This article has morphed into something entirely different from the original idea I had yesterday when I started writing it. As it stands, it appears as though COVID-19 deaths might not be COVID-19 deaths at all.
Many thanks to Clare Craig, Norman Fenton, Martin Neil, Joel Smalley, Scott McLachlan, Jonathan Engler and Ben Lewis for your helpful feedback.
I am going to try to pay homage to what I spent 2 days rewriting and also to what the take home message is. I can only hope I did a decent job explaining my own confusion.
I found a website today (yesterday) that I like because it has maps and numbers. My favorite things. It’s called USA Health Rankings: Live Longer Live Better and you can find it here. Their data is sourced from many places.¹
There are many interesting things to see in their data compilation and it’s really nice how they do state-by-state comparisons in their rate assessments for top causes of death in the United States. For the purposes of this article, I would like to focus on COVID-19 as a cause of death. It became the #1 cause of death shortly before the roll-out of the COVID-19 injections into the United States, and has remained #1 until recently, bumped out by Coronary Heart Disease (CHD).
If you like watching numbers change, click ‘play’ on their COVID-19 death simulator. You will be able to watch COVID-19 go to #1 on December 28, 2020 and revert to #2 on February 15, 2023. Keep in mind that due to the 2-month head start that CHD had (the clock started for the other causes on January 1, 2020), it actually overtook CHD on November 12, 2020 and fell back to the #2 position on May 6, 2023. How do you spell Adverse Event again?
But wait now, before we take these rates to the bank: What is a COVID-19 death?
On COVID-19 deaths
Before I go any further, I want to try to define more clearly (at least for myself) what a COVID-19 death is. I have never placed much value on either COVID-19 ‘cases’, or ‘deaths’, because in the former, a ‘case’ relies on 2 things:
PCR with cts high enough (45!) to catch any DNA (and it’s not just about cts) - sometimes being done with a single set of primers
A specific list of symptoms, which quite frankly, suit many illnesses including pneumonia.
In the latter, a COVID-19 death relies on death certificates which have been reported to have the cause of death mis-attributed to COVID-19, when the cause of death was clearly attributable to something else, like blunt force trauma. A COVID-19 death would also rely on PCR status since it would have to also be deemed a ‘case’, by definition.
 |
John Beaudoin has been an absolute warrior tracking deaths, COVID-19 and otherwise, using death certificate data from Massachussetts and you can read about that here in this article written by Madhava Setty, and here. He is also going to make an appearance on Dr. Drew soon to explain much of what he has discovered. Stay tuned.
Here’s a definition of a COVID-19 death that was being used in Massachusetts:
The current definition in Massachusetts is someone who has the virus listed as a cause of death on their death certificate, or someone who has had a COVID-19 diagnosis within 60 days and does not have it listed as their cause of death on their death certificate.²
Just to be clear here, that little ‘or’ has staggering implications. It means that if an individual was brought to a hospital after being in a deadly car crash, and was ‘tested’ for COVID-19 (as was the standard) prior to dying (or perhaps… after?), and that ‘test’ ‘came back positive’, then that individual, whose death certificate might have otherwise read: “massive internal bleeding from car crash” (not COVID-19) would be officially written down as a COVID-19 death.
Scott McLachlan reminded me of Norman Fenton’s example that demonstrates the defectiveness of this definition well. Consider an individual who gets exposed to SARS-CoV-2, gets ‘tested’, recovers, and then 59 days later gets killed in a car crash. This individual would be considered a COVID-19 death.
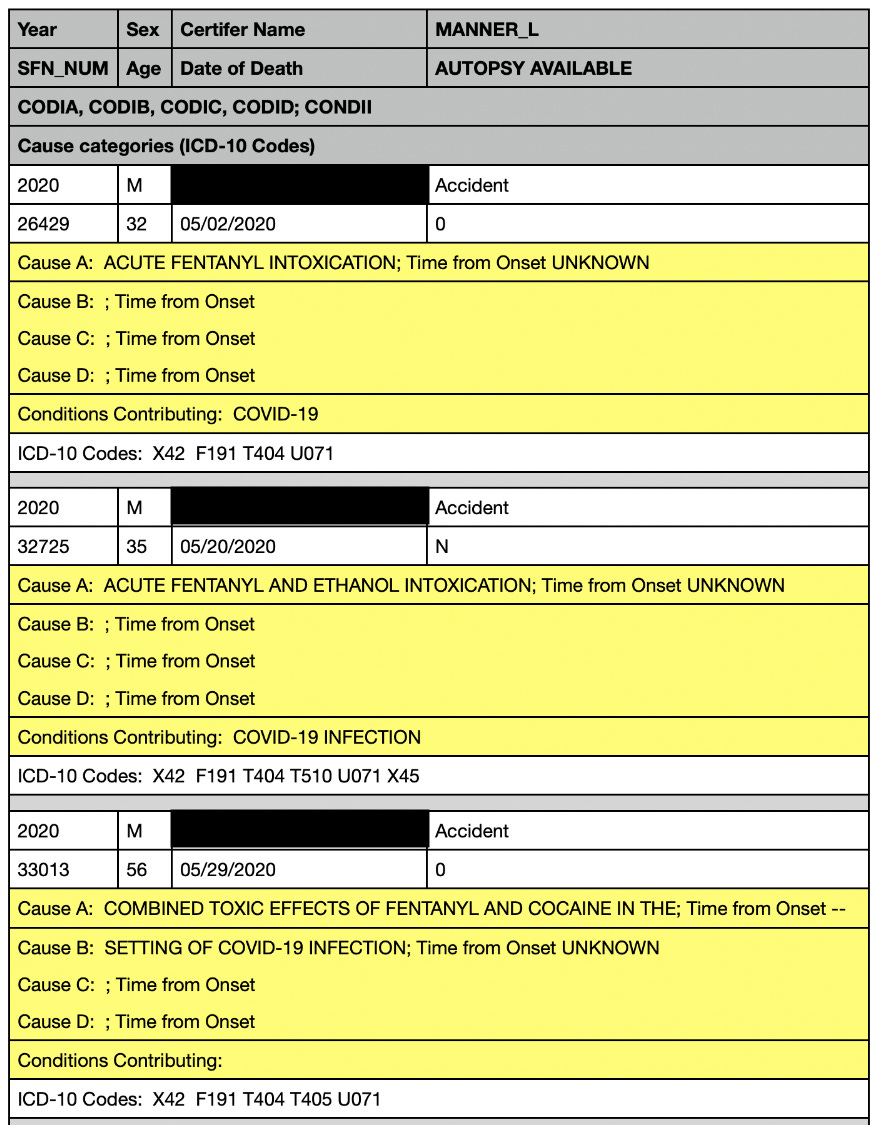
The following vital record reports in Figure 3 produced by Monsieur Beaudoin, show 3 individuals who died from fentanyl use (Overdose → OD) with COVID-19 listed as a cause of death or a contributing condition. As John pointed out to me:
‘A’ is the immediate cause or the last thing that happened before death. ABCD are reverse time order as causes of death. Whichever is the last one listed is what I call the root cause, but CDC calls the Underlying cause UCOD. Part II (conditions contributing) is for conditions contributing to death or possibly contributing to death. If covid is causal, it should be the last in part I (Causes A-D).
