the market). In 2013, a journal presented 3 cases of autoimmunity and POF following HPV vaccine administration, and in 2014, another journal present 3 additional case reports.
Likewise, VAERS (which typically captures less than 1% of the adverse events that occur) tells a similar story. Currently on VAERS (which has been in operation since 1990), 39 cases of POF have been reported, 30 from the HPV vaccine and 9 from the COVID vaccine, while 125 cases of premature menopause (a related condition) have been reported, of which 74 came from an HPV vaccine and 43 from a COVID vaccine (along with 1 anthrax, 1 hepatitis A, 2 meningococcal, 1 TDAP and 3 unknown). However, despite VAERS being designed to recognize specific adverse events associated with vaccines, this was somehow missed.
Let’s now look at what happened once Gardasil was given to our next generation:
Note: in 2020 it was estimated 77.1% of girls between 13 and 17 years of age had received this vaccine, while in England roughly 90% of girls had received the vaccine.
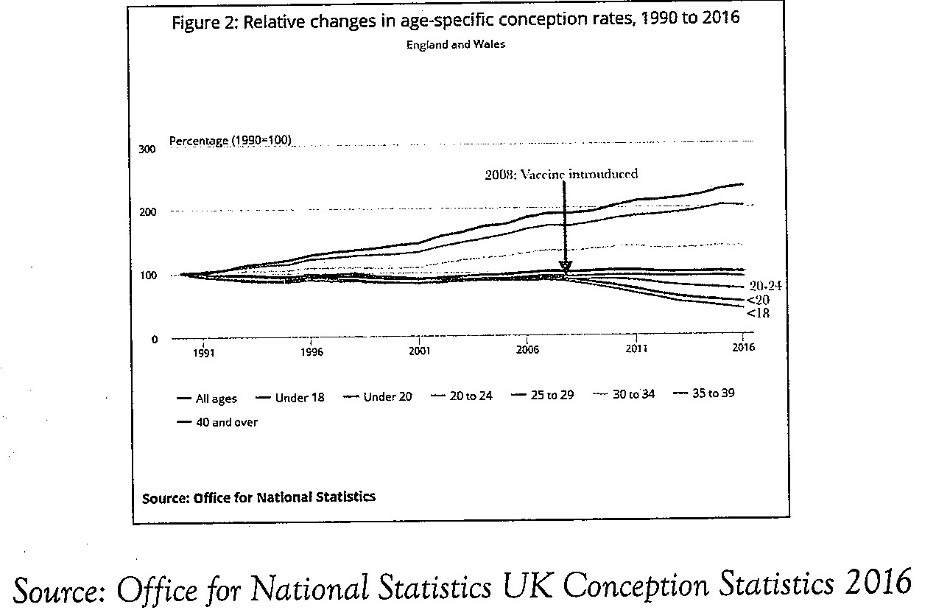
To
clarify this chart: an overall decline of 44% was observed for girls
under 18, most of whom lived in England. The rate in decline was the
greatest in those under 16. For example, in neighboring Scotland, also a
part of the United Kingdom the teen pregnancy rate declined 60% from
2007 to 2015.
Typically, it is very difficult
to draw causation between two events because so many other variables are
also present. While fertility in all age ranges was affected by
Gardasil, this dataset is remarkable for how clearly it is able to show
this correlation. This profound drop in teenage fertility was originally
acknowledged and met with alarm. Because no cause could be identified,
it was then forgotten and the trend has continued ever since (with the
exception of individuals like Elon Musk saying declining fertility rates
pose an existential risk to the United States).
Note: for Gardasil, the miscarriage rate was even greater if vaccination occurred within 30 days of conception and likewise when the first Gardasil vaccine was tested, the FDA noticed there were 5 birth defects (compared to 0 in the “placebo” group) when the vaccine was given within 30 days of conception—but the FDA nonetheless did not put a warning for this on the label.
Similarly, with the COVID vaccines, from the start, one of the major concerns with them was that they were never adequately tested for this safety during pregnancy despite numerous reasons they could be dangerous during pregnancy. Then, as more and more red flags they posed a fertility risk emerged (e.g., in VAERS and V-Safe), the medical system decided to push the vaccine on pregnant women while claiming it was safe and simultaneously refusing to release the actual V-safe data (which through a FOIA ICAN litigated we were later able to show was being fraudulently presented to the public to massively downplay the dangers of the vaccines it detected).
Note: Igor Chudov showed Moderna’s higher (and hence more toxic) mRNA dose posed a much greater pregnancy risk (e.g., it caused 42% more miscarriages and 0.09793% of infants born to a Pfizer mother died whereas 0.18948% from a Moderna mother died). Likewise compared to Pfizer, Moderna caused 3.7 times as many birth defects, 1.48 as many NICU admissions and a massive increase in preterm births [(0/42 vs. 4/34]).
Since the vaccine hit the market:
•Menstrual issues have been observed in roughly half of the female COVID-19 vaccine recipients.
•Numerous OBGYNs (e.g., James Thorpe, Kimberly Bliss)
have tried to sound the alarm on this problem. Likewise, we’ve seen
numerous vaccinated patients who simply cannot get pregnant.
