Why did politicians ever lockdown society in the first place? Can we
all agree that the stated purpose was to “flatten the curve” so our
hospital system could handle the inevitable COVID-19 patients who needed
care? At that point, at least, back in early March, people were
behaving rationally. They accepted that you can’t eradicate a virus, so
let’s postpone things enough to handle it. The fact is, we have done
that, and so much more. The headlines are filled with dire warnings of a
“second wave” and trigger-happy Governors are rolling back regulations
to try to stem the tide of new cases. But, is any of it actually true
and should we all be worried? No, it’s not a second wave. The COVID-19
virus is on its final legs, and while I have filled this post with
graphs to prove everything I just said, this is really the only graph
you need to see, it’s the CDC’s data, over time, of deaths from COVID-19 here in the U.S., and the trend line is unmistakable:
If virologists were driving policy about COVID-19 rather than public
health officials, we’d all be Sweden right now, which means life would
effectively be back to normal. The only thing our lockdowns have done at
this point is prolong the agony a little bit, and encouraged Governors
to make up more useless rules. Sweden’s health minister understood that
the only chance to beat COVID-19 was to get the Swedish population to a
Herd Immunity Threshold against COVID-19, and that’s exactly what they
have done, so let me start there.
The Herd Immunity Threshold (“HIT”) for COVID-19 is between 10-20%
This fact gets less press than any other. Most people understand the
basic concept of herd immunity and the math behind it. In the early
days, some public health officials speculated that COVID-19’s HIT was
70%. Obviously, the difference between a HIT of 70% and a HIT of 10-20%
is dramatic, and the lower the HIT, the quicker a virus will burn out as
it loses the ability to infect more people, which is exactly what
COVID-19 is doing everywhere, including the U.S, which is why the death
curve above looks the way it looks. Scientists from Oxford, Virginia
Tech, and the Liverpool school of Tropical Medicine, all recently
explained the HIT of COVID-19 in this paper:
“We searched the literature for estimates of
individual variation in propensity to acquire or transmit COVID-19 or
other infectious diseases and overlaid the findings as vertical lines in
Figure 3. Most CV estimates are comprised between 2 and 4, a range
where naturally acquired immunity to SARS-CoV-2 may place populations
over the herd immunity threshold once as few as 10-20% of its
individuals are immune.”
“Naturally acquired herd immunity to COVID-19 combined with earnest protection of the vulnerable elderly — especially nursing home and assisted living facility residents — is an eminently reasonable and practical alternative to the dubious panacea of mass compulsory vaccination against the virus. This strategy was successfully implemented
in Malmo, Sweden, which had few COVID-19 deaths by assiduously
protecting its elder care homes, while ‘schools remained open, residents
carried on drinking in bars and cafes, and the doors of hairdressers
and gyms were open throughout.”
One of the most vocal members of the scientific community discussing
COVID-19’s HIT is Stanford’s Nobel-laureate Dr. Michael Levitt. Back on
May 4, he gave this great interview to the Stanford Daily
where he advocated for Sweden’s approach of letting COVID-19 spread
naturally through the community until you arrive at HIT. He stated:
Stanford’s Nobel-Laureate Dr. Michael Levitt
“If Sweden stops at about 5,000 or 6,000 deaths, we will know that
they’ve reached herd immunity, and we didn’t need to do any kind of
lockdown. My own feeling is that it will probably stop because of herd
immunity. COVID is serious, it’s at least a serious flu. But it’s not
going to destroy humanity as people thought.”
Guess what? That’s exactly what happened. As of today, 7 weeks after his prediction, Sweden has 5,280 deaths.