So if COVID-19 is the cause of death, it should be Cause D, by my understanding. But to be honest, I still don’t know the answer to the question: Were these 3 individuals written up as COVID-19 deaths? As in, would their deaths count as COVID-19 deaths in the database for the cumulative count of COVID-19 deaths in the United States? I believe the answer is ‘yes’ based on the fact that these 3 individuals have ‘the virus listed as a cause of death on their death certificate’. This is preposterous.
 |
You might also find it interesting to know that the timeframe in the definition of a COVID-19 death was changed from 60 days to 30 days and this subsequently lowered the number of COVID-19 deaths by 15%. How much lower would that percentage be if mis-assigned deaths that were clearly from trauma, like the kind sustained from a car crash were removed from the COVID-19 death count? Would COVID-19 still be the #1 cause of death? I dare say, no way.
I found another definition of a COVID-19 death that read:
In April 2021, a death was classified as COVID-19-associated if it was determined that the virus directly caused or contributed to the person’s death, the person had a diagnosis within 60 days and had no other obvious cause of death, such as trauma.³
This makes far more sense to me since at least car crash victims could not have COVID-19 written up as the cause of death. But a ‘diagnosis’ within 2 months? And was this an actual diagnosis or a best guess based on a sketchy ‘test’ and pneumonia-like symptoms?
The CDC also have a definition of a COVID-19 death:
A COVID-19–associated death occurred in a person with a documented COVID-19 diagnosis who died, and whose report local health authorities reviewed (e.g., using vital records, public health investigation, or other data sources) to make that determination. Per national guidance, this group should include persons whose death certificate lists COVID-19 disease or SARS-CoV-2 as an underlying cause of death or as a significant condition contributing to death. Rates of COVID-19 deaths by vaccination status are reported based on when the patient was tested for COVID-19, not the date the patient died.⁴
Again, the question about ‘diagnosis’ arises. And that last phrase is a bit weird to me. From what I understand, it means that 2 individuals, uninjected and injected, who both died on the same day, but were ‘tested for COVID-19’ in January and March, respectively, will have their ‘COVID-19 death’ report written down as having occurred in January and in March, respectively, not both in March when they actually died.
But did we even need symptoms? According to Norman Fenton, we did not.
In the UK a covid case ONLY required a positive PCR test (symptoms were not needed) and anybody who was PCR positive within 28 days of death had covid on their death certificate. 'Officially' (but only after 2 years) the UK government said they were only going to classify covid deaths those for which covid was a contributory factor.⁵
You can read about his analysis here. Just imagine the over-counting of the COVID-19 deaths!
The question remains, who was written down as a COVID-19 death, and what percentage of these were valid? In my opinion, there is no reason to ‘test’ an individual who ODs on fentanyl, for example, for COVID-19. Presumably, there is no relationship between their OD and whether or not they had some version of SARS-CoV-2 at one point or another. So every single death certificate with whereby the individual ODed should be unclassified as a COVID-19 death, if they were so classified. Same thing goes for trauma deaths. And a plethora of other mis-assigned deaths!
I think we can all agree based on these evidences that the actual COVID-19 death count is far lower than portrayed, so if we assume that COVID-19 death counts are lower in ‘reality’ than are being reported, then what I would like to know is this: Is the discrepancy between the over-count and real-count proportional over time?
We might also wonder what the incentives were behind mis-attributing cause of death. Were there incentives? Were there motives, or was it really just a difference in the number of days to COVID-19 ‘diagnosis’ issue? Was it simply a ‘diagnosis’ issue, for that matter, as in: mass misdiagnoses? Who assigned the 60 day timeframe? Who changed it 30 to manifest a lower COVID-19 death count? Did the switch to 30 days to lower the death count on March 11, 2022 have anything to do with making it look like the shots were working? Could the 60 days have been assigned to make it look like more people were dying from COVID-19 than actually were? Were doctors paid to write COVID-19 on death certificates as the cause of death? Were parents of demised children asked to change the cause of death to COVID-19? Why would a doctor who actually saw an individual die from car crash trauma include any information about COVID-19 on that individual’s death certificate with regard to cause of death?
Let’s be blunt. It would be to the benefit of the producers of COVID-19 injectable products and anyone profiting off of them, to over-count COVID-19 deaths to make it appear as though there was certainly a good reason to get ‘vaccinated’ - ie: to prevent severe illness or dying from COVID-19, for example, as per the guidelines and recommendations of the CDC. No one wants to die from ‘deadly virus’, right? Funny how people don’t seem to mind dying from an experimental injection. Sorry. I had to.
