On the Trail of the Elusive X-Factor: A
Sixty-Two-Year-Old Mystery Finally Solved
Posted on
February 14, 2008 by Christopher
Masterjohn • 3
Comments
Contents
- Article Summary
- On the Trail of the Elusive X-Factor (Main Article)
- A Sixty-Year Mystery
- Vitamin K: Three Discoveries Converge
- Perfect Correspondence
- Synergy with Vitamins A and D
- Vitamin K2 and Dental Health
- Vitamin K2 and Bone Health
- Vitamin K2 and Heart Disease
- Vitamin K2 and the Brain
- Other Roles of Vitamin K2
- Vitamin K2 in Foods
- Figures
- Figure 1: The Structure of K Vitamins and Their Chemical Behavior
- Figure 2: Corresponding Characteristics of Activator X and Vitamin K2
- Figure 3: Vitamin K-Dependent Carboxylation
- Figure 4: Vitamin K2 Contents of Selected Foods
- Sidebars
- The Activator X Test
- Interactions between Vitamins A, D, and K2
- Is Vitamin K2 an Essential Nutrient?
- The Vitamin K-Dependent Carboxylase
- Vitamin K2 and the Brain: A Closer Look
- Bacterial Production of Vitamin K2
- Supplementing with Vitamin K2
- References
- Follow Up Questions & Answers
|
In
1945, Dr. Weston Price described “a new vitamin-like activator” that played
an influential role in the utilization of minerals, protection from tooth
decay, growth and development, reproduction, protection against heart disease
and the function of the brain.Using a chemical test, he determined that this
compound—which he called Activator X—occurred in the butterfat, organs and
fat of animals consuming rapidly growing green grass, and also in certain sea
foods such as fish eggs.Dr. Price died before research by Russian scientists
became known in the West. These scientists used the same chemical test to
measure a compound similar to vitamin K.Vitamin K2 is produced by
animal tissues, including the mammary glands, from vitamin K1, which
occurs in rapidly growing green plants.A growing body of published research
confirms Dr. Price’s discoveries, namely that vitamin K2 is
important for the utilization of minerals, protects against tooth decay,
supports growth and development, is involved in normal reproduction, protects
against calcification of the arteries leading to heart disease, and is a
major component of the brain.Vitamin K2 works synergistically with
the two other “fat-soluble activators” that Price studied, vitamins A and D.
Vitamins A and D signal to the cells to produce certain proteins and vitamin
K then activates these proteins.Vitamin K2 plays a crucial role in
the development of the facial bones, and its presence in the diets of
nonindustrialized peoples explains the wide facial structure and freedom from
dental deformities that Weston Price observed.
|
Main Article (On the Trail of the Elusive X-Factor)
Read in: Czech
In 1945, Weston Price published a second edition of his pioneering work Nutrition and Physical Degeneration, to which he added a new chapter entitled, “A New Vitamin-Like Activator.”1 In it, he presented evidence of a theretofore unrecognized fat-soluble substance that played a fundamental role in the utilization of minerals and whose absence from modern nutrition was responsible for the proliferation of dental caries and other degenerative diseases. Although Price quantified the relative amount of this substance in thousands of samples of dairy products sent to him from around the world, he never determined its precise chemical identity. For want of a better means of identification, he referred to it as “Activator X,” also sometimes referred to as the “Price Factor.”
Price found the highest concentrations of this nutrient in “the milk of several species, varying with the nutrition of the animal” and found the combination of cod liver oil and high-Activator X butter to be superior to that of cod liver oil alone. In the many butter samples he tested, Activator X was only present when the animals were eating rapidly growing green grass. In most regions, this occurred in the spring and early fall.
https://www.blogger.com/null
In 1945, Weston Price published a second edition of his pioneering work Nutrition and Physical Degeneration, to which he added a new chapter entitled, “A New Vitamin-Like Activator.”1 In it, he presented evidence of a theretofore unrecognized fat-soluble substance that played a fundamental role in the utilization of minerals and whose absence from modern nutrition was responsible for the proliferation of dental caries and other degenerative diseases. Although Price quantified the relative amount of this substance in thousands of samples of dairy products sent to him from around the world, he never determined its precise chemical identity. For want of a better means of identification, he referred to it as “Activator X,” also sometimes referred to as the “Price Factor.”
Price found the highest concentrations of this nutrient in “the milk of several species, varying with the nutrition of the animal” and found the combination of cod liver oil and high-Activator X butter to be superior to that of cod liver oil alone. In the many butter samples he tested, Activator X was only present when the animals were eating rapidly growing green grass. In most regions, this occurred in the spring and early fall.
https://www.blogger.com/null
A Sixty-Year Mystery
For over
sixty years, all attempts to identify this elusive “X” factor have failed. In
the 1940s, Dr. Royal Lee, founder of the whole food supplement company Standard
Process, suggested that activator X was the essential fatty acids.2
In 1980, Dr. Jeffrey Bland suggested more specifically that it was the
elongated omega-3 essential fatty acid called EPA.3 Although these
fatty acids exert some effects on calcium metabolism,4 neither the
distribution of these unsaturated fatty acids in foods nor their chemical
behavior corresponds to that of Activator X. Cod liver oil is much richer than
butter in essential fatty acids including EPA, and the oils of plant seeds are
even richer in these fats, but Price found little, if any, Activator X in these
foods. Moreover, Price tested for Activator X by quantifying the ability of a
food to oxidize iodide to iodine; essential fatty acids, however, do not
possess this chemical ability.
In 1982, one author wrote to the Price-Pottenger Nutrition Foundation that after pursuing a number of false leads while attempting to identify the X factor, he had concluded that the “peculiar behavior” observed in Price’s chemical test might be due to a “special kind of oxygen-containing heterocyclic ring,” and suggested a compound called 6-methoxybenzoxazolinone (MBOA) as a likely candidate.5 Although researchers first identified MBOA as an antifungal agent found in corn,6 later studies showed that it was found in many other plant foods and acted as a reproductive stimulant in some animals by mimicking the hormone melatonin.7 Although it is present in young, rapidly growing grass, no research has ever established MBOA as an essential nutrient, attributed to it any of the physiological roles of Activator X, or demonstrated its presence in the foods that Price considered to be the richest sources of this nutrient. MBOA, then, was just another false lead; we will soon see, however, that the writer’s observations about the chemical nature of Activator X were largely correct.
https://www.blogger.com/null
In 1982, one author wrote to the Price-Pottenger Nutrition Foundation that after pursuing a number of false leads while attempting to identify the X factor, he had concluded that the “peculiar behavior” observed in Price’s chemical test might be due to a “special kind of oxygen-containing heterocyclic ring,” and suggested a compound called 6-methoxybenzoxazolinone (MBOA) as a likely candidate.5 Although researchers first identified MBOA as an antifungal agent found in corn,6 later studies showed that it was found in many other plant foods and acted as a reproductive stimulant in some animals by mimicking the hormone melatonin.7 Although it is present in young, rapidly growing grass, no research has ever established MBOA as an essential nutrient, attributed to it any of the physiological roles of Activator X, or demonstrated its presence in the foods that Price considered to be the richest sources of this nutrient. MBOA, then, was just another false lead; we will soon see, however, that the writer’s observations about the chemical nature of Activator X were largely correct.
https://www.blogger.com/null
Vitamin K: Three Discoveries Converge
The test
that Price used for Activator X, called iodometric determination, was
traditionally regarded within the English language literature as a test for
peroxides (carbon-containing molecules that have been damaged by oxygen).8,9
Since peroxides do not have any activity as vitamins, the relationship between
the test and any nutritional substance remained a mystery. Although researchers
publishing in other languages were using the test to detect a class of
chemicals called quinones at least as far back as 1910,10 it was not
until 1972 that Danish researchers published a paper in the British Journal of Nutrition showing that the test could be used
to detect biological quinones such as K vitamins in animal tissues.12
K vitamins (Figure 1) possess oxygen-containing ring structures that are capable of oxidizing iodide to iodine and would therefore be detected by Price’s Activator X test. The K vitamins are likely to go down in history as the most misunderstood group of vitamins of the twentieth century. In many ways, however, modern researchers are now rediscovering properties of these vitamins that Price had discovered over sixty years ago. It has now become clear that both Activator X and its precursor in rapidly growing grass are both members of this group.