•Many reports have come out about this problem (e.g., this one
highlighted that the COVID vaccine caused the miscarriage rate to jump
from 28% to 40% at one of Utah’s largest fertility clinic and contained
many stories of miscarriages, death, disability, and a wide range of
other adverse events).
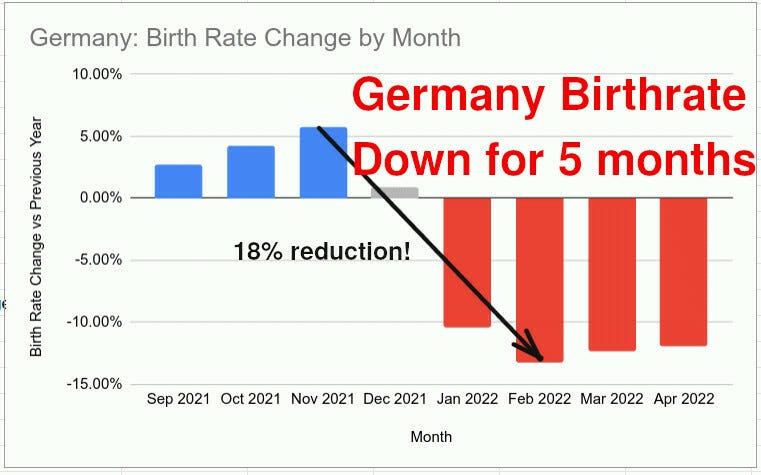
•The have been massive drops in the birthrate since the COVID vaccines hit the market (in the range of 8-16%), which is massive and could not have happened by chance (e.g., see this report and this report).
Likewise, consider this recent headline:
SINGAPORE: For the first time ever, Singapore’s resident total fertility rate has dropped below 1.0. Preliminary estimates show that the total fertility rate fell to 0.97 in 2023, declining further from the previous record of 1.04 in 2022 and 1.12 in 2021.
Note: a total fertility rate below 2.1 will cause a population to drop because there are more deaths than births.
Deaths
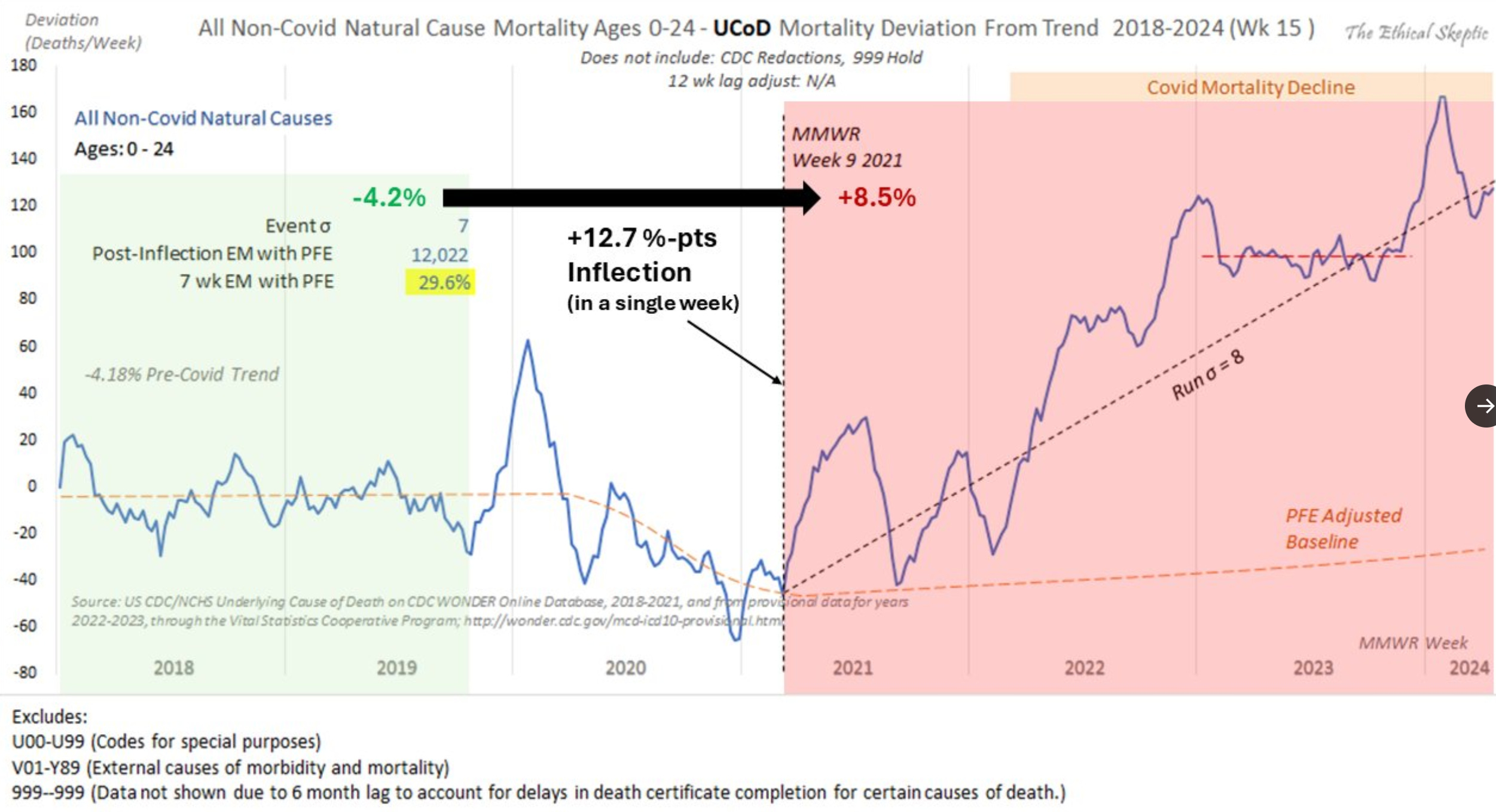
Much attention has been brought to the explosion of “unexplained” (and often sudden) deaths which occurred after the COVID vaccines hit the market in the youngest and the healthiest members of society:
However, significantly less attention has been given to the fact in the initial Gardasil trials, out of 21,458 10 vaccine recipients and 7 “placebo” recipients died including 7 from car accidents
(which can be triggered by POTS causing drivers to pass out). However
despite the Gardasil death rate (8.5 per 10,000) being almost twice the
background death rate in girls and young women (4.37), the FDA was not
concerned.