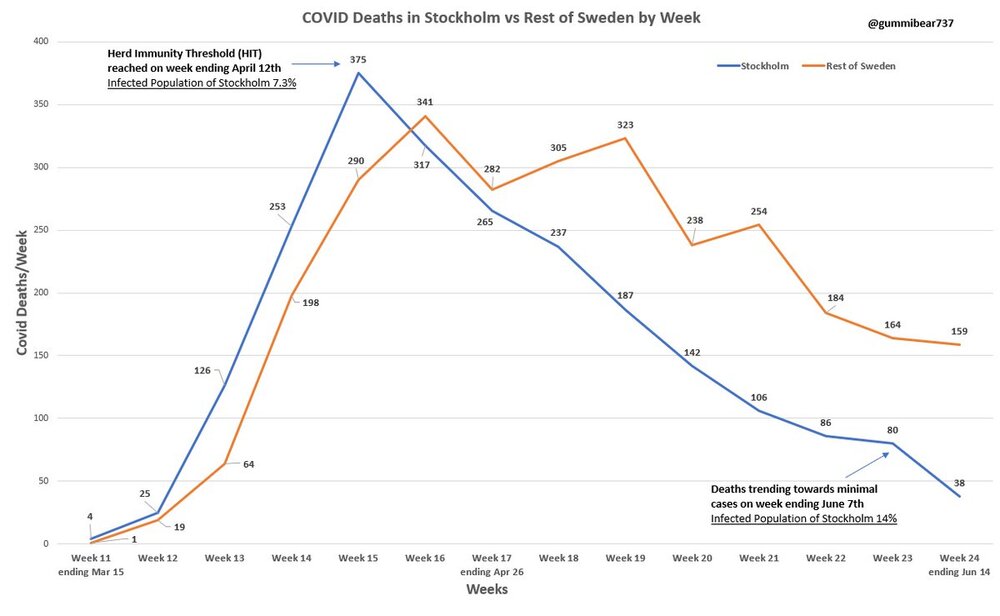
In this graph, you can see that deaths in Sweden PEAKED when the HIT
was halfway to its peak (roughly 7.3%) and by the time the virus hit 14%
it was nearly extinguished. (Shoutout to Gummi Bear on Twitter, a scientist who makes great graphs.)
How could Dr. Levitt have predicted the death range for Sweden so
perfectly 7 weeks ago? Because he had a pretty solid idea of what the
HIT would be. (If you’d like to further geek-out on HIT, check out: Why herd immunity to COVID-19 is reached much earlier than thought.) I absolutely LOVE Dr. Levitt (and as a Stanford alum, so proud he is a Stanford professor), watch this incredible video from just yesterday, go to 10:59 and just listen to this remarkable man!! Thrilled with his brand-new paper, released today, Predicting the Trajectory of Any COVID19 Epidemic From the Best Straight Line.
By the way, as a quick aside, and something else the press won’t
touch: COVID-19 is a coronavirus, and we have ALL been exposed to MANY
coronaviruses during our lives on earth (like the common cold). Guess
what? Scientists are now showing evidence that up to 81% of us can mount a strong response to COVID-19 without ever having been exposed to it before:
Cross-reactive SARS-CoV-2 T-cell epitopes revealed
preexisting T-cell responses in 81% of unexposed individuals, and
validation of similarity to common cold human coronaviruses provided a
functional basis for postulated heterologous immunity.
This alone could explain WHY the HIT is so much lower for COVID-19
than some scientists thought originally, when the number being talked
about was closer to 70%. Many of us have always been immune! If that’s
not enough for you, a similar study from Sweden was just released
and shows that “roughly twice as many people have developed T-cell
immunity compared with those who we can detect antibodies in.” (We kind
of knew this from the data on the Diamond Princess when only 17% of the people on board tested
positive, despite an ideal environment for mass spread, implying 83% of
the people were somehow protected from the new virus.) Quick Update: This article
came out one day after I wrote mine, and validated everything I just
said, except the author is wrong about COVID-19’s HIT, it’s 10-20%, not
60%, which is even better news:
“However,
it does provide a possible explanation for why the Covid-19 epidemic
seems to have died away in many places once it had infected around 20
percent of the local population (as judged by the presence of
antibodies). If people are developing some kind of immunity to Covid-19
via their T cells then it could mean that a far higher percentage of the
population has been exposed to Covid-19 than previously thought.