There are two natural forms of vitamin K: vitamin K1 and vitamin K2. Vitamin K1, also called phylloquinone, is found in the green tissues of plants, tightly embedded within the membrane of the photosynthesizing organelle called the chloroplast. As the chlorophyll within this organelle absorbs energy from sunlight, it releases high-energy electrons; vitamin K1 forms a bridge between chlorophyll and several iron-sulfur centers across which these electrons travel, releasing their energy so that the cell can ultimately use it to synthesize glucose.13
When animals consume vitamin K1, their tissues convert part of it into vitamin K2,14 which fulfills a host of physiological functions in the animal that we are only now beginning to understand. The ability to make this conversion varies widely not only between species14 but even between strains of laboratory rats,15,16 and has not been determined in humans. The mammary glands appear to be especially efficient at making this conversion, presumably because vitamin K2 is essential for the growing infant.17 Vitamin K2 is also produced by lactic acid bacteria,18 although bacteria produce forms of the vitamin that are chemically different from those that animals produce, and researchers have not yet established the differences in biological activity between these forms.
Although both K vitamins were discovered and characterized over the course of the 1930s, two fundamental misunderstandings about these vitamins persisted for over sixty years: the medical and nutritional communities considered blood clotting to be their only role in the body, and considered vitamins K1 and K2 to simply be different forms of the same vitamin. The first vitamin K-dependent protein relating to skeletal metabolism was not discovered until 1978. It was not until 1997, nearly twenty years later, that the recognition that vitamin K was “not just for clotting anymore” broke out of the confines of the fundamental vitamin K research community.19
Since the amount of vitamin K1 in typical diets is ten times greater than that of vitamin K2,20 researchers have tended to dismiss the contribution of K2 to nutritional status as insignificant. Yet over the last few years, a growing body of research is demonstrating that these two substances are not simply different forms of the same vitamin, but are better seen as two different vitamins: whereas K1 is preferentially used by the liver to activate blood clotting proteins, K2 is preferentially used by the other tissues to place calcium where it belongs, in the bones and teeth, and keep it out of where it does not belong, in the soft tissues.21 Acknowledging this research, the United States Department of Agriculture, in conjunction with researchers from Tufts University, finally determined the vitamin K2 contents of foods in the U.S. diet for the first time in 2006.22
https://www.blogger.com/null
K vitamins (Figure 1) possess oxygen-containing ring structures that are capable of oxidizing iodide to iodine and would therefore be detected by Price’s Activator X test. The K vitamins are likely to go down in history as the most misunderstood group of vitamins of the twentieth century. In many ways, however, modern researchers are now rediscovering properties of these vitamins that Price had discovered over sixty years ago. It has now become clear that both Activator X and its precursor in rapidly growing grass are both members of this group.
There are two natural forms of vitamin K: vitamin K1 and vitamin K2. Vitamin K1, also called phylloquinone, is found in the green tissues of plants, tightly embedded within the membrane of the photosynthesizing organelle called the chloroplast. As the chlorophyll within this organelle absorbs energy from sunlight, it releases high-energy electrons; vitamin K1 forms a bridge between chlorophyll and several iron-sulfur centers across which these electrons travel, releasing their energy so that the cell can ultimately use it to synthesize glucose.13
When animals consume vitamin K1, their tissues convert part of it into vitamin K2,14 which fulfills a host of physiological functions in the animal that we are only now beginning to understand. The ability to make this conversion varies widely not only between species14 but even between strains of laboratory rats,15,16 and has not been determined in humans. The mammary glands appear to be especially efficient at making this conversion, presumably because vitamin K2 is essential for the growing infant.17 Vitamin K2 is also produced by lactic acid bacteria,18 although bacteria produce forms of the vitamin that are chemically different from those that animals produce, and researchers have not yet established the differences in biological activity between these forms.
Although both K vitamins were discovered and characterized over the course of the 1930s, two fundamental misunderstandings about these vitamins persisted for over sixty years: the medical and nutritional communities considered blood clotting to be their only role in the body, and considered vitamins K1 and K2 to simply be different forms of the same vitamin. The first vitamin K-dependent protein relating to skeletal metabolism was not discovered until 1978. It was not until 1997, nearly twenty years later, that the recognition that vitamin K was “not just for clotting anymore” broke out of the confines of the fundamental vitamin K research community.19
Since the amount of vitamin K1 in typical diets is ten times greater than that of vitamin K2,20 researchers have tended to dismiss the contribution of K2 to nutritional status as insignificant. Yet over the last few years, a growing body of research is demonstrating that these two substances are not simply different forms of the same vitamin, but are better seen as two different vitamins: whereas K1 is preferentially used by the liver to activate blood clotting proteins, K2 is preferentially used by the other tissues to place calcium where it belongs, in the bones and teeth, and keep it out of where it does not belong, in the soft tissues.21 Acknowledging this research, the United States Department of Agriculture, in conjunction with researchers from Tufts University, finally determined the vitamin K2 contents of foods in the U.S. diet for the first time in 2006.22
https://www.blogger.com/null
Perfect Correspondence
Because
vitamin K1 is directly associated with both chlorophyll and
beta-carotene within a single protein complex and plays a direct role in
photosynthesis,13 the richness of the green color of grass, its rate
of growth, and its brix rating (which measures the density of organic material
produced by the plant) all directly indicate its concentration of vitamin K1.
Animals grazing on grass will accumulate vitamin K2 in their tissues
in direct proportion to the amount of vitamin K1 in their diet. The
beta-carotene associated with vitamin K1 will also impart a yellow
or orange color to butterfat; the richness of this color therefore indirectly
indicates the amount of both vitamins K1 and K2 in the
butter. Not only are the K vitamins detected by the Activator X test and distributed
in the food supply precisely as Price suggested, but, as shown in Figure
2, the physiological actions that Price attributed to Activator X
correspond perfectly to those of vitamin K2. It is therefore clear
that the precursor to Activator X found in rapidly growing, green grass is none
other than vitamin K1, while Activator X itself is none other than
vitamin K2.
Ironically, Price discovered the roles of vitamin K2 in calcium metabolism, the nervous system and the cardiovascular system more than sixty years before the vitamin K research community began elucidating these roles itself, while vitamin K researchers discovered the chemical structure of activator X several years before Price even proposed its existence. Had Price been aware that his chemical test had been used for decades outside of the English language scientific community to detect quinones, a class to which the K vitamins belong, the two independent discoveries of this one vitamin may have converged sooner.
Instead, English-speaking researchers continued for decades to labor under the illusion that the iodometric method detected only peroxides; by the time this illusion was corrected, better methods for detecting peroxides had already been developed, Activator X had been forgotten, and the opportunity to make the connection between these three discoveries was lost. The twenty-first century, however, is already making radical revisions to our understanding of the K vitamins, which now make it clearer than ever that Activator X and vitamin K2 are one and the same.
https://www.blogger.com/null
Ironically, Price discovered the roles of vitamin K2 in calcium metabolism, the nervous system and the cardiovascular system more than sixty years before the vitamin K research community began elucidating these roles itself, while vitamin K researchers discovered the chemical structure of activator X several years before Price even proposed its existence. Had Price been aware that his chemical test had been used for decades outside of the English language scientific community to detect quinones, a class to which the K vitamins belong, the two independent discoveries of this one vitamin may have converged sooner.
Instead, English-speaking researchers continued for decades to labor under the illusion that the iodometric method detected only peroxides; by the time this illusion was corrected, better methods for detecting peroxides had already been developed, Activator X had been forgotten, and the opportunity to make the connection between these three discoveries was lost. The twenty-first century, however, is already making radical revisions to our understanding of the K vitamins, which now make it clearer than ever that Activator X and vitamin K2 are one and the same.
https://www.blogger.com/null
Synergy with Vitamins A and D
Price
showed Activator X to exhibit dramatic synergy with vitamins A and D. Chickens
voluntarily consumed more butter and died more slowly on a deficiency diet when
the butter was high in both vitamin A and Activator X than when it was high in
vitamin A alone. Cod liver oil, which is high in both vitamins A and D,
partially corrected growth retardation and weak legs in turkeys fed a
deficiency diet, but the combination of cod liver oil and high-Activator X
butter was twice as effective. Likewise, Price found that the combination of
cod liver oil and a high-Activator X butter oil concentrate was more effective
than cod liver oil alone in treating his patients for dental caries and other
signs of physical degeneration.