Note: the actual death rate was likely lower since young and healthy girls were selected for the trials.
Risk vs. Benefit
If you take a step back, this is quite extraordinary—if we make the absolute best case scenario about Gardasil (that every drop in cervical cancer deaths) was due to it (and not an existing trend), in England, it saved 0.6 lives per 10,000 injected and 0.2 per 10,000 in the USA.
Conversely,
it killed at least 4.13 per 10,000 who were injected (who unlike those
who typically die past the age of 50, these individuals were at the
start of their lives). Furthermore, it gave at least 230 a significant
autoimmune disorder, and had a significant impact on their fertility.
Finally, many suffered a wide range of more subtle complications from
the vaccines.
Putting it mildly, that is a terrible
risk vs. benefit ratio. Sadly, I’ve come to the conclusion many things
in modern medicine ultimately are sales funnels design to hook people
into more and more costly medical services (at the expense of their
health). In turn, one I’ve tried to bring awareness to was recently
discussed by Tucker Carlson and Elon Musk (which shows how much
awareness of the subject is spreading):
Note: the dangers of SSRIs are discussed further here, and their link to mass shootings (and other forms of psychotic violence) here.

In this sales funnel, one point I highlighted is that Gardasil’s frequent neurological damage also causes psychiatric instability which in turn results in young women being moved down the sales funnel—something I have directly observed happen multiple times. However, in almost all cases, that outcome will never be linked to Gardasil. Likewise, I have numerous patients who developed lifelong autoimmune disorders shortly after the vaccine, but beyond none of their doctors believing their assertion the two were linked, most patients don’t even draw the connection until I point it out in their history.
All of this in turn touches upon two critical points:
•In
many cases for a vaccine, their risks clearly outweigh their benefits
(e.g., I published an attempt to objectively compare the risks and
benefits of each childhood vaccine here—out
of which I believe HPV has one of the worst balances between the two).
Yet, no matter how absurd the ratio is (e.g., children are not at risk
of getting COVID and the vaccine does not prevent transmission, so there
is no conceivable argument to ethically justify giving these risky
products to them), the medical community still, in lockstep, recommends
them.
•If Gardasil had such a high injury rate, it should have been detected in the trials (which as I showed it to some extent was) and not approved by the regulators.
As you might guess, what actually happened has numerous remarkable parallels to COVID-19.
Gardasil’s Clinical Trials
In a previous article on Gardasil’s clinical trials, I argued they had many parallels to an abusive relationship as in both:
•The
abuser will initially say you are the most wonderful person imaginable
for coming to them and give you numerous lavish promises to entice you
into their trap.
•Once they have you ensnared, begin to go back on every promise and continually gaslight
you as they hurt you (e.g., beyond denying your injuries, they will
never allow them to enter the trial record regardless of how much the
participants try).
•Then once you have nothing to offer them, they will discard you and leave you on your own to pick up the mess.
Sadly, this type of abuse in research has become so normalized, that by the time COVID-19 came around, not only did it happen again, but the government actually sided with the abuser.
Here for example are two stories of Gardasil clinical trial participants that have a remarkable number of parallels to what the COVID-19 vaccine trial participants went through:
When she was eighteen and still in high school, Kesia received a brochure in the mail about an exciting clinical trial for a vaccine that would prevent cervical cancer. She didn’t know it was possible to vaccinate against cancer. She had heard that getting regular Pap tests was the best way to prevent cancer because most problems could be caught early and treated. The brochure said that the vaccine had no side effects, as it had already been thoroughly tested. It read, “FUTURE 2 er IKKE et bivirkningsstudie,” which translates to “the FUTURE 2 study is NOT a side effect study” (original emphasis on “NOT”). This piqued her interest, particularly because the vaccine had already been proven safe….