Antibodies and T cells combined, it is conceivable that some places such
as London or New York are already at or near the 60 per cent infection
level required to achieve herd immunity.”
Back to death rates over time.
We actually have our own Sweden here in the U.S. It’s called New York
City. In our case, we accidentally created a Sweden scenario, in that
we took our medicine quickly, because: 1) New York locked down so late
that they didn’t flatten anything, 2) they have the highest population
density in the U.S. in NYC, and 3) the public health officials and
Governors there made the bone-headed decision to send COVID-positive nursing home residents back to their nursing home,
accelerating deaths of the most vulnerable. What’s their death curve
look like today? In this case, I borrowed the graph from the NYC public
health website:
Hmm…notice anything about the chart or its slope? The reason deaths
from COVID-19 are dwindling down to nothing isn’t because Governor Cuomo
is a policy genius (in fact, he likely created more unnecessary deaths
than any other Governor with the nursing home decision), it’s because
the virus—like every virus in the history of mankind—is running out of
people to infect. The virus has a HIT of 10-20% and 70% of people are
likely naturally immune. Hosts are in short supply! That’s what viruses
do, and wait until you see what New York’s likely HIT is today.
Infection Fatality Rate. In my first blog post late last month, LOCKDOWN LUNACY: the thinking person’s guide,
I discussed Infection Fatality Rate in detail, so I am just going to
give a very quick summary here. Stanford’s Dr. John Ioannidis published a meta-analysis
(because so many IFR studies have been done around the world in April
and early May) where he analyzed TWELVE separate IFR studies and his
conclusion lays out the likely IFR for COVID-19:
“The infection fatality rate (IFR), the probability
of dying for a person who is infected, is one of the most critical and
most contested features of the coronavirus disease 2019 (COVID-19)
pandemic. The expected total mortality burden of COVID-19 is directly
related to the IFR. Moreover, justification for various
non-pharmacological public health interventions depends crucially on the
IFR. Some aggressive interventions that potentially induce also more
pronounced collateral harms1 may be considered appropriate, if IFR is
high. Conversely, the same measures may fall short of acceptable
risk-benefit thresholds, if the IFR is low…Interestingly, despite their
differences in design, execution, and analysis, most studies provide IFR
point estimates that are within a relatively narrow range. Seven of the
12 inferred IFRs are in the range 0.07 to 0.20
(corrected IFR of 0.06 to 0.16) which are similar to IFR values of
seasonal influenza. Three values are modestly higher (corrected IFR of
0.25-0.40 in Gangelt, Geneva, and Wuhan) and two are modestly lower than
this range (corrected IFR of 0.02-0.03 in Kobe and Oise).”
The data on IFR has now been replicated so many times that our own
Centers for Disease Control announced that their ‘best estimate’ showed
an IFR below 0.3%. In this article on the CDC’s new data, they also highlighted how the cascading declines in IFR has removed all the fears of doomsday:
“That “best estimate” scenario also assumes that 35
percent of infections are asymptomatic, meaning the total number of
infections is more than 50 percent larger than the number of symptomatic
cases. It therefore implies that the IFR is between 0.2 percent and 0.3
percent. By contrast, the projections that the CDC made in March, which
predicted that
as many as 1.7 million Americans could die from COVID-19 without
intervention, assumed an IFR of 0.8 percent. Around the same time,
researchers at Imperial College produced a worst-case scenario in which 2.2 million Americans died, based on an IFR of 0.9 percent.”
In order to be as bullet-proof as possible, and because the IFR is an
important part of the math I will do right now, I’ve decided to pick a
simple and defensible number, the final number pegged by the CDC for COVID-19’s IFR: 0.26%
(As an aside, if we’d known this 3 months ago, no one in the public
health world would have panicked. It’s a bad flu, and the rates for
younger people are dramatically below 0.26% and approaching zero for
children.) Now that you understand COVID’s IFR and the likely HIT, it’s
much easier to talk about the second wave, the data, and the
implications. Here’s the deal:
“Yes, certain states are having an uptick in three
measurements: COVID-19 tests administered, positive COVID-19 tests, and
hospitalizations. All three of these measurements are dubious.