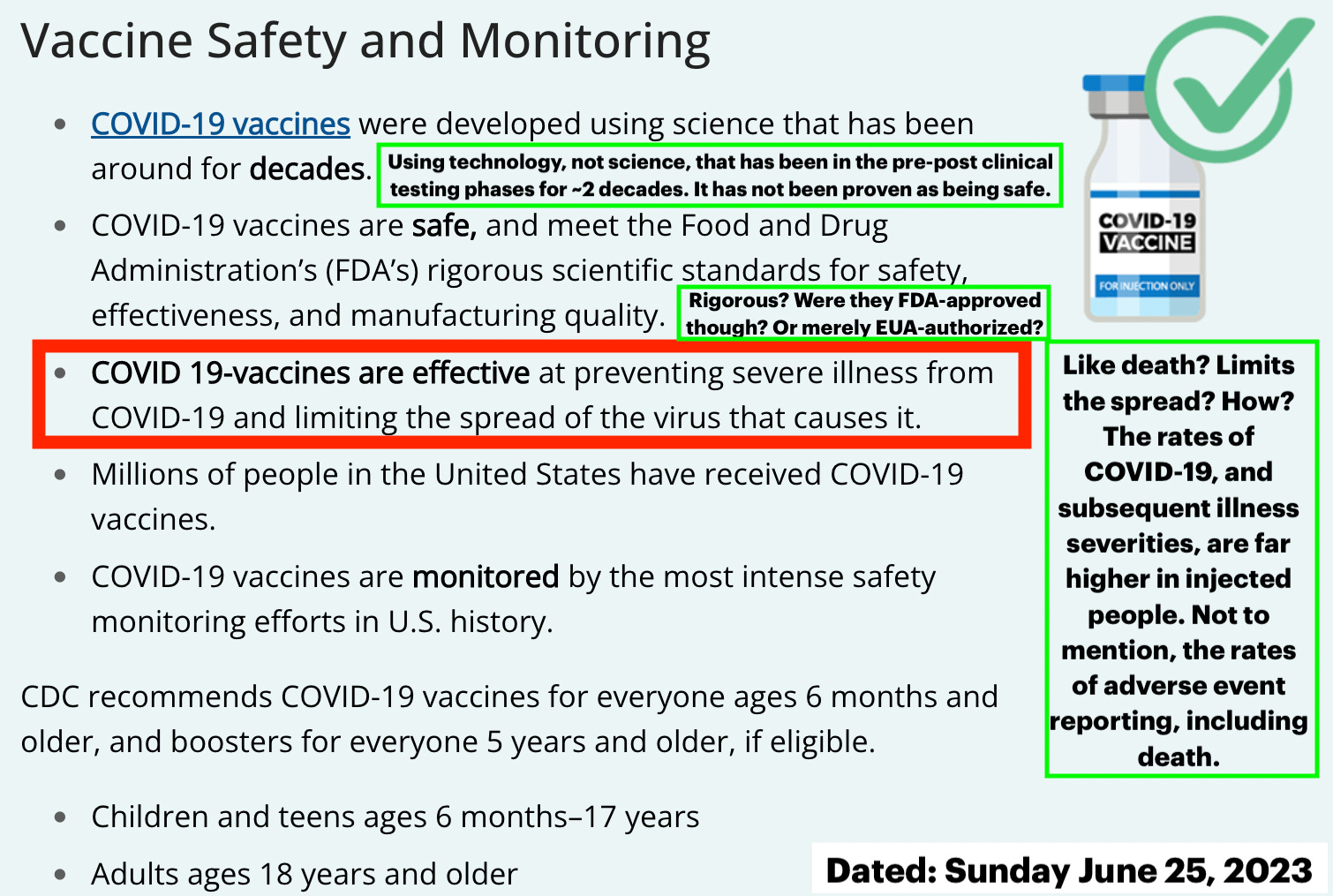 |
For some references to my snarky emboldened comments framed in bright green in Figure 4, go here, here, here and here. Please feel free to add references in comments.
So… in the face that the ‘COVID-19 death’ count is far lower than it has been made to appear…
What is a COVID-19 death?
I consulted with my all-cause mortality buddies (Jonathan, Martin, Norman, Clare, Joel, Danny, Shahar, Retsef, Josh and a mouse) on this and got a great array of answers. To me, the following would be a suitable definition:
An individual who presents with respiratory symptoms associated with SARS-CoV-2 infection - as confirmed by sequence validation - who subsequently progresses to severe COVID-19 (due to withholding of life-saving treatments⁶) and death.
This definition would not weed out respiratory-related (pneumonia) cases with nosocomial (hospital-acquired) SARS-CoV-2 involvement.⁷ The number of pneumonia death cases with COVID-19 as a true contributing condition⁸ are likely quite low, and would depend on the timeframe to death from exposure to SARS-CoV-2 and the frailty of the individual. In these rare cases, however, it would be appropriate to list COVID-19 as a contributing condition on the death certificate.
But the thing is that this definition was not used and it begs the question: How many people who had non-SARS-CoV-2 respiratory symptoms went to the hospital and got ‘tested’, died and deemed a COVID-19 death? All of them, by my guess. So that basically means, everyone. Every pneumonia case. So how many COVID-19 deaths were there in actuality?
I dare say that Denis Rancourt, whose work I admire and appreciate, would likely claim there were no COVID-19 deaths, since he would argue that all of the deaths occurred due to effects that the humans imposed, and not due to the effects of a virus.
Let’s agree for argument’s sake, since I would like to examine some data (and we are using government-sourced data) that a COVID-19 death includes individuals whose death certificate lists COVID-19 disease or SARS-CoV-2 as an underlying cause of death or as a significant condition contributing to death, as per the CDC definition. Let’s just accept for now that many, many individuals (perhaps all) have been counted as COVID-19 deaths that weren’t.
On COVID-19 death data
As previously mentioned, according to this USA health rankings collective database, COVID-19 became the #1 cause of death in the United States in mid-November 2020. This is ~30 days before the initial roll-out of the COVID-19 injections started. Remember, there were still some tens of thousands of people enrolled in the clinical trials at this time. It stayed in the #1 position for 905 days (2 years, 5 months, 24 days excluding the end date). Well done, COVID-19. Well done.
Question: Shouldn’t the shots have brought the COVID-19 death count down during this timeframe if they were effective at preventing severe illness and death?