…At her [third vaccination] appointment, she told the clinician she wasn’t feeling well and was frequently tired and in pain. She asked if she should perhaps delay the shot. The nurse reassured her that what she was feeling had nothing to do with the vaccine and that she could get the third dose without problem. The nurse asked if Kesia had had any reactions after her second dose. Outside of the headaches, the fatigue, and muscle aches from her ongoing illness, Kesia couldn’t remember the exact details from the last six months. She told the nurse about the headaches, which she got four or five times a week, lasting all day. The nurse told her not to worry and that some headaches were normal.
She completed the paperwork and gave Kesia her third and final injection…After this appointment, Kesia felt dizzy for the first time. She felt nauseated, and her arm hurt more than ever. During the following weeks, however, her health took a sharp turn for the worse.
She went to her doctor, and when she told him she had participated in a clinical trial for a new vaccine, he was worried. He made a note in her file, and Kesia saw him put two exclamation points next to it. He asked her to talk to the trial staff again about her symptoms because all her blood tests were fine [common blood tests typically cannot detect signs of vaccine injuries which leads to the patients being told nothing is wrong and it is all in their head].
Kesia returned to the hospital for a follow-up visit a month after her final shot. She tried to talk to the trial staff again about her symptoms based on her doctor’s concerns [sadly this is often the only way to get people to listen], and they listened more intently this time. She told them that she was struggling to keep a normal, everyday life and that this was not something she had ever experienced before. But they told her once again that her symptoms were not the kind they would expect to see with the vaccine, and she should continue to see her regular doctor.
Kesia accepted this explanation; after all, they were the experts, and she knew the vaccine had already been tested for safety. She tried to put it out of her mind (“I DIDN’T WANT IT TO BE THE VACCINE”), as she had a 50 percent chance she’d received the saline placebo and not the vaccine at all.
As [the] months passed, Kesia became so ill that all she could think about was her next doctor’s appointment. She missed so many exams in her last year of high school that she couldn’t graduate alongside her classmates. She had to put her dreams and plans “on hold until she could feel well enough to get through the day without a headache or pain in her joints and muscles. It was a daily struggle to get out of bed, let alone to attend school or university…She never thought months would turn into years, and years would turn into more than a decade [I also know people who have experienced things like this].
When the trial investigators unblinded the trial in 2007, a year after the FDA approved Gardasil, Kesia learned that she had received the vaccine after all. She was relieved that the trial was over. If she had had the saline injection, she would have been strongly urged to go back to the hospital for the three vaccines, which would have been tough now that she was so ill [this an excellent illustration of the cult-like mentality around vaccines, which only see their benefits but not their harms]. She heard no more from the clinical trial staff, although she agreed to be part of follow-up studies.”
More than a year later, when she was sitting with her husband, watching an online news channel, things clicked. She heard a woman talk about getting the vaccine shortly after it was approved. As the woman described her reaction to each shot, Kesia’s heart stopped. It was like listening to her own story—the same timeline, the same symptoms. At that moment, Kesia felt like the rug had been pulled out from under her. After all these years of wondering why she was so sick, here was another woman telling the exact same story.
She couldn’t believe it. How could this happen if the vaccine had been “proven” safe? Every time she told the trial nurse about her symptoms, the nurse assured her that they weren’t related…She barely slept that night.
The next day, she went online to start looking for answers [although Facebook aggressively censors pharmaceutical injury support groups, they are much more common now than they were in the past and I’ve learned a great deal from them]. She contacted Denmark’s vaccine victim support group and spoke with Sara, who eventually became her dear friend. They talked for a long time, and Sara understood. She had heard it before. For Kesia, though, it was the first time she didn’t feel crazy. It had been thirteen years of living with pain and hearing doctors deny that her condition was real [this is what you hear over and over again in those previously mentioned support groups].
In April 2016, she finally sat down with her husband to watch The Vaccinated Girls. She wasn’t quite prepared to see Danish teenagers suffering from precisely what she had been living through for more than a decade. She cried for what she had suffered, but even more for what was happening to all the other girls since the clinical trials. If clinicians in the trials denied any connection between her symptoms and the vaccine, it made sense that doctors today continue to deny them.
Only a few miles away in Copenhagen, another young woman was going through a similar awakening. Sesilje had also been in the FUTURE 2 study, and like Kesia, her health too has suffered ever since. The two young women met through the victim support group in July 2016. Sesilje’s story is remarkably similar to Kesia’s, with one significant difference: Sesilje received the placebo…
…Sesilje didn’t notice any strong reactions after the first shot, although it was quite painful. She had an unusual menstrual period the month following the vaccine but did not think it was related. The clinicians did not give her any booklet or form for recording symptoms. They did mention that she would feel injection site reactions and maybe a headache. The bleeding was just a coincidence, she thought.
A month later, Sesilje went back to the hospital for her second shot…[The clinicians] told her that she should see her personal doctor about the menstrual period, as it was unrelated. “It was after this shot that she noticed unusual symptoms, not just the heavy menstrual period. Her skin hurt, she had headaches, and she felt as if she had the flu. Her stomach really hurt, and she lost twelve pounds in a matter of weeks. She went to her doctor, but he could not figure out her symptoms. Sesilje couldn’t understand; she had always been healthy [this is also a very common story].