Hopefully, some of the rise in cases is REAL, because then the U.S. will
arrive at Herd Immunity Threshold (“HIT”), which has been slightly
delayed by lockdowns, sooner. Based on the “death curve” in the US, we
are very close to being done.”
Take population, COVID Deaths, and IFR to find HIT
C’mon stay with me! This math is basic, junior high level stuff. And,
it’s going to give us the most important, but very crude, number we
need to understand all this second wave nonsense: the approximate HIT
already attained by state and by the United States. If you know how many
people have died from COVID-19 in any one region, you can quickly
calculate how many people have had COVID-19 in that same region. All you
do is divide deaths by the IFR. Let’s use NY as the example. As of
today, there have been 31,137 deaths from COVID-19. Take 31,137/.0026,
you get 11,975,969 people infected with COVID-19. Take those 11 million
people divided by New York’s population of 19.45 million, you get a HIT
of…65%. (Data geek comment: New York’s HIT is clearly OVER-stated,
because total deaths drives HIT, and NY has a much higher rate of
nursing home deaths due to bad policy.) Huge disclaimer: This math is crude, but it’s also
directionally accurate, and the comparisons BETWEEN states helps explain
what’s going on. Importantly, the HIT required to snuff out the virus
in any one region could be lower than Sweden’s number of 17%, for a
million reasons, most notably better medical knowledge today than a few
months ago about how to keep a vulnerable person alive. Still, just look
at this table I created using the math above:
Notice anything? New York is WELL PAST Herd Immunity Threshold (as is
New Jersey), the southern states in the news are BELOW the implied HIT,
while the U.S. overall is nearly there with 15%. This is why the death
curve from the CDC (and NYC!) that I opened this blog post with looks
the way it looks: we are basically done with the virus. Just like Sweden. Oh, and Italy:
Quick update: Mount Sinai doctors just released a study
showing a seroprevalence study of a random sample of 5,000 New Yorkers,
it states that “by the week ending April 19, the seroprevalence in the
screening group reached 19.3%.” If you take that 19.3% number, and
consider what we just learned from Sweden—that half of people with
immunity won’t show it with this test—and then consider how many more
people have been exposed since April 28, it’s entirely plausible that NY
is well past 40% or more people, which starts to look
closer to the 65% number my math shows. Either way, let’s just keep it
simple: New York, and especially NYC, are WELL PAST HIT of 10-20%, which
explains why their death curve looks the way it looks.
Florida details
While HIT matters more than anything else in explaining the
trajectory of the virus, and tells us that the U.S. is very close to
being done with COVID-19, I wanted to take a closer look at one state,
Florida, the current whipping boy of the press. They also have great
data. No one seems to be listening to the Governor, the health
department, or the hospitals in Florida, who all seem to be saying the
same thing, which is basically that everything is fine. On June 20,
Florida’s department of health produced a presentation that explained
how their testing had changed over time. Check out this slide:
So, as the state re-opened, they began to test everyone, “regardless
of age and symptoms.” What do you think would happen when they did that?
Obviously, more positives. So, here’s my first fact: Fact #1: All of the “second wave” states have dramatically
increased their testing. This alone causes cases to rise, and is the
single biggest reason they have. Still not convinced? Check out this eye-opener of a chart that
shows per-capita testing in the U.S. versus other countries. Notice
anything about June? Not only do we do MORE testing than any other
country, but our testing spiked in June, right as all the headlines
about more cases came out. Hmmm…
It’s not quite that simple. Yes, cases are up because more testing is
being done. Cases have never, ever been a reliable indicator of
ANYTHING. But, hospitalizations have been a reliable indicator. And,
unexpectedly, there was an uptick in hospitalizations for COVID-19
beginning around June 6th in Florida, as you can see here:
Florida hospitalizations due to COVID-19 trend line.