Vitamin K2 is the substance that makes the vitamin A- and vitamin D-dependent proteins come to life. While vitamins A and D act as signaling molecules, telling cells to make certain proteins, vitamin K2 activates these proteins by conferring upon them the physical ability to bind calcium. In some cases these proteins directly coordinate the movement or organization of calcium themselves; in other cases the calcium acts as a glue to hold the protein in a certain shape.33 In all such cases, the proteins are only functional once they have been activated by vitamin K.
Osteocalcin, for example, is a protein responsible for organizing the deposition of calcium and phosphorus salts in bones and teeth. Cells only produce this protein in the presence of both vitamins A and D;34 it will only accumulate in the extracellular matrix and facilitate the deposition of calcium salts, however, once it has been activated by vitamin K2.35 Vitamins A and D regulate the expression of matrix Gla protein (MGP),36,37 which is responsible for mineralizing bone and protecting the arteries from calcification; like osteocalcin, however, MGP can only fulfill its function once it has been activated by vitamin K2.33 While vitamins A and D contribute to growth by stimulating growth factors and promoting the absorption of minerals, vitamin K2 makes its own essential contribution to growth by preventing the premature calcification of the cartilaginous growth zones of bones.38
Vitamin K2 may also be required for the safety of vitamin D. The anorexia, lethargy, growth retardation, bone resorption, and soft tissue calcification that animals fed toxic doses of vitamin D exhibit bear a striking resemblance to the symptoms of deficiencies in vitamin K or vitamin K-dependent proteins. Warfarin, which inhibits the recycling of vitamin K, enhances vitamin D toxicity and exerts a similar type of toxicity itself. Similarly, the same compounds that inhibit the toxicity of Warfarin also inhibit the toxicity of vitamin D. I have therefore hypothesized elsewhere that vitamin D toxicity is actually a relative deficiency of vitamin K2.39 The synergy with which vitamin K2 interacts with vitamins A and D is exactly the type of synergy that Price attributed to Activator X.
https://www.blogger.com/null
Vitamin K2 is the substance that makes the vitamin A- and vitamin D-dependent proteins come to life. While vitamins A and D act as signaling molecules, telling cells to make certain proteins, vitamin K2 activates these proteins by conferring upon them the physical ability to bind calcium. In some cases these proteins directly coordinate the movement or organization of calcium themselves; in other cases the calcium acts as a glue to hold the protein in a certain shape.33 In all such cases, the proteins are only functional once they have been activated by vitamin K.
Osteocalcin, for example, is a protein responsible for organizing the deposition of calcium and phosphorus salts in bones and teeth. Cells only produce this protein in the presence of both vitamins A and D;34 it will only accumulate in the extracellular matrix and facilitate the deposition of calcium salts, however, once it has been activated by vitamin K2.35 Vitamins A and D regulate the expression of matrix Gla protein (MGP),36,37 which is responsible for mineralizing bone and protecting the arteries from calcification; like osteocalcin, however, MGP can only fulfill its function once it has been activated by vitamin K2.33 While vitamins A and D contribute to growth by stimulating growth factors and promoting the absorption of minerals, vitamin K2 makes its own essential contribution to growth by preventing the premature calcification of the cartilaginous growth zones of bones.38
Vitamin K2 may also be required for the safety of vitamin D. The anorexia, lethargy, growth retardation, bone resorption, and soft tissue calcification that animals fed toxic doses of vitamin D exhibit bear a striking resemblance to the symptoms of deficiencies in vitamin K or vitamin K-dependent proteins. Warfarin, which inhibits the recycling of vitamin K, enhances vitamin D toxicity and exerts a similar type of toxicity itself. Similarly, the same compounds that inhibit the toxicity of Warfarin also inhibit the toxicity of vitamin D. I have therefore hypothesized elsewhere that vitamin D toxicity is actually a relative deficiency of vitamin K2.39 The synergy with which vitamin K2 interacts with vitamins A and D is exactly the type of synergy that Price attributed to Activator X.
https://www.blogger.com/null
Vitamin K2 and Dental Health
Weston
Price was primarily interested in Activator X because of its ability to control
dental caries. By studying the remains of human skeletons from past eras, he
estimated that there had been more dental caries in the preceding hundred years
than there had been in any previous thousand-year period and suggested that
Activator X was a key substance that people of the past obtained but that
modern nutrition did not adequately provide. Price used the combination of
high-vitamin cod liver oil and high-Activator X butter oil as the cornerstone
of his protocol for reversing dental caries. This protocol not only stopped the
progression of tooth decay, but completely reversed it without the need for oral
surgery by causing the dentin to grow and remineralize, sealing what were once
active caries with a glassy finish. One 14-year-old girl completely healed 42
open cavities in 24 teeth by taking capsules of the high-vitamin cod liver oil
and Activator X concentrate three times a day for seven months.
Activator X also influences the composition of saliva. Price found that if he collected the saliva of individuals immune to dental caries and shook it with powdered bone or tooth meal, phosphorus would move from the saliva to the powder; by contrast, if he conducted the same procedure with the saliva of individuals susceptible to dental caries, the phosphorus would move in the opposite direction from the powder to the saliva. Administration of the Activator X concentrate to his patients consistently changed the chemical behavior of their saliva from phosphorus-accepting to phosphorus-donating. The Activator X concentrate also reduced the bacterial count of their saliva. In a group of six patients, administration of the concentrate reduced the Lactobacillus acidophilus count from 323,000 to 15,000. In one individual, the combination of cod liver oil and Activator X concentrate reduced the L. acidophilus count from 680,000 to 0.
In the 1940s, researchers showed that menadione and related compounds inhibited the bacterial production of acids in isolated saliva.47 Menadione itself is a toxic synthetic analogue of vitamin K, but animal tissues are able to convert a portion of it to vitamin K2. The ability of vitamin K-related compounds to inhibit acid production in isolated saliva had no relationship to their vitamin activity, and the most effective of these compounds had practically no vitamin activity at all.48 Researchers unfortunately assumed that because vitamin K did not have a unique role in inhibiting acid formation in saliva within a test tube that it had no nutritional role in preventing tooth decay within living beings.
In 1945, American researchers conducted a double-blind, placebo-controlled trial of menadione-laced chewing gum and showed it to reduce the incidence of new cavities and cause a dramatic drop in the L. acidophilus count of saliva.49 The next year, the Army Medical Department attempted to repeat these results but failed, and research on vitamin K and dental health in the United States was subsequently abandoned.50 The authors of the original study assumed that the menadione exerted its effect simply as a topical anti-bacterial agent, even though it was highly unlikely to sustain a sufficient concentration in the saliva to exert this effect. Ten years later, German researchers showed that injecting menadione into the abdominal cavities of hamsters more effectively prevented tooth decay than feeding it orally.51 Although they could not rule out the possibility that some of this menadione was secreted into the saliva, their results argued in favor of a nutritional role for the vitamin K2 that would have been produced from it. Despite this finding, to this day no one has investigated the role of natural K vitamins in the prevention of dental caries.
Nevertheless, our continually expanding understanding of the physiology of both K vitamins and teeth now makes it clear that vitamin K2 plays an essential role in dental health. Of all organs in the body, vitamin K2 exists in the second highest concentration in the salivary glands (the highest concentration is found in the pancreas). Even when rats are fed only K1, nearly all of the vitamin K in their salivary glands exists as K2.15 Both vitamin K52 and vitamin K-dependent proteins53 are secreted into the saliva, although their function is unknown.
We now know that the growth and mineralization of the dentin that Price observed in response to the combination of cod liver oil and Activator X concentrate would primarily require three essential factors: vitamins A, D, and K2. There are three calcified tissues of the teeth: the cementum forms the roots, the enamel forms the surface, and the dentin forms the support structure beneath it. Cells called odontoblasts lining the surface of the pulp just beneath the dentin continually produce new dentin material. If a cavity invades the dentin and reaches these cells they can die. The pulp tissue, however, contains stem cells that can differentiate into new odontoblasts that could regenerate the lost dentin if the right conditions were present.54
Dentin is unique among the tissues of the teeth for its expression of osteocalcin, a vitamin K-dependent protein better known for its role in organizing the deposition of calcium and phosphorus salts in bone. In the infant rat, whose teeth grow very rapidly, dentin manufactures much more osteocalcin than bone does, suggesting that osteocalcin plays an important role in the growth of new dentin. Matrix Gla protein (MGP), which is required for the mineralization of bone, is also expressed in dentin.55 Vitamins A and D signal odontoblasts to produce osteocalcin,56,57 and probably regulate their expression of MGP as well. Only after vitamin K2 activates these proteins’ ability to bind calcium, however, can they lay down the mineral-rich matrix of dentin. The remarkable synergy between these three vitamins exactly mirrors the process Price observed.
https://www.blogger.com/null
Activator X also influences the composition of saliva. Price found that if he collected the saliva of individuals immune to dental caries and shook it with powdered bone or tooth meal, phosphorus would move from the saliva to the powder; by contrast, if he conducted the same procedure with the saliva of individuals susceptible to dental caries, the phosphorus would move in the opposite direction from the powder to the saliva. Administration of the Activator X concentrate to his patients consistently changed the chemical behavior of their saliva from phosphorus-accepting to phosphorus-donating. The Activator X concentrate also reduced the bacterial count of their saliva. In a group of six patients, administration of the concentrate reduced the Lactobacillus acidophilus count from 323,000 to 15,000. In one individual, the combination of cod liver oil and Activator X concentrate reduced the L. acidophilus count from 680,000 to 0.