1.1 On death count decline
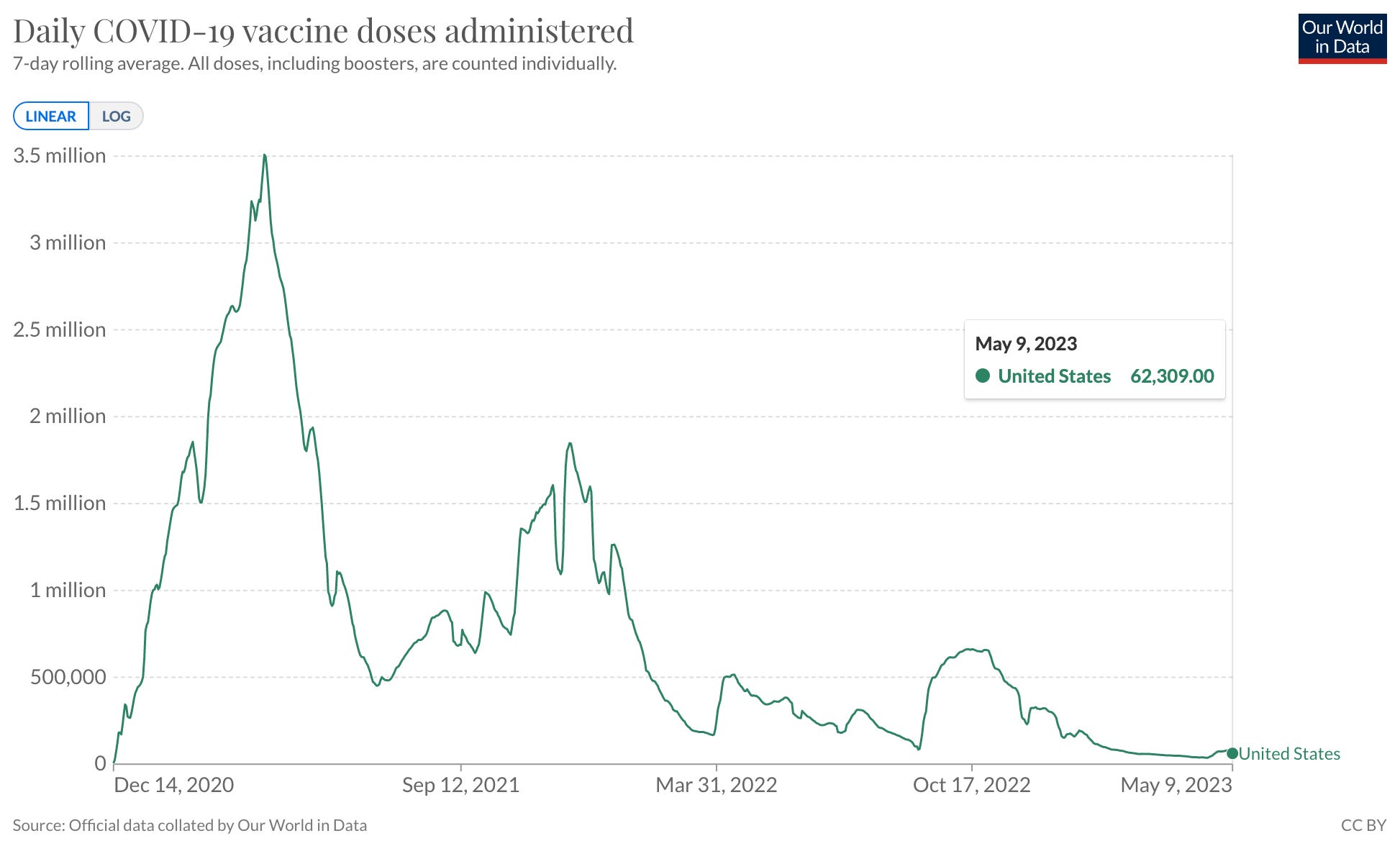
Regardless of the over-exaggerated death count, it should still have declined over the injection timeframe if the shots worked. The COVID-19 injections were rolled out and administered aggressively starting late December 2020. The reception of the injections has been waning however - much like the immunity conferred - since about the end of 2021. In Figure 5 below, Our World in Data (OWID)⁹ demonstrates the roll-out as per number of daily doses administered in the United States from December 2020 through to May 2023. To date, ~677,000,000 doses have been administered in the United States.¹⁰ You can see that approximately half of these doses were administered by late June 2021.
 |
1.2 On timing of death count decline
I would assume that shortly after the injections were rolled out that the number of COVID-19 deaths would start to decline, I mean, given that the shots are ‘safe’ and ‘effective’ at reducing severe illness and death. The timeframe of highest injection rates spans 2021, and it is clear to see according to your friendly neighborhood gates-funded OWID, that the COVID-19 death rate decays steadily following the roll-out of the shots. Now if the shots had any longevity, as would be the case in a natural infection scenario, the COVID-19 deaths would continue to decline until there were no more.