The most obvious reason COVID-19 hospitalizations are going up is
because of what’s happening in the hospital system. Patients are
returning to the hospitals for elective surgery that were all delayed
during the lockdown. EVERY patient is screened for COVID-19. A patient
who is undergoing elective knee surgery and tests positive for COVID-19
even though they are asymptomatic will be classified as “hospitalized
with COVID-19.” This was explained in a recent NY Timesarticle:
“One-third of all patients admitted to the city’s
[Miami] main public hospital over the past two weeks after going to the
emergency room for car-crash injuries and other urgent problems have
tested positive for the coronavirus.”
Fact #2: Hospitalizations for COVID-19 are up slightly
because of how COVID-19 positive patients are tracked. They will be in
the number even if they didn’t go to the hospital BECAUSE of COVID-19. Still, there is something else going on. It’s not just more
tests and the way hospitalizations are happening. Many states re-opened
on May 1 and their trend lines were flat to down for weeks. It’s as if
some super-spreader event happened in certain states towards late
May/Early June. It’s really clear that something unique is going on if
you look at data from Minnesota, the state where George Floyd was
tragically murdered, where positive cased are stratified by age:
As you can see, in Minnesota, the percentage of positive cases by
people age 20-29 really spiked in mid to late June, which means
infections likely happened in early June or late May. Yes, obviously,
the densely-packed protests for racial equality and social justice—which
I personally applaud—appear to have caused a REAL uptick in cases and
hospitalizations. See this article, Houston Protesters Begin to Fall Ill With Coronavirus After Marching for George Floyd. Just look at the median age of NEW cases in Florida for mid-June (used to be in the mid-60s):
Fact #3: A REAL rise in both cases and hospitalizations
perfectly matches the timing of the nationwide protests which included
many densely-packed crowds together for many hours and even days. Not convinced? Check out this great graph that
overlays the timing of the protests, lockdowns, social mobility, and
hospitalizations using data for the entire US. Note there is a time
delay between exposure and hospitalizations (between 8 and 15 days), and
look at when the yellow hospitalization line goes up.
However, the good news about all of this is that there has been no
impact on the number of COVID-19 patients in ICUs, which is consistent
with the fact that we know younger patients are less impacted by
COVID-19, check out this chart:
Fact #4: Despite a small uptick in hospitalizations, the number of COVID-19 patients in the ICU continues to decline. IT’S DEATHS, NOT CASES
You’ve been hearing about a handful of states with rising cases, here they are on a chart, cases are clearly rising:
But for those states, what about deaths? They appear to be going the other way:
And, finally, perhaps the most important slide, using Florida as the
example, there is NO correlation between more tests, more positive
tests, and DEATHS (red line in the graph). The fact that these three
measures are not linear means Florida has a low and stable death rate,
and the recent uptick in positive cases—which happens to be perfectly
timed to the nationwide protests—means nothing: Fact #5: There is NO correlation in Florida—the state taking
the most heat in the press about a second wave—between positive tests
and deaths. Of course, anyone who has been paying attention to the data
could have told you that, because the national data on COVID-19 deaths
is looking more and more like Sweden’s, as we already discussed. Today,
our national HIT is roughly 15%, which means we are almost done, no
matter what any Governor does.
I’ve seen discussion about how the protests caused an uptick
in infections amongst younger people. Some in opposition to that fairly
obvious reality point to New York, which also had densely-packed
protests but has NOT seen an uptick in hospitalizations—how do you
explain that? By now, you know the answer: New York’s HIT is already 65%!
Notably, in the math I used, Florida only had a Herd
Immunity Threshold number of 6%, well below the target of 17%. So, yes,
they MAY WELL have to endure a few more deaths before they achieve HIT.
But, it’s highly likely that 1) it won’t need to be as high as 17%
because the people being infected are much younger (where death rate is
much lower) and 2) that it will happen in the next few weeks, and policy
will have nothing to do with whether it happens or not. Either way,
because we know the national number is 15%, the virus is almost gone, no
matter what anyone says or does, and all you need to do to verify that
is look at the CDC’s death curve.