In the 1940s, researchers showed that menadione and related compounds inhibited the bacterial production of acids in isolated saliva.47 Menadione itself is a toxic synthetic analogue of vitamin K, but animal tissues are able to convert a portion of it to vitamin K2. The ability of vitamin K-related compounds to inhibit acid production in isolated saliva had no relationship to their vitamin activity, and the most effective of these compounds had practically no vitamin activity at all.48 Researchers unfortunately assumed that because vitamin K did not have a unique role in inhibiting acid formation in saliva within a test tube that it had no nutritional role in preventing tooth decay within living beings.
In 1945, American researchers conducted a double-blind, placebo-controlled trial of menadione-laced chewing gum and showed it to reduce the incidence of new cavities and cause a dramatic drop in the L. acidophilus count of saliva.49 The next year, the Army Medical Department attempted to repeat these results but failed, and research on vitamin K and dental health in the United States was subsequently abandoned.50 The authors of the original study assumed that the menadione exerted its effect simply as a topical anti-bacterial agent, even though it was highly unlikely to sustain a sufficient concentration in the saliva to exert this effect. Ten years later, German researchers showed that injecting menadione into the abdominal cavities of hamsters more effectively prevented tooth decay than feeding it orally.51 Although they could not rule out the possibility that some of this menadione was secreted into the saliva, their results argued in favor of a nutritional role for the vitamin K2 that would have been produced from it. Despite this finding, to this day no one has investigated the role of natural K vitamins in the prevention of dental caries.
Nevertheless, our continually expanding understanding of the physiology of both K vitamins and teeth now makes it clear that vitamin K2 plays an essential role in dental health. Of all organs in the body, vitamin K2 exists in the second highest concentration in the salivary glands (the highest concentration is found in the pancreas). Even when rats are fed only K1, nearly all of the vitamin K in their salivary glands exists as K2.15 Both vitamin K52 and vitamin K-dependent proteins53 are secreted into the saliva, although their function is unknown.
We now know that the growth and mineralization of the dentin that Price observed in response to the combination of cod liver oil and Activator X concentrate would primarily require three essential factors: vitamins A, D, and K2. There are three calcified tissues of the teeth: the cementum forms the roots, the enamel forms the surface, and the dentin forms the support structure beneath it. Cells called odontoblasts lining the surface of the pulp just beneath the dentin continually produce new dentin material. If a cavity invades the dentin and reaches these cells they can die. The pulp tissue, however, contains stem cells that can differentiate into new odontoblasts that could regenerate the lost dentin if the right conditions were present.54
Dentin is unique among the tissues of the teeth for its expression of osteocalcin, a vitamin K-dependent protein better known for its role in organizing the deposition of calcium and phosphorus salts in bone. In the infant rat, whose teeth grow very rapidly, dentin manufactures much more osteocalcin than bone does, suggesting that osteocalcin plays an important role in the growth of new dentin. Matrix Gla protein (MGP), which is required for the mineralization of bone, is also expressed in dentin.55 Vitamins A and D signal odontoblasts to produce osteocalcin,56,57 and probably regulate their expression of MGP as well. Only after vitamin K2 activates these proteins’ ability to bind calcium, however, can they lay down the mineral-rich matrix of dentin. The remarkable synergy between these three vitamins exactly mirrors the process Price observed.
https://www.blogger.com/null
Vitamin K2 and Bone Health
Price also
believed that Activator X played an important role in bone health. Butter oil
concentrate cured rickets and increased serum levels of calcium and phosphorus
in rats consuming a mineral-deficient diet. In a four-year-old boy who suffered
from rampant tooth decay, seizures and a tendency to fracture, the combination
of a large helping of this concentrate and a meal of whole wheat and whole milk
rapidly resolved each of these symptoms.
Although the small amount of vitamin D in the butter oil was probably sufficient to cure rickets and the combination of vitamins A and D most likely produced the rise in serum calcium and phosphorus,58 vitamin K2 has a definite role in bone health. There are at least two vitamin K-dependent proteins that fulfill important functions in skeletal metabolism: matrix Gla protein (MGP) and osteocalcin.
In 1997, researchers from the University of Texas and the University of Montreal developed mice that lacked the gene that codes for MGP. These mice appeared normal for the first two weeks of their lives, after which they developed faster heart beats, stopped growing and died within two months with the rupture of their heavily calcified aortas. The disorganization of their cartilage cells not only produced short stature, but also produced osteopenia and spontaneous fractures.38
The bones of mice that lack the osteocalcin gene mineralize just as well as those of mice that do not lack the gene, but the mineral deposits are organized differently. This could mean that osteocalcin is important to the functional quality of bone and the ability to regulate its shape.59 Isolated human osteoblasts, the cells that lay down the calcified matrix of bone, secrete osteocalcin in response to vitamins A and D.34 The protein-rich matrix surrounding these cells will only accumulate this osteocalcin, however, if it is activated by vitamin K2. Calcification of the extracellular matrix occurs in parallel with the accumulation of osteocalcin, but it is not clear whether this protein plays a direct role in laying down the calcium salts or if its accumulation simply reflects the higher amount of vitamin K2 that is available to activate other proteins involved more directly in mineralization such as MGP.35
When there is an insufficient amount of vitamin K to keep up with the production of vitamin K-dependent proteins, many of these proteins are secreted into the blood in an inactive form. Circulating cells then take up these useless proteins and destroy them.40 By drawing a person’s blood and testing the percentages of circulating osteocalcin that are active and inactive, we can determine whether that person’s bone cells have enough vitamin K to meet their needs. People with the highest percentages of inactive osteocalcin are at a more than five-fold increased risk of hip fracture,60 confirming the value of the test.
By using this test, we can also show that vitamin K2 is the preferred K vitamin of the bones. It takes one milligram per day of a highly absorbable pharmacological preparation of vitamin K1 to maximally activate osteocalcin in human subjects;28 it appears, however, that humans are not capable of absorbing much more than one fifth this amount from whole foods.24 By contrast, large amounts of vitamin K2 are readily absorbed from foods.26 Even when using highly absorbable forms of these vitamins, vitamin K2 is much more effective. Researchers from the University of Maastricht in the Netherlands recently showed that over the course of 40 days, vitamin K2 was three times more effective than vitamin K1 at raising the percentage of activated osteocalcin. Moreover, the effect of vitamin K1 reached a plateau after just three days, whereas the effect of vitamin K2 increased throughout the entire study. Had it lasted longer, the study may have shown an even greater superiority of vitamin K2.32
We can therefore regard the percentage of inactive osteocalcin primarily as a marker for vitamin K2 status. In the healthy adult population, one hundred percent of the vitamin K-dependent blood coagulants produced by the liver are in their active form. By contrast, in this same population between ten and thirty percent of circulating osteocalcin is in its inactive form. Researchers rarely encounter individuals whose osteocalcin is fully activated.31 This suggests that vitamin K2 deficiency is universal, and that variation in K2 status within the population simply reflects varying degrees of deficiency.