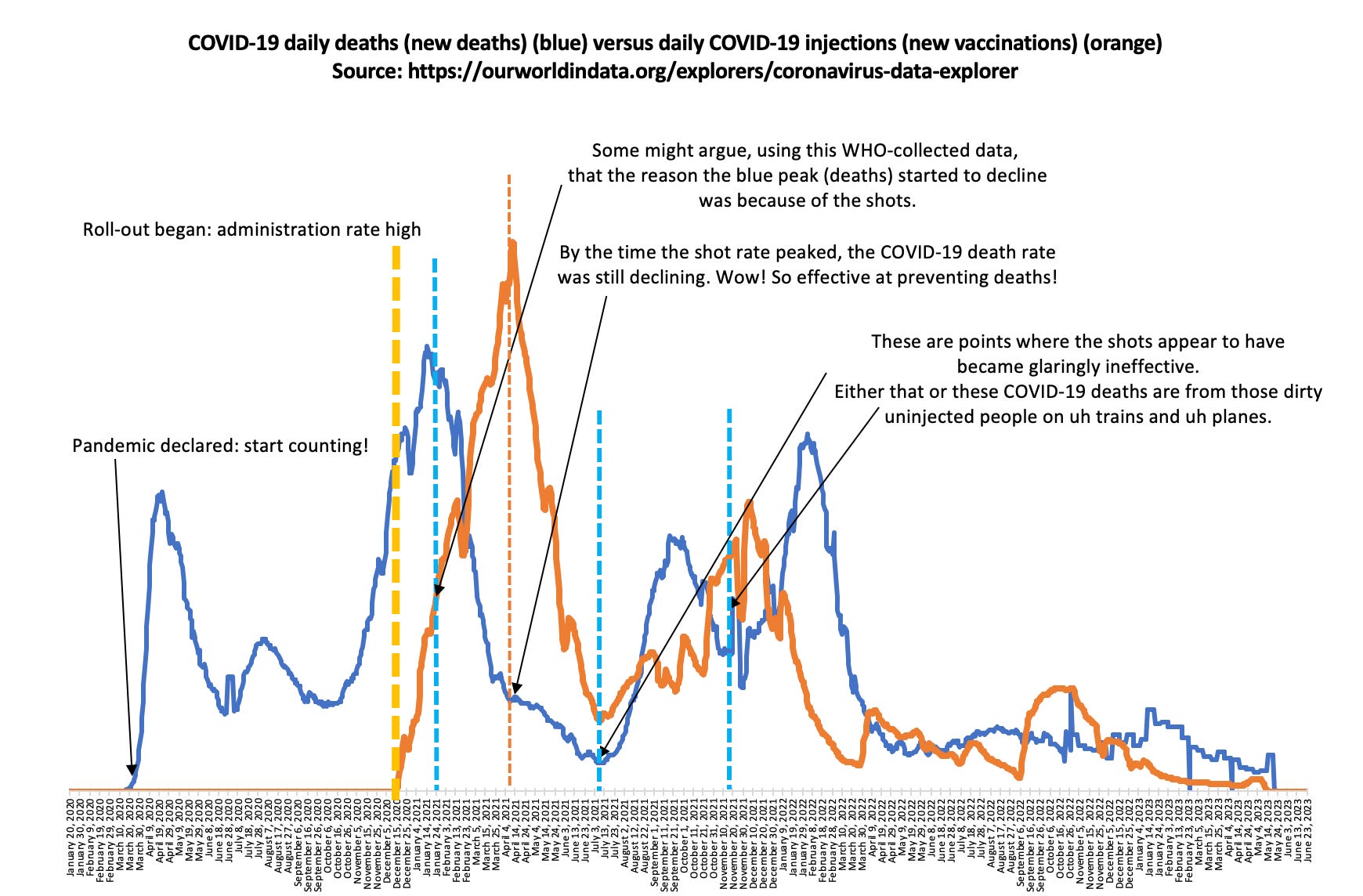 |
But there are resurgences of COVID-19 deaths. How can this be? Could it be that these are the uninjected people are getting COVID-19 and dying? Or could it be that the injections just became ineffective due to mutations?
Or… put on your tinfoil hats folks… Could it be that the COVID-19 deaths are actually pneumonia deaths? That would certainly explain why the COVID-19 shots were not working to reduce these deaths.
1.3 On pneumonia deaths
I downloaded the National Center for Health Statistics (NCHS) Mortality Surveillance data for influenza, pneumonia and COVID-19 deaths and first checked to see if the COVID-19 deaths matched OWID. They did. Perfectly. Then I decided to plot the influenza deaths. Not many there. Moving on. Then, I decided to plot the pneumonia deaths. Are my eyes deceiving me or are COVID-19 deaths actually pneumonia deaths?
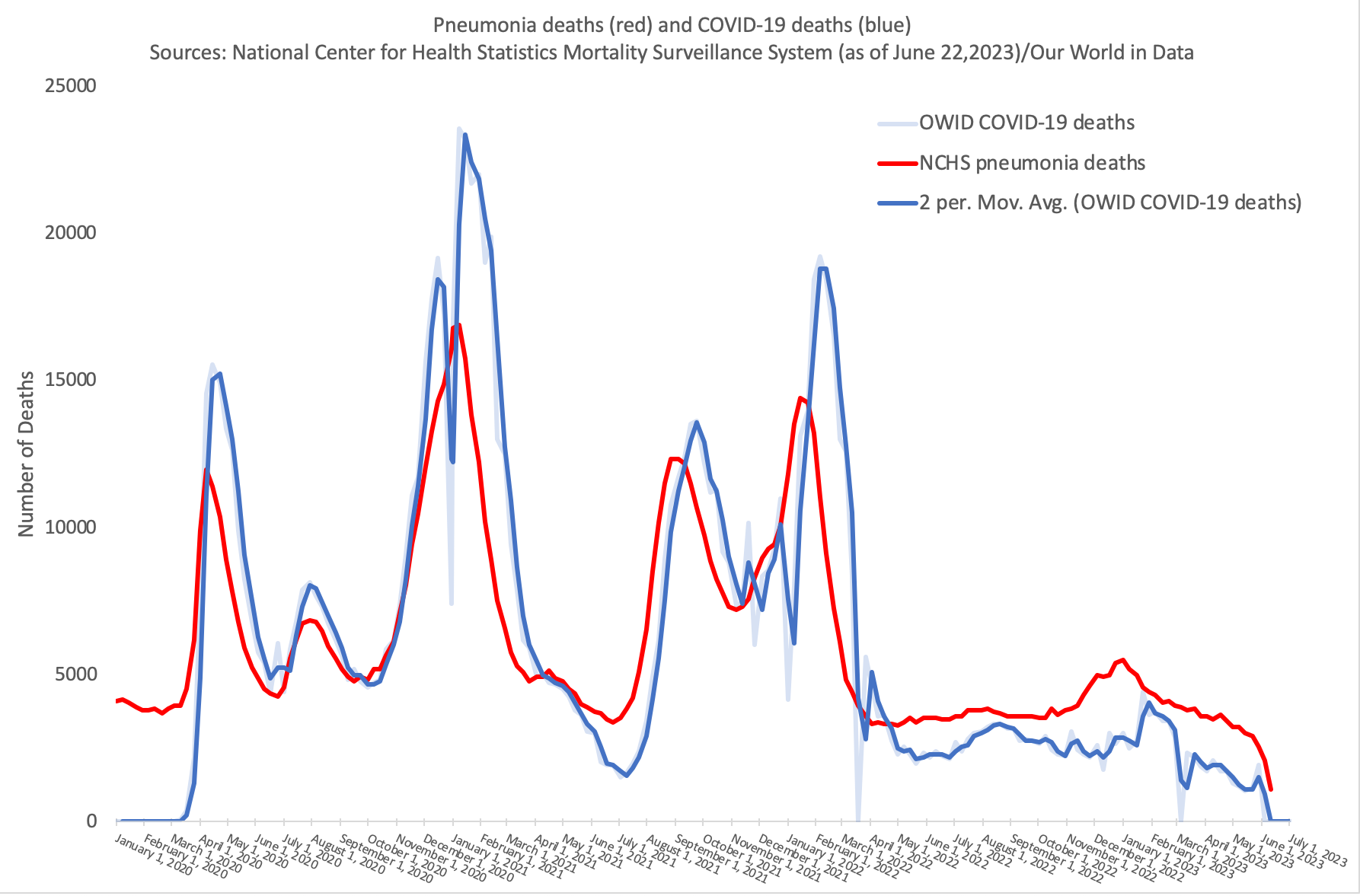 |
Now I might be getting this wrong, but it seems from this data that we can promptly answer the question: What is a COVID-19 death?