A final thought about Florida: John Thomas Littell, MD is a family physician in Florida. I was going to publish an excerpt from his Letter to the Editor of the Orlando Medical News, but it’s so good and so wide-ranging, I want you to read the whole thing, and then we can wrap this up:
“Several times a day, on every possible news outlet,
we are bombarded with updates as to the new number of “cases” of
COVID-19 in the U.S. and elsewhere. News analysts then use these
numbers to justify criticisms of those who dare to reject the CDC’s
recommendations with regards to mask wearing and social distancing. It
is imperative that all Americans – and especially those in the medical
profession – understand the actual definition of a “case” of COVID -19
so as to make informed decisions as to how to live our lives. “Older Americans remember all too well the dread they experienced
when a family member was diagnosed with a “case” of scarlet fever,
diphtheria, whooping cough (pertussis), or polio. During my career in
family medicine, including several years as an Army physician, I have
cared for patients with chickenpox, shingles, Lyme disease as well as
measles, tuberculosis, malaria, and AIDS. The “case definition”
established for all of these diseases by the CDC requires the presence
of signs and symptoms of that disease. In other words, each case
involved a SICK patient. Laboratory studies may be performed to
“confirm” a diagnosis, but are not sufficient in the absence of clinical
symptoms. “Having now been privileged to care for sick patients with
COVID-19, both in and out of the hospital setting, I am happy to see the
number of these sick patients dwindle almost to zero in my community –
while the “case numbers” for COVID-19 continue to go up. Why is that? “In marked contrast to measles, shingles, and other infectious
disease, “cases” of COVID-19 do NOT require the presence of ANY symptoms
whatsoever. Health departments are encouraging everyone and anyone to
come in for testing, and each positive test is reported as yet another
“new” case of COVID-19! “On April 5, 2020, a small number of state epidemiologists
(Council of State and Territorial Epidemiologists (CSTE) Technical
Supplement: Interim-20-ID-01) came up with a “surveillance” case
definition for COVID-19. At the time, there was uncertainty as to
whether or not completely asymptomatic persons could transmit COVID-19
sufficiently enough to infect and cause disease in others. (This notion
has never been proven and, in fact, has recently been discounted – cfr “
A Study on the Infectivity of Asymptomatic SARS-CoV-2 Carriers, Ming
Fao et al, Respir Med, 2020 Aug – available online through PubMed 2020
May 13, as well as recent reports from the WHO itself). The CSTF
thereby justified the unconventional case definition for COVID-19,
adding ‘CSTE realizes that field investigations will involve
evaluations of persons with no symptoms and these individuals will need
to be counted as cases.’ “Hence, anyone who has a positive PCR test (the nasal swab, PCR
test for COVID Antigen or Nucleic Acid) or serological test (blood test
for antibodies –IgG and/or IgM) would be classified as a “case” – even
in the absence of symptoms. In our hospitals at this time, there are
hundreds of former nursing home residents sitting in “COVID” units who
are in their usual state of good health, banned from returning to their
former nursing home residences simply because they have TESTED Positive
for COVID-19 during mass testing programs in the nursing homes. “The presence of a positive lab test for COVID-19 in a person who
has never been sick is actually GOOD news for that person and for the
rest of us. The positive test indicates that this person has likely
mounted an adequate immune response to a small dose of COVID-19 to whom
he or she was exposed – naturally (hence, no need for a vaccine vs.
COVID-19). “It is important as well to understand that the presence of lab
testing is not the ONLY criterion that the the CDC uses to established a
diagnosis of COVID-19. The presence of only 1 or 2 flu-like symptoms
(fever,chills, cough, sore throat, shortness of breath) – in the
absence of another proven cause (e.g., influenza, bacterial pneumonia)
is SUFFICIENT to give a diagnosis of COVID-19 – as long as the patient
also meets certain “epidemiological linkage” criteria as follows: “In a person with clinically compatible symptoms, [a ‘case’
will be reported if that person had] one or more of the following
exposures in the 14 days before onset of symptoms: travel to or
residence in an area with sustained, ongoing community transmission of
SARS-CoV-2; close contact (10 minutes or longer, within a 6 foot
distance) with a person diagnosed with COVID-19; or member of a risk
cohort as defined by public health authorities during an outbreak.”