Vitamin K1 supplements produce modest decreases in bone loss in the elderly. A number of Japanese trials, on the other hand, have shown that vitamin K2 completely reverses bone loss and in some cases even increases bone mass in populations with osteoporosis.31 The pooled results of seven Japanese trials show that vitamin K2 supplementation produces a 60 percent reduction in vertebral fractures and an 80 percent reduction in hip and other non-vertebral fractures.61 These studies used extremely high amounts of vitamin K2 and did not observe any adverse effects over the course of several years. Since they used such high doses of K2, however, and no studies have tested lower doses, they do not constitute definitive proof that the vitamin activity rather than some drug-like action unique to the high dose produced such dramatic results. The balance of the evidence, however, suggests that vitamin K2 is essential to skeletal health and that it is a key substance that modern diets do not adequately provide.
https://www.blogger.com/null
Although the small amount of vitamin D in the butter oil was probably sufficient to cure rickets and the combination of vitamins A and D most likely produced the rise in serum calcium and phosphorus,58 vitamin K2 has a definite role in bone health. There are at least two vitamin K-dependent proteins that fulfill important functions in skeletal metabolism: matrix Gla protein (MGP) and osteocalcin.
In 1997, researchers from the University of Texas and the University of Montreal developed mice that lacked the gene that codes for MGP. These mice appeared normal for the first two weeks of their lives, after which they developed faster heart beats, stopped growing and died within two months with the rupture of their heavily calcified aortas. The disorganization of their cartilage cells not only produced short stature, but also produced osteopenia and spontaneous fractures.38
The bones of mice that lack the osteocalcin gene mineralize just as well as those of mice that do not lack the gene, but the mineral deposits are organized differently. This could mean that osteocalcin is important to the functional quality of bone and the ability to regulate its shape.59 Isolated human osteoblasts, the cells that lay down the calcified matrix of bone, secrete osteocalcin in response to vitamins A and D.34 The protein-rich matrix surrounding these cells will only accumulate this osteocalcin, however, if it is activated by vitamin K2. Calcification of the extracellular matrix occurs in parallel with the accumulation of osteocalcin, but it is not clear whether this protein plays a direct role in laying down the calcium salts or if its accumulation simply reflects the higher amount of vitamin K2 that is available to activate other proteins involved more directly in mineralization such as MGP.35
When there is an insufficient amount of vitamin K to keep up with the production of vitamin K-dependent proteins, many of these proteins are secreted into the blood in an inactive form. Circulating cells then take up these useless proteins and destroy them.40 By drawing a person’s blood and testing the percentages of circulating osteocalcin that are active and inactive, we can determine whether that person’s bone cells have enough vitamin K to meet their needs. People with the highest percentages of inactive osteocalcin are at a more than five-fold increased risk of hip fracture,60 confirming the value of the test.
By using this test, we can also show that vitamin K2 is the preferred K vitamin of the bones. It takes one milligram per day of a highly absorbable pharmacological preparation of vitamin K1 to maximally activate osteocalcin in human subjects;28 it appears, however, that humans are not capable of absorbing much more than one fifth this amount from whole foods.24 By contrast, large amounts of vitamin K2 are readily absorbed from foods.26 Even when using highly absorbable forms of these vitamins, vitamin K2 is much more effective. Researchers from the University of Maastricht in the Netherlands recently showed that over the course of 40 days, vitamin K2 was three times more effective than vitamin K1 at raising the percentage of activated osteocalcin. Moreover, the effect of vitamin K1 reached a plateau after just three days, whereas the effect of vitamin K2 increased throughout the entire study. Had it lasted longer, the study may have shown an even greater superiority of vitamin K2.32
We can therefore regard the percentage of inactive osteocalcin primarily as a marker for vitamin K2 status. In the healthy adult population, one hundred percent of the vitamin K-dependent blood coagulants produced by the liver are in their active form. By contrast, in this same population between ten and thirty percent of circulating osteocalcin is in its inactive form. Researchers rarely encounter individuals whose osteocalcin is fully activated.31 This suggests that vitamin K2 deficiency is universal, and that variation in K2 status within the population simply reflects varying degrees of deficiency.
Vitamin K1 supplements produce modest decreases in bone loss in the elderly. A number of Japanese trials, on the other hand, have shown that vitamin K2 completely reverses bone loss and in some cases even increases bone mass in populations with osteoporosis.31 The pooled results of seven Japanese trials show that vitamin K2 supplementation produces a 60 percent reduction in vertebral fractures and an 80 percent reduction in hip and other non-vertebral fractures.61 These studies used extremely high amounts of vitamin K2 and did not observe any adverse effects over the course of several years. Since they used such high doses of K2, however, and no studies have tested lower doses, they do not constitute definitive proof that the vitamin activity rather than some drug-like action unique to the high dose produced such dramatic results. The balance of the evidence, however, suggests that vitamin K2 is essential to skeletal health and that it is a key substance that modern diets do not adequately provide.
https://www.blogger.com/null
Vitamin K2 and Heart Disease
Price
analyzed more than 20,000 samples of dairy products sent to him every two to
four weeks from various districts of the United States, Canada, Australia,
Brazil and New Zealand. Dividing the total area into many districts, each
producing dairy products with different patterns of seasonal fluctuation in
vitamin A and Activator X content, he found an inverse relationship in each
district between the vitamin content of butterfat and the mortality from
pneumonia and heart disease.
The role of vitamin A in the immune system is well established. We do not currently know, however, whether vitamin K2 plays an important role in the immune system. Nevertheless, lymph glands and bone marrow accumulate large amounts of it62 and a vitamin K-dependent protein called gas6 plays a role in phagocytosis,33 a process wherein immune cells destroy and consume foreign cells or the body’s own cells when they are infected or no longer needed. It is therefore possible that K vitamins could play an important role in protecting against infectious diseases such as pneumonia.
Vitamin K2‘s ability to protect us from heart disease is much more clearly established. Research is in fact rapidly redefining heart disease largely as a deficiency of this vitamin. While it is most clearly established that vitamin K2 deficiency causes calcification of the cardiovascular system, vitamin K2 appears to protect against the inflammation and accumulation of lipids and white blood cells that characterize atherosclerosis as well.
Cardiovascular calcification can begin as early as the second decade of life, and is nearly ubiquitous in the population by the age of 65.33 There are primarily two types: calcification of the heart valves and tunica media constitutes one type, while calcification of the tunica intima constitutes the second. The tunica media is the middle layer of the artery; it contains elastic fibers that allow the artery to stretch and accommodate varying degrees of pressure. The elastic fibers of the tunica media and the valves of the heart calcify during diabetes, kidney disease and aging. The tunica intima is the innermost layer of the artery and is the site where atherosclerosis develops. In atherosclerosis, calcified deposits rich in lipids and white blood cells accumulate on the debris left behind by the blood vessel’s smooth muscle cells once they have died.63
In healthy arteries, the vitamin K-dependent matrix Gla protein (MGP) congregates around the elastic fibers of the tunica media and guards them against the formation of crystals by the calcium that circulates in the blood. The inactive form of MGP, which cells produce when they do not have sufficient K vitamins to meet their needs, does not exist in healthy arteries. In early atherosclerosis, by contrast, most MGP exists in its inactive form and associates with calcified structures containing lipids, white blood cells, and the remnants of dead smooth muscle cells. Inactive MGP also accumulates within the calcified deposits of the medial sclerosis that occurs during diabetes, kidney disease and aging. Although blood tests for the percentage of inactive and active MGP are not available, patients with severe calcifications have high percentages of inactive osteocalcin, indicating a general deficiency of vitamin K2.63
Two other vitamin K-dependent proteins are likely to play a role in the development of atherosclerosis: gas6 and protein S. Gas6 promotes the survival of the smooth muscle cells that line the intima and the rapid clearance of those that die. The rapid clearance of these dead cells may be important for preventing the accumulation of the calcified lipids and white blood cells that gather around them. Protein S guides the immune system to clear away this debris from the intima gently rather than mounting a dangerous inflammatory attack against it.33 As these observations all predict, experimental and epidemiological evidence both show that vitamin K2 is a powerful inhibitor of cardiovascular disease.
Mice that lack the gene for MGP develop extensive calcification of the aorta, aortic valves and arteries soon after birth and bleed to death within two months when their heavily calcified aortas rupture.38 Warfarin, which inhibits the recycling of K vitamins40 and the conversion of K1 to K2,64 causes calcification of the tunica media in rats within two weeks,21 increases arterial stiffness, decreases the ability of the artery to accommodate moderately high levels of blood pressure, and causes the death of the artery’s smooth muscle cells.65 Marcoumar, a similar drug, doubles the degree of aortic valve calcification in humans over the course of one to three years.42
Large amounts of vitamin K2 completely inhibit the ability of Warfarin to cause arterial calcification in rats. Vitamin K1, by contrast, has no inhibitory effect at all.21 Researchers from the University of Maastricht recently showed that both K vitamins can reverse calcification that has already occurred in Wistar Kyoto rats.65 The K vitamins also reduced the number of dead smooth muscle cells after Warfarin treatment, showing that vitamin K-dependent proteins not only promote cell survival but also facilitate the safe clearance of cells that have died. Although both K vitamins were effective, these rats convert vitamin K1 to vitamin K2 with great efficiency. In the absence of Warfarin, two-thirds of the vitamin K in the blood vessels of the rats that consumed K1 alone existed as K2. In the presence of Warfarin, however, which inhibits the conversion, none of the vitamin K in these blood vessels existed as K2. Apparently, vitamin K1 is effective after but not during Warfarin treatment because it can only protect against arterial calcification insofar as it is converted to vitamin K2.
