New Study Supports Conclusion of Retracted 2020 Study Showing Unvaxxed Kids Healthier Than Vaxxed
A new study by James Lyons-Weiler, Ph.D. and Dr. Russell Blaylock supports the conclusions of a study by Dr. Paul Thomas, published in November 2020 and later retracted after an anonymous reader expressed concerns.

Miss a day, miss a lot. Subscribe to The Defender's Top News of the Day. It's free.
In November 2020, a study that carefully examined 10 years’ worth of data from a pediatric practice in Oregon run by Dr. Paul Thomas was published. Five days following the publication of the study, Thomas’ license was suspended.
A month after that, the journal decided to inform the authors that an anonymous reader had expressed some concerns about the study.
This single reader’s comments that involved bad guesswork led ultimately to the journal’s decision to retract the paper, leaving the authors stunned.
The authors knew that the reader’s concerns had already been addressed during peer review, and expected the journal to rule in favor of not retracting the paper. The journal editorial board knew this, too.
The concern centered primarily on the question of whether the large differences in the number of medical visits required for attention to specific health conditions like anemia, gastroenteritis, asthma, ear infections and many others, were due to parents who did not vaccinate not showing up to their well-baby and well-child visits.
Because Thomas’ license was suspended, he had to focus on his case and try to keep his life from falling apart; the medical board kept postponing the hearing, and no hearing had occurred.
In fact, no hearing has been held to date.
James Lyons-Weiler, Ph.D. suggested to Thomas that perhaps the medical board had overreached by applying a penalty without due process, a fact that Thomas then shared with his lawyer.
When his lawyer wrote the medical board pointing out that Thomas had suffered a penalty without due process, they offered to reinstate his license, pending the outcome of a hearing, on the condition that he do no more research.
This clearly shows the agenda of the medical board was not to ensure that the children in the practice were receiving good pediatric medical care.
It is now clear that the singular priority of the medical board was to shut down Thomas’ practice of abiding by informed consent — as required by Oregon state law for all medical procedures — and to prevent him from sharing any additional findings from the 10 years of data that had been collected from his practice.
New study supports earlier conclusions by Thomas
Today, the study is revived by a second study, this time conducted by Lyons-Weiler and his medical collaborator, Dr. Russell Blaylock.
In this second study, the following questions were addressed:
- Which group of patients adhered to the regular well-child visit better, the vaccinated patients or those who had refused vaccines?
- In groups of patients matched for health check visitation usage, which adverse health outcomes following vaccination differed between vaccinated patients and those who refused vaccines?
- After adjusting for healthcare visitations and age, do vaccines still significantly affect overall adverse health conditions in a manner independent of their interaction with healthcare visitations and age?
- Did older patients in the practice who stopped vaccinating experience a decrease in the adverse health outcomes that have been attributed to vaccines?
The study results, which are found in the paper entitled “Revisiting Excess Diagnoses of Illnesses and Conditions in Children Whose Parents Provide Informed Permission to Vaccinate Them” show that the anonymous reader’s concerns were unfounded; the unvaccinated families made their well-child visits with greater frequency than the vaccinated families.
This study, funded by the public, answers the first questions.
The answer to the second question is “results vary,” but this may be due to smaller sample sizes reducing power (see the study for details).
The study split the patients into high, medium and low health care visitation usage blocks, and many of the adverse health effects are seen increased in the vaccinated group of patients within these blocks (blocks are groups of patients matched on health care visitation usage).
For the third question, the scientists found that after defining a model that included healthcare visit utilization and age, vaccines were still a significant factor that increased adverse health outcomes, many of which had previously been associated with vaccines.
Moreover, the authors also determined that vaccines were still significant following consideration of the interaction term between vaccination status and the other model factors.
Importantly, had the study authors not considered the interaction term, the results would have seemed to imply that vaccination was negatively predictive of adverse health outcomes.
In the model in which vaccines, health care visits per age and the interaction term was considered, the number of vaccines was a positive significant predictor of overall adverse health.
Interaction terms are usually ignored by studies that “adjust for” variables. Adding covariates into the model without considering the interaction term with the main effect — vaccines — can mask a significant effect on the rates of post-vaccination health issues, providing a misleading result.
It’s worth noting that breastfeeding — another correlate of lifestyle measures — had no significant singular or interaction effects.