When Sesilje returned for her third shot, the trial staff told her again that her recent health issues were unrelated. She should continue to see her own doctors and follow their advice. They assured her it was safe to proceed.
[After] finishing the series in 2003, Sesilje was told she had to wait until 2007 to find out if she had received the saline placebo or the vaccine. Her symptoms persisted, but no doctor could figure out why. She developed an allergy to her deodorant and various skin creams. She went to a dermatologist, who told her to switch brands, which didn’t help. As part of her studies in medical research, Sesilje was around healthcare professionals, but no one could explain why she was so ill. Like Kesia, she learned to cope [and suffered significant symptoms in the years that followed, especially after being pressured to and receiving the actual vaccine]…
…In 2015, everything changed. She read online that the Gardasil clinical trials had used an aluminum solution as the control, not saline, as she had been told. Sesilje worked in clinical research, so she knew that this should not have been permissible. She was certain that she had been told that the control was saline—it was even printed in the brochure she received years ago.
She was determined to research this, if only to prove the online information wrong. She expected to confirm that the placebo was “saltvand”—Danish for “saline.” Instead, she found that there was no saline placebo group at all. What she had read online was correct: the control contained aluminum. Her heart sank. She knew what this meant: because the vaccine also had the same solution as the control, [she had] received [a total of] six injections containing aluminum, three as the “placebo” and later three as the vaccine.
The protocol said that safety testing was the clinical trial’s number one objective. Yet Merck had assured potential trial volunteers in the brochure they’d received that the control was saline and that FUTURE 2 was not a “side effect trial,” because the vaccine had already been proven safe [as all vaccines are “safe”]. Was this why their side effects were not taken seriously, because even the trial administrators didn’t know exactly what they were injecting into participants? The clinicians did not collect any medical records from Kesia’s or Sesilje’s doctors and didn’t record any details to explain why they thought the symptoms were unrelated. The reason Kesia and Sesilje felt safe enlisting in the trial was that [they were told] Gardasil had been proven safe.
Note: in a previous article, I detailed many of the approaches Merck used to hide the injuries participants received (e.g., they made it impossible for trial participants to report most of their injuries, gave trial investigators the discretion to label injuries as “unrelated to the vaccine,” and then dismissed all the ones that nonetheless got through those two filters as still being unrelated to the vaccine).
In addition to their immense suffering, this story highlights a few critical points.
First, clinical trials are supposed to identify potential risks of a new product. In turn, if at least 2 girls in the tiny (relatively speaking) trials had those type of injuries, it means far more were affected when the vaccine hit the market.
Second, rather than this being a placebo effect, these girls had a strong psychological investment in believing the vaccine was not the source of their injury. This is a very important point that often gets glossed over (e.g., parents who acknowledge vaccines hurt their children wrestle with an immense amount of guilt for their decision to vaccinate—and hence often simply refuse to consider the harm occurred) as one of the most common arguments used to discredit those parents is either that they lack the capacity to recognize they are being conned by misinformation or that they have unscrupulous motives to blame the vaccine (e.g., a bias against vaccines or a desire for money).
Third, their experience (and the fact neither FDA or EMA ever did anything about it) was what helped me to predict how the COVID-19 vaccine trials would like play out (and was why I joined numerous private groups for vaccine trial participants as I knew that would be the best way to get an accurate picture on how dangerous the vaccine actually was since I felt it was inevitable most of their injuries would never be reported).
Fourth, their experiences (and the concerning clinical trial data I’ve detailed throughout this article) should have been red flags to the drug regulators. However, rather than recognize them, they accepted every excuse Merck provided and declared the vaccines to be “safe and effective.”
Finally, this helps to illustrate why in the current regulatory environment it is unwise to enroll in a clinical trial as there is no recourse for being injured (as regardless of how the participant tries to have it be reported) as all the existing incentives are for vaccines companies to downplay the injuries to their product so they can declare the vaccine “safe and effective.” In turn, this is exactly what happened in the (unblinded) COVID vaccine trials (e.g., numerous whistleblowers showed that the FDA in collaboration with the pharmaceutical companies buried their crippling injuries and unblinded the trials so they could disproportionately count COVID cases in the unvaccinated individuals to create the illusion of efficacy).
Regulatory Response
The Director for the FDA’s Center for Biologics Evaluation and Research, Dr. Jesse Goodman, called Gardasil a “huge advance,” and added that the vaccine deserved a speedy review process because “ . . . its rapid approval underscores FDA’s commitment to help make safe and effective vaccines available as quickly as possible.”
Due to how toxic Gardasil was, once it hit the market, the FDA and CDC were deluged with a wave of reports of adverse reactions to it. However, rather than acknowledge them, they doubled down on their protection of the vaccine and concocted an increasing elaborate series of steps to protect the vaccine.