Note that the definition of a “risk cohort” includes age > 70 or
living in a nursing home or similar facility. “So, in essence, any person with an influenza- like illness (ILI)
could be considered a “case” of COVID-19, even WITHOUT confirmatory
lab testing. The CDC has even advised to consider any deaths from
pneumonia or ILI as “Covid-related” deaths – unless the physician or
medical examiner establishes another infectious agent as the cause of
illness. “Now perhaps you see why the increasing number of cases, and even
deaths, due to COVID-19 is fraught with misinterpretation and is NOT in
any way a measure of the ACTUAL morbidity and mortality FROM
COVID-19. My patients who insist upon wearing masks, gloves and social
distancing are citing these misleading statistics as justification for
their decisions (and, of course, that they are following the ‘CDC
guidelines’). I simply advise them, ‘COVID-19 is NOT in the atmosphere
around us; it resides in the respiratory tracts of infected individuals
and can only be transmitted to others by sick, infected persons after
prolonged contact with others’. “So you may ask – why are we continuing to report increasing
numbers of cases of COVID as though it were BAD news for America? Rather
than as GOOD news, i.e, that the thousands of healthy Americans testing
positive (also known as “asymptomatic”) are indicative of the
presence of herd immunity – protecting themselves and many of us from
potential future assaults by variants of COVID? “Why did we as a society stop sending our children to schools and
camps and sports activities? Why did we stop going to work and church
and public parks and beaches? Why did we insist that healthy persons
“stay at home” – rather than observing the evidence-based, medically
prudent method of identifying those who were sick and isolating them
from the rest of the population – advising the sick to “stay at home”
and allowing the rest of society to function normally? And, while we
witnessed the gatherings of protestors in recent days with little
concerns for COVID-19 spread among these asymptomatic persons, most
certainly many are hoping that the increasing “case” numbers for
COVID-19 will discourage folks from coming to any more rallies for
certain candidates for political office. “Fear is a powerful weapon. FDR famously broadcast to Americans
in 1933 that “We have nothing to fear, but fear itself”. I would argue
that we have to fear those who would have us remain fearful and servile
and willing to surrender basic freedoms without justification.” *John Thomas Littell, MD, is a board-certified family physician.
After earning his MD from George Washington University, he served in the
US Army, receiving the Meritorious Service Medal for his work in
quality improvement, and also served with the National Health Service
Corps in Montana. During his eighteen years in Kissimmee, FL, Dr Littell
has served on the faculty of the UCF School of Medicine, President of
the County Medical Society, and Chief of Staff at the Florida Hospital.
He currently resides with his wife, Kathleen, and family in Ocala,
Florida, where he remains very active as a family physician with
practices both in Kissimmee and Ocala.
Dr. Littell brings up many more issues than I have chosen to address in this post, because I already wrote about them in my previous blog post on May 30.
Wasn’t this supposed to be about hospitals?
The only reason ever given for locking down in the first
place was space availability in hospitals. Here’s what Florida said
about their hospitals last week:
And here’s what doctors in Houston, Texas said last week:
“Hospital CEO’s including, Dr. Marc Boom with Houston Methodist, Dr. David L. Callender with Memorial Hermann Health System, Dr. Doug Lawson with St. Luke’s Health, and Mark A. Wallace with Texas Children’s Hospital,
held a zoom conference, June 25, out of concern, “that recent news
coverage has unnecessarily alarmed the Houston community about hospital
capacity during this COVID-19 surge.” The two key major takeaways from
today’s discussion: The Houston health care system has the resources and
capacity necessary to treat patients with COVID-19 and otherwise…”
Sigh. So why is the press making such a big deal out of the “second wave”? I don’t do politics, but if I did I would probably mention that here.