Blaylock posed the final question to Lyons-Weiler, who conducted the data analysis.
When older children were studied, and those who had the most vaccines were compared to those to those of the same age who had fewer vaccines, a clear pattern emerged for most of the adverse health outcomes: the risk of having a higher adverse health outcome was higher in the most-vaccinated older children compared to the least-vaccinated older children to a degree that was larger than that expected given any variation between the two groups in healthcare visit utilization.
This reflects the positive health effects of vaccine cessation.
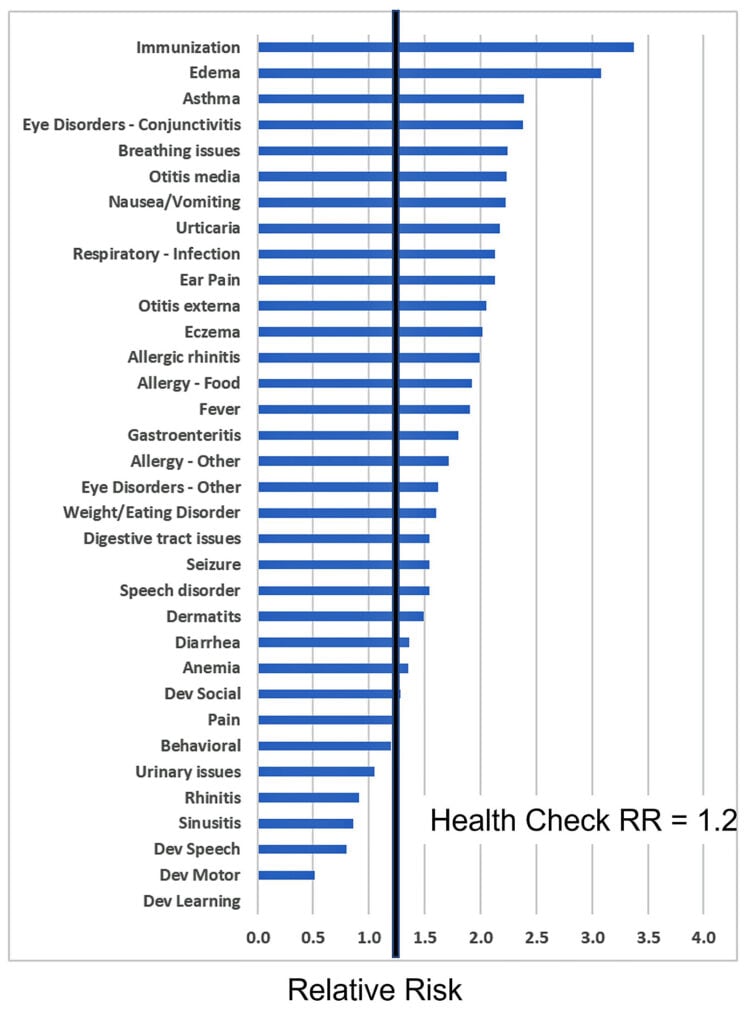
The relative risk of adverse health outcomes in older children who continued to vaccinate compared to those who ceased vaccination in Thomas’ practice.
Combined, all of these results mean that the method developed by Lyons-Weiler to consider the number of office visits needed for adverse health outcomes represents a robust, reliable and rigorous advance in methodology for the study of adverse health outcomes following medical exposures, including vaccines.
The method, “Relative Incidence of Office Visits,” had already been shown to be more powerful.
Lyons-Weiler reports that this is necessarily so because the measure contains more information than mere rates of diagnosis.
The RIOV measure has a higher dynamic range than odds ratios and relative risks based on diagnosis only. Studies that focus on the rates of diagnosis are using a subset of RIOV but are only limiting their count of office visits to that for the initial diagnosis.
The authors estimated that vaccination increases the need for visits to the doctor for vaccine-related health outcomes at a rate of 2.56 to 4.98 new chronic-illness-related visits per unit increase in vaccination per year.
“That translates into far more chronic illness in vaccinating children than in those not vaccinating, a disease burden that is not considered in risk: benefit considerations when it comes to vaccine policies and laws,” said Lyons-Weiler.
The paper, which was subjected to blinded peer review, describes all of the details of the results, is open access, and is published in the peer-reviewed journal International Journal of Vaccine Theory, Research, and Practice.
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the views of Children's Health Defense.