A COVID-19 death is a pneumonia death.
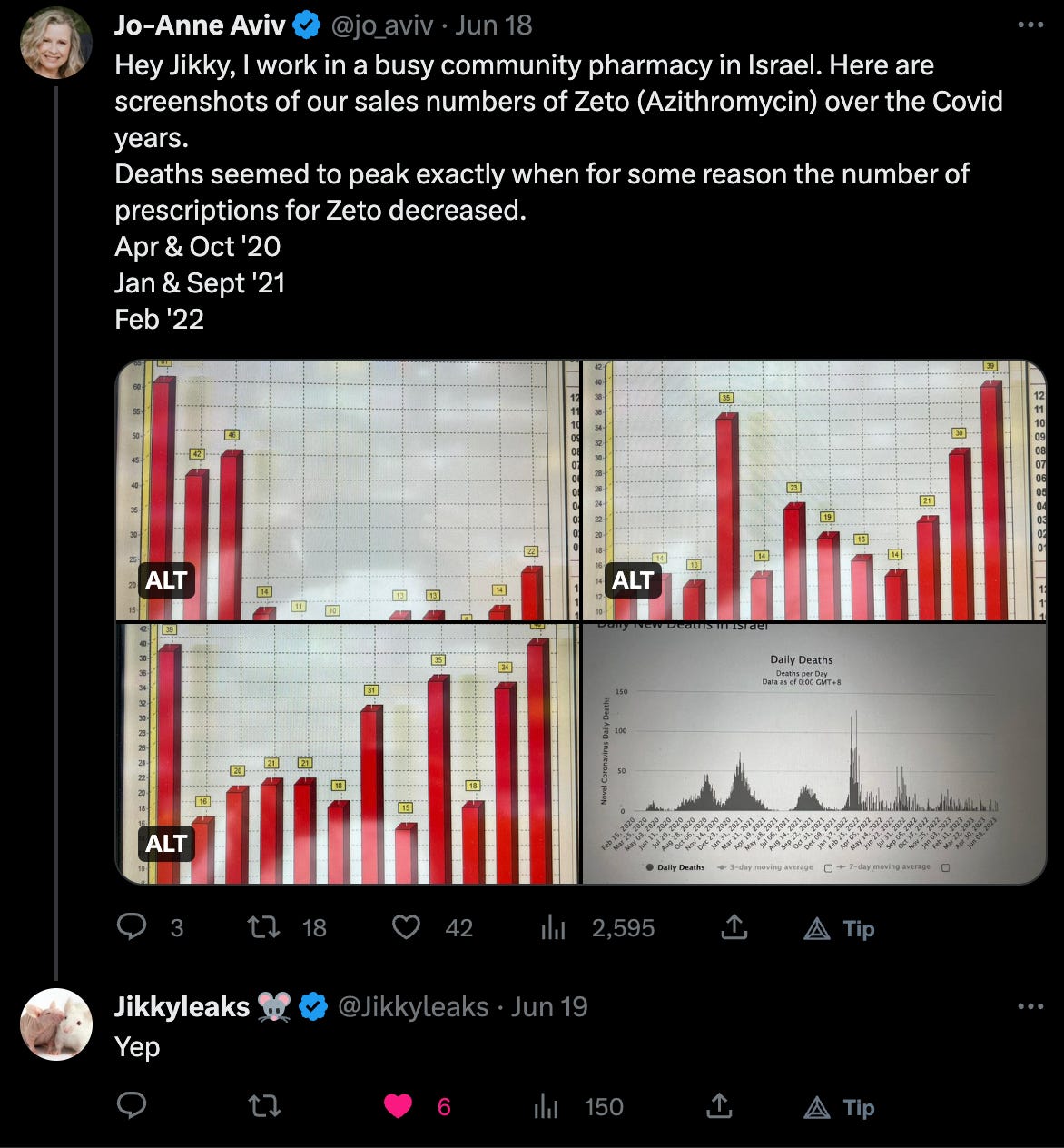
I believe that this is something that Jikkyleaks (#3tablets) and JJ Couey have been saying for a long time. Remember how regular antibiotics were made unavailable? In the face of all this ‘viral’ testing, antibiotics would have been ‘justifiably’ thrown off the table. Remember how you were instructed to go turn cyanotic if you were suffering from respiratory symptoms? Remember how they continue to push face coverings that promote secondary infections and exacerbate existing ones? Geez, it makes sense, doesn’t it? The excess deaths in the COVID-19 death group are likely the over-shoot from mis-attribution of other causes of death. Pneumonia + everything else = COVID-19 deaths.