What are Governors doing?
In a quick word: nothing helpful. I think this guy summarizes how I feel:
Seriously, though, the rollbacks of openings are simply ridiculous,
and simply compounding a terrible idea, and delaying the inevitable
process within each region of achieving a proper Herd Immunity
Threshold. If you want to get angry about lockdowns all over again, like
I did in my article in May, just read this: The lockdown is causing so many deaths. Here’s an excerpt:
“How many people aged 15 or under have died of
Covid-19? Four. The chance of dying from a lightning strike is one in
700,000. The chance of dying of Covid-19 in that age group is one in 3.5
million. And we locked them all down. Even among the 15- to
44-year-olds, the death rate is very low and the vast majority of deaths
have been people who had significant underlying health conditions. We
locked them down as well. We locked down the population that had
virtually zero risk of getting any serious problems from the disease,
and then spread it wildly among the highly vulnerable age group. If you
had written a plan for making a complete bollocks of things you would
have come up with this one.”
In Conclusion
Dr. Michael Levitt and Sweden have been right all along. The only way
through COVID-19 is by achieving the modest (10-20%) Herd Immunity
Threshold required to have the virus snuff itself out. The sooner
politicians—and the press—start talking about HIT and stop talking about
new confirmed cases, the better off we will all be. Either way, it’s
likely weeks, not months, before the data of new daily deaths will be so
low that the press will have to find something new to scare everyone.
It’s over. A quick note:
Haters of this article will post articles about Sweden saying their
approach has been a failure. They will point to recent press about
Sweden having higher rates of COVID-19 positive tests lately—Sweden has pushed back strongly—so here’s a chart for the haters, it shows positive cases in Sweden, tracked against deaths. There’s no correlation.
For my truly committed readers who made it this far:
“The death rate is a fact; anything beyond this is an inference.”
—William Farr (1807 – 1883)
William Farr, creator of Farr’s law, knew
this over 100 years ago. Viruses rise and fall at roughly the same
slopes. It’s predictable, and COVID-19 is no different, which is why,
after looking at all these death curves, it’s not very hard to declare
that the pandemic is over. Oxford’s center for Evidence Based Medicine
has a wonderful explanation of Farr’s law, and it’s well worth a read. Some of my favorite quotes:
“Farr shows us that once peak infection has been reached
then it will roughly follow the same symmetrical pattern on the
downward slope.”
“In the midst of a pandemic, it is easy to forget Farr’s
Law, and think the number infected will just keep rising, it will not.
Just as quick as measures were introduced to prevent the spread of
infection we need to recognise the point at which to open up society and
also the special measures due to ‘density’ that require special
considerations.”
“Once peak deaths have been reached we should
be working on the assumption that the infection has already started
falling in the same progressive steps. Using deaths as the proxy for
falling infections facilitates the planning of the next steps for
reopening those societies that are in lockdown.”
A reader just sent me this chart from the CDC. If you don’t think the
COVID-19 virus has run its course according to Farr’s Law, I can’t help
you!
About the author: J.B. Handley is the best-selling author of How to End the Autism Epidemic. He graduated with honors from Stanford University, and currently serves as a Managing member of Bochi Investments, a private investment firm. He can be reached at jbhandleyblog@gmail.com
Sign up
for free news and updates from Robert F. Kennedy, Jr. and the
Children’s Health Defense. CHD is planning many strategies, including
legal, in an effort to defend the health of our children and obtain
justice for those already injured. Your support is essential to CHD’s successful mission.



“However, it does provide a possible explanation for why the Covid-19 epidemic seems to have died away in many places once it had infected around 20 percent of the local population (as judged by the presence of antibodies). If people are developing some kind of immunity to Covid-19 via their T cells then it could mean that a far higher percentage of the population has been exposed to Covid-19 than previously thought. Antibodies and T cells combined, it is conceivable that some places such as London or New York are already at or near the 60 per cent infection level required to achieve herd immunity.”

















No comments:
Post a Comment