In the Nurses’ Health Study, the risk of heart disease was a modest 16 percent lower for those consuming more than 110 micrograms per day of vitamin K1, but there was no benefit from consuming any more than this.66 This small amount is equivalent to consuming only three servings of kale per month. The Health Professionals Follow-Up Study generated a similar finding in men, although it lost significance after adjustment for other dietary risk factors.67 It isn’t clear whether the slight increase in risk associated with only the lowest intakes reflects the possibility that only very small amounts of vitamin K1 are absorbed, or simply reflects the association between K1 intake and a healthy lifestyle. People who consume more vitamin K1 weigh less, smoke less, eat more fruits, vegetables, fish, folate, vitamin E and fiber,68 and are more likely to use vitamin supplements.67
The inverse association between heart disease and vitamin K2 intake is more straightforward. In The Rotterdam Study, which prospectively followed just over 4,600 men aged 55 or older in the Netherlands, the highest intake of vitamin K2 was associated with a 52 percent lower risk of severe aortic calcification, a 41 percent lower risk of coronary heart disease (CHD), a 51 percent lower risk of CHD mortality, and a 26 percent lower risk of total mortality. Even though the study population consumed ten times more K1 than K2, vitamin K1 had no association with either the degree of aortic calcification or the risk of heart disease.20 The profound effects of variations in such small amounts of dietary K2 emphasize just how powerful this substance is in the prevention of degenerative disease.
https://www.blogger.com/null
The role of vitamin A in the immune system is well established. We do not currently know, however, whether vitamin K2 plays an important role in the immune system. Nevertheless, lymph glands and bone marrow accumulate large amounts of it62 and a vitamin K-dependent protein called gas6 plays a role in phagocytosis,33 a process wherein immune cells destroy and consume foreign cells or the body’s own cells when they are infected or no longer needed. It is therefore possible that K vitamins could play an important role in protecting against infectious diseases such as pneumonia.
Vitamin K2‘s ability to protect us from heart disease is much more clearly established. Research is in fact rapidly redefining heart disease largely as a deficiency of this vitamin. While it is most clearly established that vitamin K2 deficiency causes calcification of the cardiovascular system, vitamin K2 appears to protect against the inflammation and accumulation of lipids and white blood cells that characterize atherosclerosis as well.
Cardiovascular calcification can begin as early as the second decade of life, and is nearly ubiquitous in the population by the age of 65.33 There are primarily two types: calcification of the heart valves and tunica media constitutes one type, while calcification of the tunica intima constitutes the second. The tunica media is the middle layer of the artery; it contains elastic fibers that allow the artery to stretch and accommodate varying degrees of pressure. The elastic fibers of the tunica media and the valves of the heart calcify during diabetes, kidney disease and aging. The tunica intima is the innermost layer of the artery and is the site where atherosclerosis develops. In atherosclerosis, calcified deposits rich in lipids and white blood cells accumulate on the debris left behind by the blood vessel’s smooth muscle cells once they have died.63
In healthy arteries, the vitamin K-dependent matrix Gla protein (MGP) congregates around the elastic fibers of the tunica media and guards them against the formation of crystals by the calcium that circulates in the blood. The inactive form of MGP, which cells produce when they do not have sufficient K vitamins to meet their needs, does not exist in healthy arteries. In early atherosclerosis, by contrast, most MGP exists in its inactive form and associates with calcified structures containing lipids, white blood cells, and the remnants of dead smooth muscle cells. Inactive MGP also accumulates within the calcified deposits of the medial sclerosis that occurs during diabetes, kidney disease and aging. Although blood tests for the percentage of inactive and active MGP are not available, patients with severe calcifications have high percentages of inactive osteocalcin, indicating a general deficiency of vitamin K2.63
Two other vitamin K-dependent proteins are likely to play a role in the development of atherosclerosis: gas6 and protein S. Gas6 promotes the survival of the smooth muscle cells that line the intima and the rapid clearance of those that die. The rapid clearance of these dead cells may be important for preventing the accumulation of the calcified lipids and white blood cells that gather around them. Protein S guides the immune system to clear away this debris from the intima gently rather than mounting a dangerous inflammatory attack against it.33 As these observations all predict, experimental and epidemiological evidence both show that vitamin K2 is a powerful inhibitor of cardiovascular disease.
Mice that lack the gene for MGP develop extensive calcification of the aorta, aortic valves and arteries soon after birth and bleed to death within two months when their heavily calcified aortas rupture.38 Warfarin, which inhibits the recycling of K vitamins40 and the conversion of K1 to K2,64 causes calcification of the tunica media in rats within two weeks,21 increases arterial stiffness, decreases the ability of the artery to accommodate moderately high levels of blood pressure, and causes the death of the artery’s smooth muscle cells.65 Marcoumar, a similar drug, doubles the degree of aortic valve calcification in humans over the course of one to three years.42
Large amounts of vitamin K2 completely inhibit the ability of Warfarin to cause arterial calcification in rats. Vitamin K1, by contrast, has no inhibitory effect at all.21 Researchers from the University of Maastricht recently showed that both K vitamins can reverse calcification that has already occurred in Wistar Kyoto rats.65 The K vitamins also reduced the number of dead smooth muscle cells after Warfarin treatment, showing that vitamin K-dependent proteins not only promote cell survival but also facilitate the safe clearance of cells that have died. Although both K vitamins were effective, these rats convert vitamin K1 to vitamin K2 with great efficiency. In the absence of Warfarin, two-thirds of the vitamin K in the blood vessels of the rats that consumed K1 alone existed as K2. In the presence of Warfarin, however, which inhibits the conversion, none of the vitamin K in these blood vessels existed as K2. Apparently, vitamin K1 is effective after but not during Warfarin treatment because it can only protect against arterial calcification insofar as it is converted to vitamin K2.
In the Nurses’ Health Study, the risk of heart disease was a modest 16 percent lower for those consuming more than 110 micrograms per day of vitamin K1, but there was no benefit from consuming any more than this.66 This small amount is equivalent to consuming only three servings of kale per month. The Health Professionals Follow-Up Study generated a similar finding in men, although it lost significance after adjustment for other dietary risk factors.67 It isn’t clear whether the slight increase in risk associated with only the lowest intakes reflects the possibility that only very small amounts of vitamin K1 are absorbed, or simply reflects the association between K1 intake and a healthy lifestyle. People who consume more vitamin K1 weigh less, smoke less, eat more fruits, vegetables, fish, folate, vitamin E and fiber,68 and are more likely to use vitamin supplements.67
The inverse association between heart disease and vitamin K2 intake is more straightforward. In The Rotterdam Study, which prospectively followed just over 4,600 men aged 55 or older in the Netherlands, the highest intake of vitamin K2 was associated with a 52 percent lower risk of severe aortic calcification, a 41 percent lower risk of coronary heart disease (CHD), a 51 percent lower risk of CHD mortality, and a 26 percent lower risk of total mortality. Even though the study population consumed ten times more K1 than K2, vitamin K1 had no association with either the degree of aortic calcification or the risk of heart disease.20 The profound effects of variations in such small amounts of dietary K2 emphasize just how powerful this substance is in the prevention of degenerative disease.
https://www.blogger.com/null
Vitamin K2 and the Brain
Price
supplied several anecdotes suggesting that Activator X plays an important role
in the nervous system. Price administered a daily meal of nutrient-dense whole
foods supplemented with high-vitamin cod liver oil and high-Activator X butter
oil to the children of impoverished mill workers who suffered from rampant
tooth decay. The treatment not only resolved the tooth decay without the need
for oral surgery, but resolved chronic fatigue in one boy and by the report of
their school teachers produced a marked increase in learning capacity in two
others.