 |
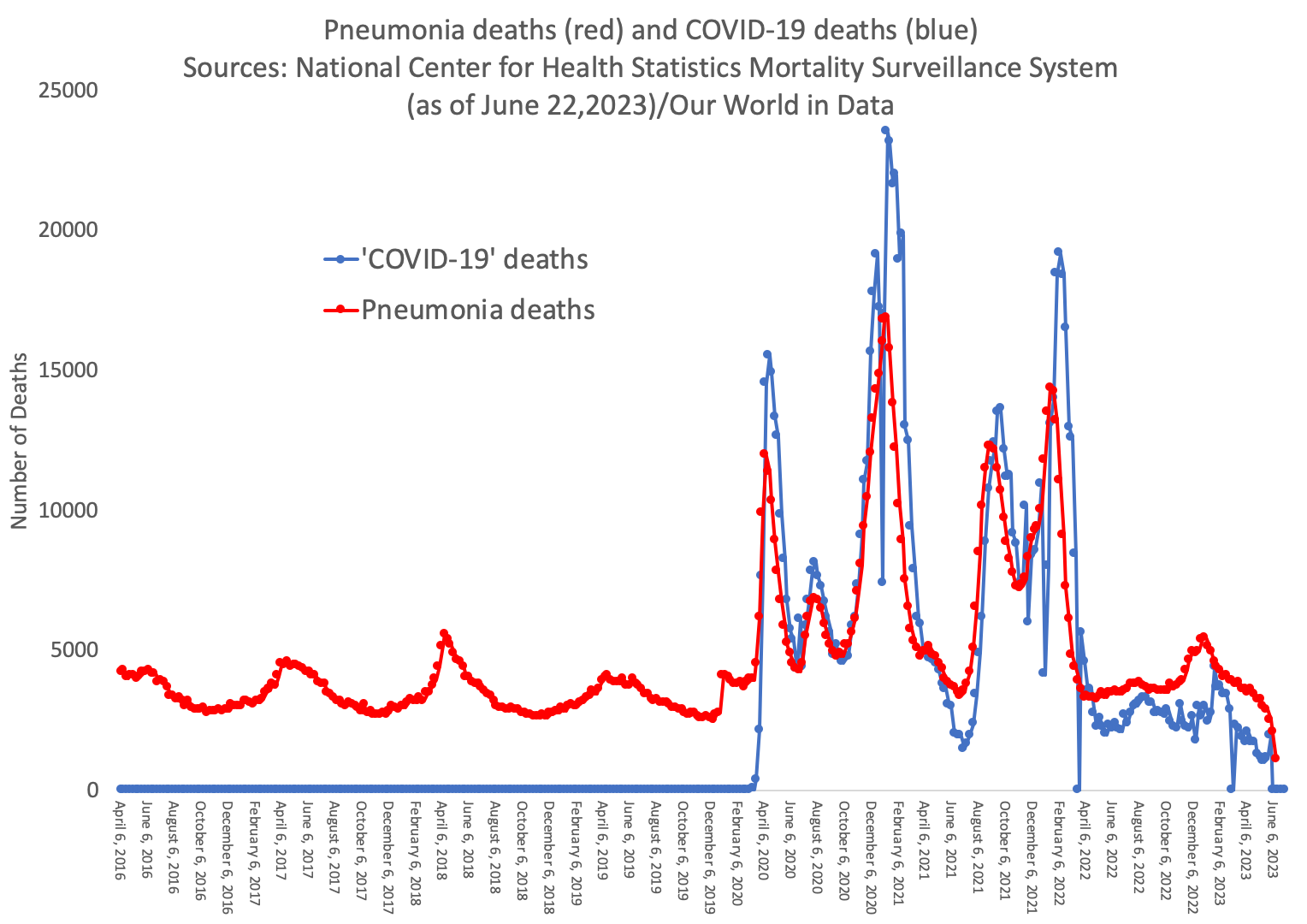
I wanted to go one step further and to check what pneumonia deaths looked like historically so I downloaded more data and plotted it against the existing pneumonia and COVID-19 data. Again, this is looking a lot like COVID-19 deaths are nothing more than pneumonia deaths that were seriously inflated - likely due to withholding of antibiotics that normally would have spared lives.
 |
I had a lot more written here to try to explain the resurgence of COVID-19 deaths in the face of the injections, but I don’t think I need to. The deaths are ebbing and flowing as they always do seasonally; the only difference here is the magnitude which is explained by withholding of standard antibiotics and medications. The mis-treatment of humans, especially elderly humans, during the ‘pandemic’ killed a lot of people.
Our elders were isolated and abandoned and left without life-saving drugs.
On WHY
So, why? Why on Earth would they do this? Why would they make up a definition of a COVID-19 death, make it depend on a fraudulent PCR ‘text’, request doctors to write-up COVID-19 as the cause of death in cases where it was not, and swap in the pneumonia data and call it COVID-19?
Well, besides burgers, ice cream and money, not wanting to die from the horribly deadly new virus might incentivize someone to take a shot promised to save them from death.
Remember, remember the 21st of Julember, the gaslighting, bad reason and plot. I see no reason, why gaslighting and bad reason, should ever, be, forgot.
You're not going to -- you're not going to get COVID if you have these vaccinations.
This is what an acting president said publicly on July 21, 2021.
We all know now that the above quoted Biden words were incorrect, and in fact, as more and data becomes ‘available’ via FOIA requests, we learn that these words were never based on scientific data to begin with.
Rochelle Walensky, the former director of the CDC was asking her colleagues about solving the problem of ‘Vaccine breakthroughs’ on January 30, 2021. You can read about that here. As a reminder, a ‘Vaccine breakthrough’ is the result of a leaky vaccine whereby the individual ‘vaccinated’ results in infection - and pathologies associated with - the virus at which the ‘vaccine’ was originally aimed to provide protection against.
A breakthrough infection is a case of illness in which a vaccinated individual becomes infected with the illness, because the vaccine has failed to provide complete immunity against the pathogen (currently only viruses).