Note: this sadly is how I was able to predict they’d do the exact same thing with the COVID vaccines even now that their harm has become so widespread the majority of America believes they are killing people and there being no possible justification to keep on pushing the vaccine (e.g., the original strain it “protects you against” is extinct, the endless boosters make you more likely to get COVID, and now only a small portion of the population is even choosing to get them).
For example, in 2009, in response to widespread publicity detailing severe adverse events attributed to the Human Papillomavirus (HPV) vaccine, the FDA and CDC initiated a study to examine Gardasil's safety profile based on VAERS case reports. It analyzed all VAERS reports filed since Gardasil's mid-2006 approval through the end of 2008, a period of two and a half years.
The study found that "the VAERS reporting rate for [Gardasil] is triple the rate for all other vaccines combined." Additionally, the study found that 68% of the reports were submitted by representatives of Merck, Gardasil's manufacturer, most of which needed to be completed or more accurate, and 90% of which required more information essential for conducting medical assessments. Finally, the authors also noted that VAERS suffered from underreporting.
Despite that red flag and a clear indication that, if anything, it was underestimating the scale of the issue, the authors just dismissed it. Instead, they declared that the high rate of adverse events "reflects greater public attention to HPV," which was purportedly "stimulated" by "widespread media coverage" and that Gardasil's "post-licensure safety profile" as calculated from VAERS data is "broadly consistent" with safety data collected in its clinical trials, while simultaneously failing to support these assertions. Not surprisingly, following the study's publication, news organizations and health authorities such as the CDC and WHO repeatedly referenced it as proof that Gardasil was safe.
Note: citing a doctored study you funded to advance your agenda is a very common tactic in the medical industry.
Similarly in Europe:
Concern has been raised about whether HPV vaccines might cause serious neurological disorders including postural orthostatic tachycardia syndrome (POTS) and chronic regional pain syndrome (CRPS). The European Medicines Agency (EMA) investigated the issue and declared in 2015 that there is no link between HPV vaccines and serious neurological adverse events. However, the certainty conveyed in EMA’s official report is undermined by a leaked, confidential document that reveals important disagreements among the experts.
Furthermore, in its assessments, EMA relied on the data the drug companies had provided to them [and then in 2015 asked them to re-evaluate for the EMA] even though it had been demonstrated that the companies had underreported possible neurological harms. Even though active comparators were used (aluminium adjuvants and other vaccines), our research group found significantly more serious neurological harms in the HPV vaccine groups than in the comparator groups in a systematic review based on clinical study reports in EMA’s possession.
Since the regulators would not address this catastrophe, others had to speak up. For example, Peter Gøtzsche, considered to be one of the world’s experts on data integrity and pharmaceutical fraud, spoke out about what was happening, after which he was immediately expelled from the Cochrane Collaboration (most likely due to the fact the previously “independent” Collaboration had recently started taking money from the Gates Foundation—one of the leading proponents of and investors in the HPV vaccine—who recently invested over 600 million dollars to vaccinate 86 million girls in low- and middle-income countries by 2025).
Note: since the events in 2018, the world-renowned work from the Cochrane Collaboration has greatly lost its objectivity (e.g., they published a high leading misleading review on the use of ivermectin for COVID-19 which played a pivotal role in many governments to abandoning its use).
Simultaneously (especially after Obama effectively caused the Democratic party to partner with the pharmaceutical industry) there was very little effort by the liberal groups who traditionally defend civil liberties to advocate for the Gardasil girls. Instead the conservative non-profit watchdog group Judicial Watch (which to my knowledge had not previously focused on medical issues) in 2007 began a campaign to hold the FDA accountable for what they’d done with Gardasil.
From their 2007 FOIAs Judicial Watch learned (in addition to the points mentioned throughout this article) that:
•At Merck’s May 18, 2006, meeting with the Vaccines and Related
Biological Products Advisory Committee, despite numerous issues being
raised, the vaccine received a unanimous vote of approval (which was the
case for many of the COVID vaccines). Likewise, at that meeting, it
opened by Merck’s representative stating “Merck proposed that studying
cancer itself isn't feasible, because it takes too long and it
disadvantages too many women” (not unlike the long term effects of a
gene therapy not being important enough to study before giving it to
everyone).
•Despite marketing Gardasil as a vaccine
that prevents cancer, Merck never tested it for the potential to cause
carcinogenicity or genotoxicity (which was also the case for the
COVID-19 vaccine). Likewise, at the time of its unanimous approval (for
“preventing cancer”), it was not known if it would actually prevent
cancer or how long it’s protection would last for.
•Despite it’s immense cost, it’s longterm effectiveness was not known (and similarly, the COVID vaccines were initially marketed as an end to the pandemic had their effectiveness rapidly wane and “required” continual boosters).
•Gardasil received an accelerated (rushed) review because it “had the potential to fill an unmet medical need” (which likewise happened with the COVID vaccines).
•The FDA was fully aware (and somewhat concerned about) the vaccine’s negative efficacy for those who were already infected and likewise concerned about Gardasil’s impact on pregnancy (which, like the COVID vaccines, Merck only studied in rats). Nonetheless, at the time of approval (for all women of child bearing age) they weren’t sure if it was safe in pregnancy (again not unlike the COVID vaccines).