Price also administered the butter oil concentrate to a four-year-old who suffered from rampant tooth decay, a fractured leg and seizures. A dessert spoonful of the butter oil served over whole wheat gruel with whole milk once before bed and five times over the course of the following day immediately resolved his seizures. Rapid healing of his fracture and dental caries followed soon after. The fact that these three symptoms appeared together and resolved following the same treatment suggests a common cause for each of them. Sixty years later, modern research is now elucidating the essential role that vitamin K2 plays not only in the dental and skeletal systems, but in the nervous system as well. This strongly suggests it was the key unidentified factor in Price’s protocol.
The brain contains one of the highest concentrations of vitamin K2 in the body; only the pancreas, salivary glands, and the cartilaginous tissue of the sternum contain more. When male Wistar rats consume vitamin K1 alone, 98 percent of the vitamin K in their brains exists as K2, demonstrating the overwhelming preference of the nervous system for this form. The K2 contents of these four tissues remain remarkably high on a vitamin K-deficient diet, suggesting either that the vitamin is so essential to their function that they have developed a highly efficient means of preserving it, or that it plays a unique role in these tissues that does not require as high a rate of turnover as is required by the roles it plays in most other tissues.15
An analysis of three autopsies showed that vitamin K2 makes up between 70 and 93 percent of the vitamin K in the human brain.69 It is not clear why humans exhibit greater variation in this percentage than rats, although it could be that we convert K1 less efficiently and are therefore more dependent on dietary K2.
Vitamin K2 supports the enzymes within the brain that produce an important class of lipids called sulfatides. The levels of vitamin K2, vitamin K-dependent proteins and sulfatides in the brain decline with age; the decline of these levels is in turn associated with age-related neurological degeneration.46 Comparisons of human autopsies associate the early stages of Alzheimer’s disease with up to 93 percent lower sulfatide levels in the brain.70 Warfarin treatment or dietary vitamin K deficiency causes lack of exploratory behavior and reduced physical activity in rats that is suggestive of fatigue.71 Animals that completely lack the enzymes to make sulfatides and a related class of lipids, cerebrosides, progressively suffer from growth retardation, loss of locomotor activity, weak legs and seizures.72
These observations suggest that deficiencies in vitamin K, especially vitamin K2, could result in fatigue and learning difficulties in humans, and that rare, extreme deficiencies of vitamin K2 in the brain could result in seizures. If this is the case, it would explain why Price observed tooth decay, bone fracture, learning difficulties and seizures to share a common cause and a common solution.
https://www.blogger.com/null
Price also administered the butter oil concentrate to a four-year-old who suffered from rampant tooth decay, a fractured leg and seizures. A dessert spoonful of the butter oil served over whole wheat gruel with whole milk once before bed and five times over the course of the following day immediately resolved his seizures. Rapid healing of his fracture and dental caries followed soon after. The fact that these three symptoms appeared together and resolved following the same treatment suggests a common cause for each of them. Sixty years later, modern research is now elucidating the essential role that vitamin K2 plays not only in the dental and skeletal systems, but in the nervous system as well. This strongly suggests it was the key unidentified factor in Price’s protocol.
The brain contains one of the highest concentrations of vitamin K2 in the body; only the pancreas, salivary glands, and the cartilaginous tissue of the sternum contain more. When male Wistar rats consume vitamin K1 alone, 98 percent of the vitamin K in their brains exists as K2, demonstrating the overwhelming preference of the nervous system for this form. The K2 contents of these four tissues remain remarkably high on a vitamin K-deficient diet, suggesting either that the vitamin is so essential to their function that they have developed a highly efficient means of preserving it, or that it plays a unique role in these tissues that does not require as high a rate of turnover as is required by the roles it plays in most other tissues.15
An analysis of three autopsies showed that vitamin K2 makes up between 70 and 93 percent of the vitamin K in the human brain.69 It is not clear why humans exhibit greater variation in this percentage than rats, although it could be that we convert K1 less efficiently and are therefore more dependent on dietary K2.
Vitamin K2 supports the enzymes within the brain that produce an important class of lipids called sulfatides. The levels of vitamin K2, vitamin K-dependent proteins and sulfatides in the brain decline with age; the decline of these levels is in turn associated with age-related neurological degeneration.46 Comparisons of human autopsies associate the early stages of Alzheimer’s disease with up to 93 percent lower sulfatide levels in the brain.70 Warfarin treatment or dietary vitamin K deficiency causes lack of exploratory behavior and reduced physical activity in rats that is suggestive of fatigue.71 Animals that completely lack the enzymes to make sulfatides and a related class of lipids, cerebrosides, progressively suffer from growth retardation, loss of locomotor activity, weak legs and seizures.72
These observations suggest that deficiencies in vitamin K, especially vitamin K2, could result in fatigue and learning difficulties in humans, and that rare, extreme deficiencies of vitamin K2 in the brain could result in seizures. If this is the case, it would explain why Price observed tooth decay, bone fracture, learning difficulties and seizures to share a common cause and a common solution.
https://www.blogger.com/null
Other Roles of Vitamin K2
Our
understanding of the K vitamins is rapidly expanding and we are likely to
discover many new roles for them as the twenty-first century progresses.
The highest concentration of vitamin K2 exists in the salivary glands and the pancreas. These organs exhibit an overwhelming preference for K2 over K1 and retain high amounts of the vitamin even when animals consume a vitamin K-deficient diet.15 The high presence of the vitamin in both of these organs suggests a role in activating digestive enzymes, although its apparent role in the regulation of blood sugar could explain its presence in the pancreas.76 The testes of male rats also exhibit a high preference for and retention of vitamin K2,16 and human sperm possess a vitamin K-dependent protein with an unknown function.77 The kidneys likewise accumulate large amounts of vitamin K269 and secrete vitamin K-dependent proteins that inhibit the formation of calcium salts. Patients with kidney stones secrete this protein in its inactive form, which is between four and twenty times less effective than its active form at inhibiting the growth of calcium oxalate crystals, suggesting that vitamin K2 deficiency is a major cause of kidney stones.77
The use of Warfarin during pregnancy produces developmental malformations of the face; as the nasal cartilage calcifies, growth of the nose comes to an early end, resulting in a stubby appearance.78 Vitamin K2 therefore most certainly played a role in the development of beautiful faces with broad features that Price observed among primitive peoples.
A number of cell experiments have shown that vitamin K2 has powerful anti-carcinogenic properties that may make it useful in preventing or treating cancer in humans.79
Researchers have recently discovered a whole new class of vitamin K-dependent proteins called transmembrane Gla (TMG) proteins. Their functions are unknown.33
The K vitamins perform all of their well understood roles in the part of the cell responsible for the modification of proteins. Only a portion of the vitamin K within a cell exists in this area, however. Even more exists in the inner membrane of the mitochondria where the cell produces its energy.45 The greatest concentration exists in the nucleus, which possesses a receptor for vitamin K that may be involved in regulating the expression of genes.44 Vitamin K2 has a greater affinity than vitamin K1 for both the mitochondrial membrane and the nuclear receptor. We presently know virtually nothing about these functions of the K vitamins and the plot will only thicken as the story unfolds.
https://www.blogger.com/null
The highest concentration of vitamin K2 exists in the salivary glands and the pancreas. These organs exhibit an overwhelming preference for K2 over K1 and retain high amounts of the vitamin even when animals consume a vitamin K-deficient diet.15 The high presence of the vitamin in both of these organs suggests a role in activating digestive enzymes, although its apparent role in the regulation of blood sugar could explain its presence in the pancreas.76 The testes of male rats also exhibit a high preference for and retention of vitamin K2,16 and human sperm possess a vitamin K-dependent protein with an unknown function.77 The kidneys likewise accumulate large amounts of vitamin K269 and secrete vitamin K-dependent proteins that inhibit the formation of calcium salts. Patients with kidney stones secrete this protein in its inactive form, which is between four and twenty times less effective than its active form at inhibiting the growth of calcium oxalate crystals, suggesting that vitamin K2 deficiency is a major cause of kidney stones.77
The use of Warfarin during pregnancy produces developmental malformations of the face; as the nasal cartilage calcifies, growth of the nose comes to an early end, resulting in a stubby appearance.78 Vitamin K2 therefore most certainly played a role in the development of beautiful faces with broad features that Price observed among primitive peoples.