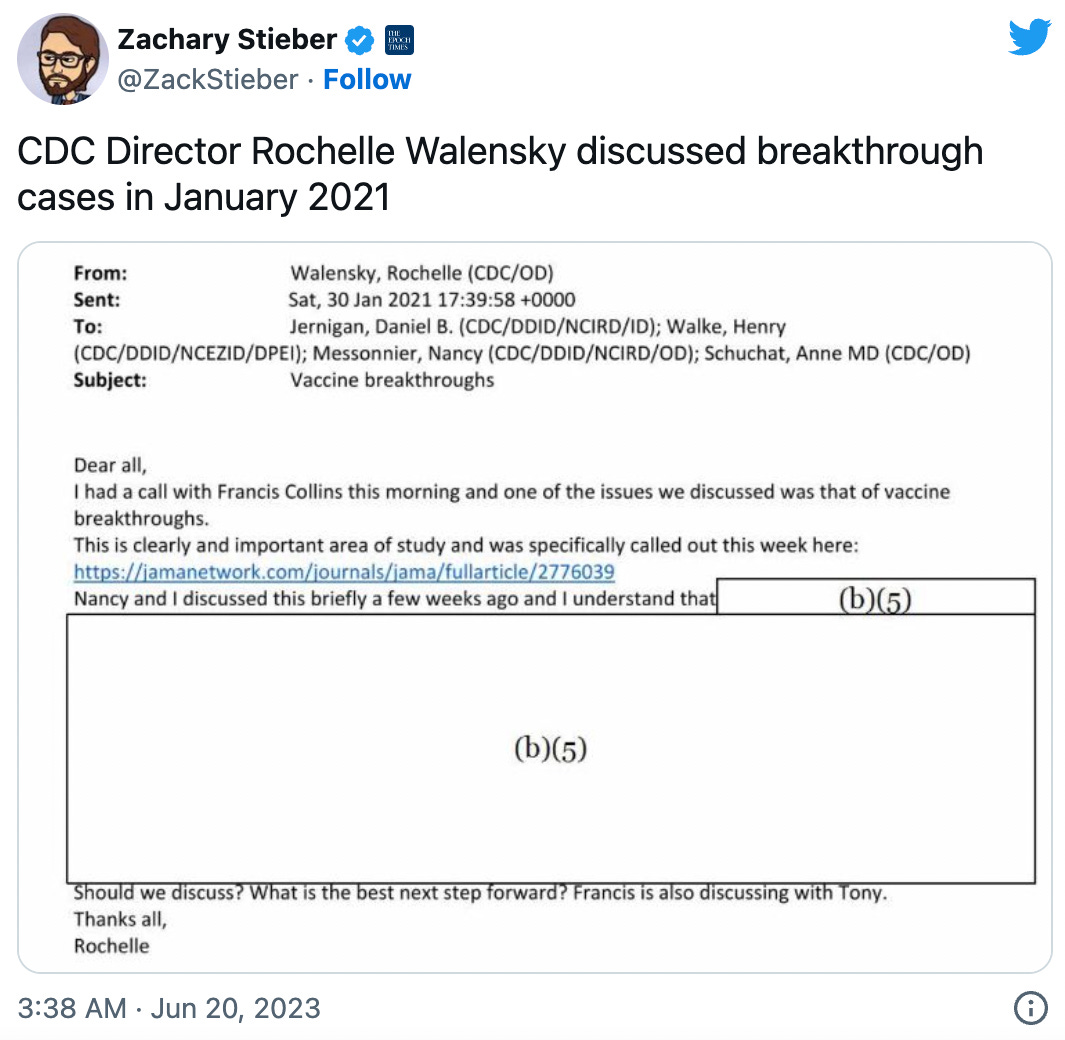 |
Walensky raised this concern in January 2021, and 5 months later, Biden was stating publicly that breakthrough infections don’t exist - you are immune to SARS-CoV-2 and won’t get its associated disease (COVID-19) if you are injected. I would assume that Biden consults with the CDC, so I would also assume that he knew that the COVID-19 injections were not effective at preventing COVID-19, ie: were associated with ‘Vaccine breakthrough’. He was, in fact, by his own words in White House remarks, insistent and even threatening at times, by my assessment. He referred to the pandemic as a ‘pandemic of the unvaccinated’ and warned that ‘[their] patience is wearing thin’. I implore everyone to read his words. There is a lot to unpack in his remarks.
And my message to unvaccinated Americans is this: What more is there to wait for? What more do you need to see? We’ve made vaccinations free, safe, and convenient. The vaccine has FDA approval. Over 200 million Americans have gotten at least one shot. We’ve been patient, but our patience is wearing thin. And your refusal has cost all of us. So, please, do the right thing. President Joe Biden
The specific words in the above quote sounds like desperation to me. There is no need for desperation. There never was a deadly virus to contend with. Unless the desperation was out of a need to get every single American woman, man and child injected for some other reason. Money? Power? Compliance testing? Population control? All of the above?
Concluding remarks
We can say with utter confidence that the injections do nothing to prevent ‘COVID-19’ deaths
COVID-19 deaths are not COVID-19 deaths
COVID-19 deaths are pneumonia deaths.
I have said this before and it warrants repeating, this was a pandemic of testing. If this testing insanity had not been ‘a thing’, then diagnoses would not have been dependent on it and death certificates wouldn’t have been alterable using this as a distinguishing feature and there would not have been a way to masquerade pneumonia deaths as COVID-19 deaths.
OUR DATA: We use the most recent data from these primary sources: WHO, World Bank, UNESCO, CIA and individual country databases for global health and causes of death. We use the CDC, NIH and individual state and county databases for verification and supplementation for USA data.
https://turnto10.com/news/local/massachusetts-department-public-health-change-diagnosis-redefines-covid-19-death-after-significant-overcount
https://www.wcvb.com/article/massachusetts-health-officials-new-criteria-for-counting-covid-19-deaths/39398221#
https://www.cdc.gov/mmwr/volumes/71/wr/mm7104e2.htm
https://wherearethenumbers.substack.com/p/the-uk-governments-flawed-covid-death
Again, sorry. I had to.
Jewkes SV, Zhang Y, Nicholl DJ. Nosocomial spread of COVID-19: lessons learned from an audit on a stroke/neurology ward in a UK district general hospital. Clin Med (Lond). 2020 Sep;20(5):e173-e177. doi: 10.7861/clinmed.2020-0422. Epub 2020 Jul 27. PMID: 32719035; PMCID: PMC7539735.
To determine whether or not COVID-19 is a contributing condition would depend on the timeframe to death and the frailty of the individual.
Edouard Mathieu, Hannah Ritchie, Lucas Rodés-Guirao, Cameron Appel, Charlie Giattino, Joe Hasell, Bobbie Macdonald, Saloni Dattani, Diana Beltekian, Esteban Ortiz-Ospina and Max Roser (2020) - "Coronavirus Pandemic (COVID-19)
https://ourworldindata.org/explorers/coronavirus-data-explorer?zoomToSelection=true&time=2020-03-01..latest&facet=none&country=~USA&pickerSort=asc&pickerMetric=location&Metric=Vaccine+doses&Interval=Cumulative&Relative+to+Population=false&Color+by+test+positivity=false
| |||||
| |||||
Jessica's Substack Input |
![]()
![]()
No comments:
Post a Comment