•Additionally, in the trials, 6 breast feeding infants had an acute respiratory illness within 30 days of mothers who got the vaccine, whereas this only happened to two breast feeding infants of mothers who got the vaccine (and likewise numerous reports have emerged of infants becoming severely ill after breast feeding from a recently vaccinated mother).
•8,864 VAERS reports had already been received for Gardasil (e.g., 38 reports of the “one in a million” Guillain-Barre Syndrome, most of which occurred immediately after the vaccine—but nonetheless were deemed to be unrelated to the vaccine by the FDA). Many of those reactions happened when it was given with the meningococcal vaccine that most commonly were fainting (that sometimes lead to severe injuries), nausea, and dizziness but also inculded girls suffered from pyrexia, convulsions, seizures, spontaneous abortions, and Guillain-Barre Syndrome. Nonetheless Gardasil (like COVID-19) was never evaluated for if it could be given concurrently with other vaccines.
•Eighteen deaths of young girls and women were reported to VAERS (e.g., a healthy 17 year old dying suddenly two days after her third dose, another 19 year being found dead in bed without any known cause and another dying of myocarditis). Frequently, blood clotting was mentioned as a potential cause but the FDA never investigated if there was a potential contraindication between taking birth control (which causes blood clotting but not sudden death and was also mentioned in the reports) and the vaccine. Finally all but one of these deaths occurred within 3 weeks of getting the vaccine.
Then from their 2013 FOIAs (which the FDA, like now, also fought) Judicial Watch learned:
•$5,877,710 had paid out to 47 people injured and 2 killed by the HPV vaccine (at the national no fault vaccine injury program), while 92 claims were still pending (5 of which were for deaths) and 59 (including 2 deaths) were rejected by the program.
Fortunately, attention was finally brought to this catastrophe (although sadly not in the United States). This TV program for example was aired in Denmark in March 2015:
To further underscore the parallels to COVID-19, I’ll end this section with a quote from Judicial Watch’s 2007 report:
While Dr. Harper said she believes that the vaccine will be beneficial in the long run, she cautions: “To put in process a place that says you must have this vaccine means that you must be part of a big public experiment and so we can’t do that. We can’t have that until we have more data.” It is unacceptable to mandate any vaccine without first testing it for effectiveness, safety, and long-term side effects. The Gardasil vaccine may be an important step in preventing cervical cancer, but it is a step that may cause other harms.
Conclusion
Typically, when a predatory industry wishes to do something unconscionable, it will begin by doing it on a smaller scale to a group that doesn’t quite have the ability to fight back, and then once it get normalized and can no longer be opposed, do it on a much broader scale. For example, all the horrific playbook Fauci enacted upon America during COVID-19 was almost identical to what he got away with doing to the gay community during AIDS and it is my view that if America had spoken out against what was being done to them, COVID-19 would have never happened.
Similarly, after Gardasil was approved in 2006, four countries (India, Uganda, Peru, and Vietnam) were chosen to as mass test sites for HPV vaccines
so these lucrative products could be added to the national immunization
programs. In India, those trials (which were funded by Gates, Merck and
GSK and conducted in areas which had no way to ever accurately monitor
cervical cancer rates) resulted in 7 deaths between 2009-2010, and
a subsequent governmental investigation discovered human rights abuses
and systematic failures in the oversight of those trials that had resulted from widespread corruption with India’s drug regulators.
For
example, many of the girls in the “trials” had never consented to
entering the trials (rather school officials “consented” for them), and
at the time were told the vaccine would protect them from all cancers
and was completely safe. Many children were injured and many with clear
contraindications to the vaccine nonetheless received the vaccine.
Ultimately, they concluded
the US governmental program (PATH) which spearheaded those trials “
“has exploited with impunity the loopholes in our system” and “has
violated all laws and regulations laid down for clinical trials by the
Government.” It hence should come as no surprise factions within the
government were willing to conduct the experimental COVID-19 campaign and continue to violate every ethical safeguard as casualties continued to mount.
Note: the last two links are a direct download for a word document .
Sadly, the Gardasil debacle was not the only test run for what we saw with the COVID vaccines and in this publication I’ve tried to expose some of the other forgotten vaccine disasters. For instance, the widely opposed childhood vaccine mandates pushed across America after the California measles outbreak in 2015-2016, were the test run for the COVID-19 mandates. Likewise, the disastrous anthrax vaccine mandates upon America’s military (which ended up being so devastating to the military laws were eventually passed to make mandating experimental vaccines on our soldiers illegal) ultimately were a beta-test for the horrific acts committed on our soldiers with the COVID vaccines.
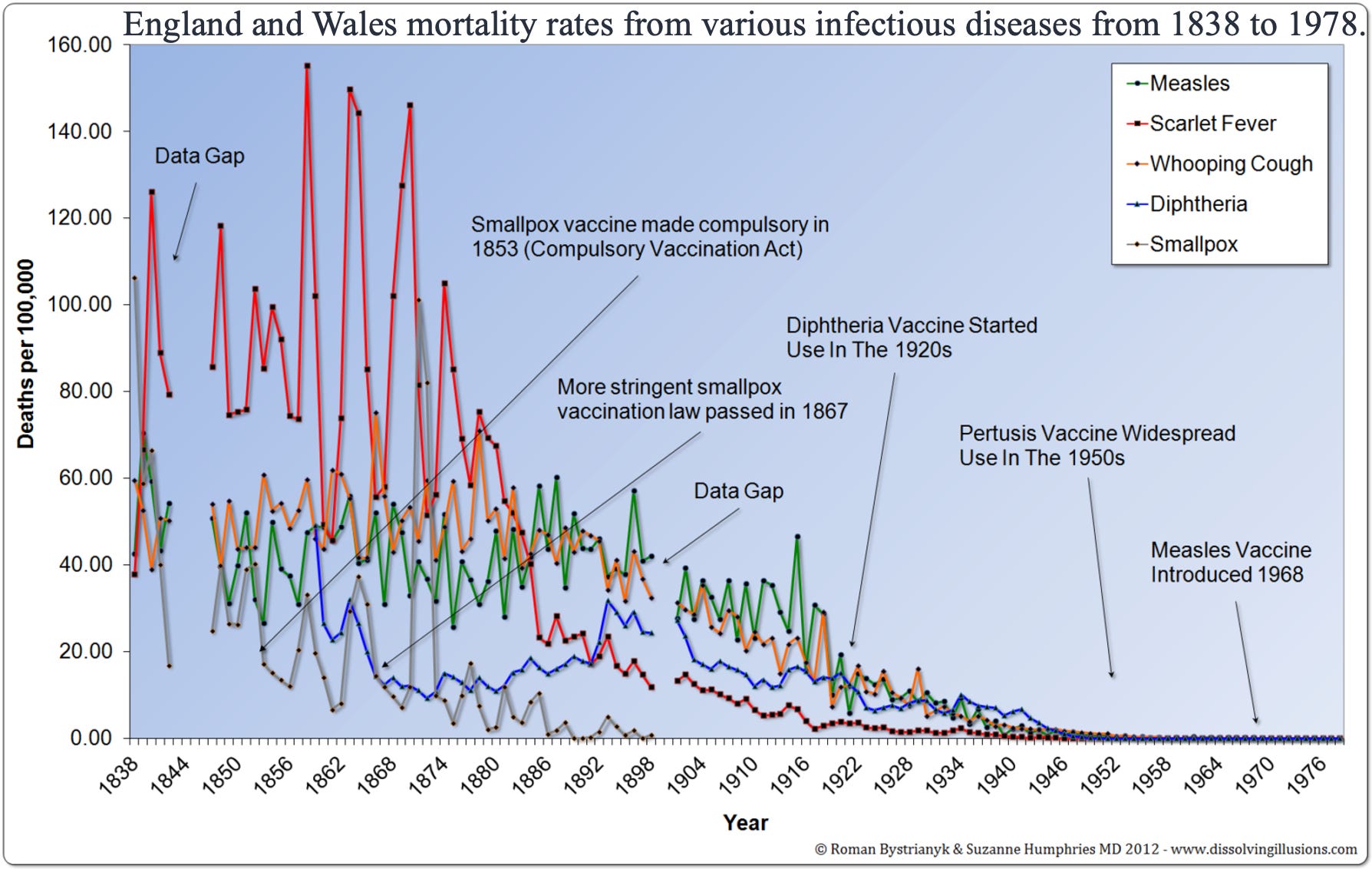
More remarkably however, you can trace all these parallels back to the earliest vaccines. For example, in the case of the smallpox vaccines, beyond being untested and some of the most dangerous vaccines in history, the disease provocation they triggered would consistently cause smallpox outbreaks—which governments responded to by demanding even stricter mandates. Eventually, this led to widespread public protest and a city’s government being replaced with one that overturned the mandates—which the medical profession predicted would cause a catastrophic smallpox outbreak, but instead resulted in the city overcoming smallpox and creating a model (e.g., quarantining contacts) which the rest of the world copied that eventually eliminated smallpox.
At this point, we are in a unique moment in history. On one hand, the insatiable greed of the pharmaceutical industry has been allowed to go so far things we previously could have never imagined would happen are now business as usual. On the other, a historically unprecedented moment has arisen and much like what we saw during the end of the smallpox mandates, much of the public now supports overturning this insanity (e.g., there is broad support for Making America Healthy Again).
Having watched the pharmaceutical industry’s abhorrent actions play out for decades, I had long resigned myself to its momentum being unstoppable—yet now I can see an unprecedented opportunity exists to change things in the near future. That hope is a large part of what drives me to work so hard on this, and likewise, I am profoundly grateful both to all of you for enabling me to do it and because everything each of you has done has been what’s made the opportunity we have now possible.
Lastly, for anyone wishing to know more about the HPV vaccine debacle, it is detailed with Mary Holland’s aptly titled book: The HPV Vaccine on Trial: Seeking Justice for a Generation Betrayed.
To learn how other readers have benefitted from this publication and the community it has created, their feedback can be viewed here. Additionally, an index of all the articles published in the Forgotten Side of Medicine can be viewed here.
No comments:
Post a Comment