A number of cell experiments have shown that vitamin K2 has powerful anti-carcinogenic properties that may make it useful in preventing or treating cancer in humans.79
Researchers have recently discovered a whole new class of vitamin K-dependent proteins called transmembrane Gla (TMG) proteins. Their functions are unknown.33
The K vitamins perform all of their well understood roles in the part of the cell responsible for the modification of proteins. Only a portion of the vitamin K within a cell exists in this area, however. Even more exists in the inner membrane of the mitochondria where the cell produces its energy.45 The greatest concentration exists in the nucleus, which possesses a receptor for vitamin K that may be involved in regulating the expression of genes.44 Vitamin K2 has a greater affinity than vitamin K1 for both the mitochondrial membrane and the nuclear receptor. We presently know virtually nothing about these functions of the K vitamins and the plot will only thicken as the story unfolds.
https://www.blogger.com/null
Vitamin K2 in Foods
Figure
4 shows the distribution of vitamin K2 in selected foods.
Precise values for the organ meats that would be richest in K2 are
not available. The pancreas and salivary glands would be richest; reproductive
organs, brains, cartilage and possibly kidneys would also be very rich;
finally, bone would be richer than muscle meat.15,16,69 Analyses of
fish eggs, which Price found to be rich in Activator X, are not available.
Commercial butter is only a moderate source of vitamin K2. After analyzing over 20,000 samples of butter sent to him from around the world, however, Price found that the Activator X concentration varied 50-fold. Vitamin K-rich cereal grasses, especially wheat grass, and alfalfa in a lush green state of growth produced the highest amounts of Activator X, but the soil in which the pasture was grown also profoundly influenced the quality of the butter. The concentrations were lowest in the eastern and far western states where the soil had been tilled the longest, and were highest in Deaf Smith County, Texas, where excavations proved the roots of the wheat grass to pass down six feet or more through three feet of top soil into deposits of glacial pebbles cemented together with calcium carbonate. It was this amazingly vitamin-rich butter that had such dramatic curative properties when combined with high-vitamin cod liver oil and nutrient-dense meals of whole milk, whole grains, organ meats, bone broths, fruits and vegetables.
For over 50 years after Price described his discovery of Activator X, the medical and nutritional communities saw vitamin K merely as a requirement for blood clotting. The poor understanding of the functions of the K vitamins within the body and the apparent lack of any relationship between Price’s chemical test and the structure of any known vitamin made it impossible to determine the identity of this mysterious substance. We now know, however, that vitamin K2 and Activator X are one and the same. Like Price’s X factor, vitamin K2 is synthesized by animal bodies from its precursor in rapidly growing grass. Cereal grasses and alfalfa are rich in this precursor, and these plants accumulate it in direct proportion to their photosynthetic activity. It is critical to the ability of teeth and bones to lay down mineralized tissue, and to the prevention of degenerative diseases of the cardiovascular and nervous systems. It is the key factor that acts in synergy with vitamins A and D: these vitamins command cells to make proteins, but vitamin K brings these proteins to life. It is an “activator,” then, in the truest sense of the word, and it is therefore fitting that we knew it for so many decades simply as “Activator X.”
Thank you to Michael Eiseike, a health researcher from Hokkaido Japan, for originally bringing the Rotterdam Study to our attention and suggesting that vitamin K2 may be the X Factor of Weston Price; and also to David Wetzel of Green Pasture Products for his input and advice.
https://www.blogger.com/nullFigures
https://www.blogger.com/null
Commercial butter is only a moderate source of vitamin K2. After analyzing over 20,000 samples of butter sent to him from around the world, however, Price found that the Activator X concentration varied 50-fold. Vitamin K-rich cereal grasses, especially wheat grass, and alfalfa in a lush green state of growth produced the highest amounts of Activator X, but the soil in which the pasture was grown also profoundly influenced the quality of the butter. The concentrations were lowest in the eastern and far western states where the soil had been tilled the longest, and were highest in Deaf Smith County, Texas, where excavations proved the roots of the wheat grass to pass down six feet or more through three feet of top soil into deposits of glacial pebbles cemented together with calcium carbonate. It was this amazingly vitamin-rich butter that had such dramatic curative properties when combined with high-vitamin cod liver oil and nutrient-dense meals of whole milk, whole grains, organ meats, bone broths, fruits and vegetables.
For over 50 years after Price described his discovery of Activator X, the medical and nutritional communities saw vitamin K merely as a requirement for blood clotting. The poor understanding of the functions of the K vitamins within the body and the apparent lack of any relationship between Price’s chemical test and the structure of any known vitamin made it impossible to determine the identity of this mysterious substance. We now know, however, that vitamin K2 and Activator X are one and the same. Like Price’s X factor, vitamin K2 is synthesized by animal bodies from its precursor in rapidly growing grass. Cereal grasses and alfalfa are rich in this precursor, and these plants accumulate it in direct proportion to their photosynthetic activity. It is critical to the ability of teeth and bones to lay down mineralized tissue, and to the prevention of degenerative diseases of the cardiovascular and nervous systems. It is the key factor that acts in synergy with vitamins A and D: these vitamins command cells to make proteins, but vitamin K brings these proteins to life. It is an “activator,” then, in the truest sense of the word, and it is therefore fitting that we knew it for so many decades simply as “Activator X.”
Thank you to Michael Eiseike, a health researcher from Hokkaido Japan, for originally bringing the Rotterdam Study to our attention and suggesting that vitamin K2 may be the X Factor of Weston Price; and also to David Wetzel of Green Pasture Products for his input and advice.
https://www.blogger.com/nullFigures
https://www.blogger.com/null
Figure 1: The Structure of K Vitamins and Their Chemical Behavior
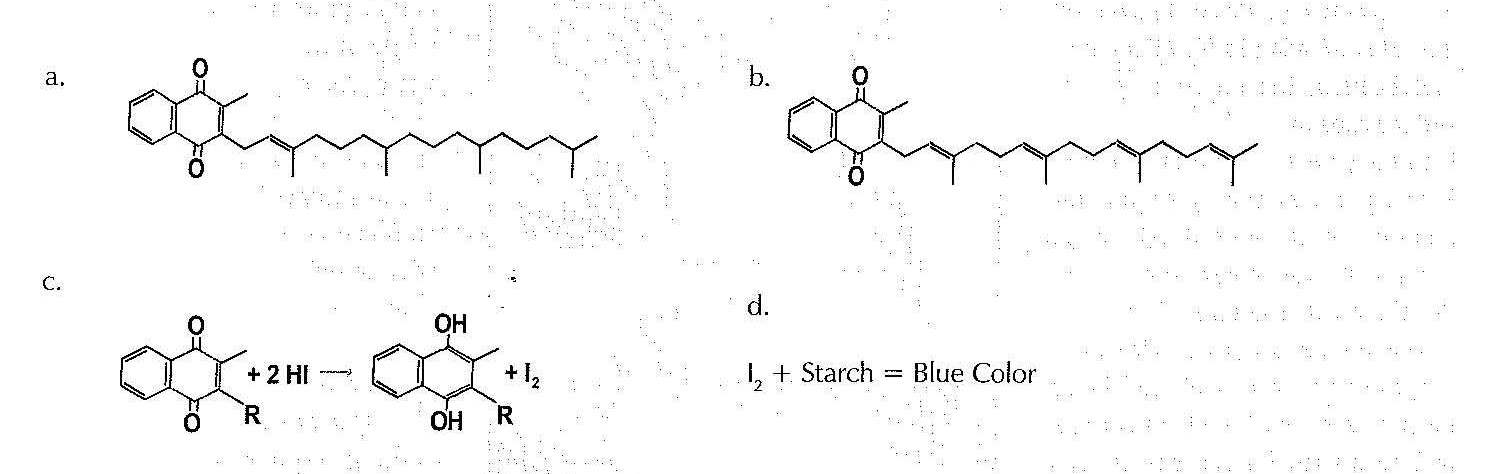
Single lines represent single bonds between carbon atoms; double lines represent double bonds between carbon atoms. Hydrogen atoms are attached to most of the carbons but are not shown.
a. Vitamin K1. The side chain extending to the right of the molecule is monounsaturated.
b. Vitamin K2. The nucleus, composed of two ring structures, is the same as that of vitamin K1. The side chain, however, is polyunsaturated rather than monounsaturated.
c. Either K vitamin would be expected to react with hydriodic acid (HI) by absorbing hydrogen atoms and liberating diatomic iodine (I2). The side chain is abbreviated by the letter “R.”
d. If the mixture of the vitamin K and hydriodic acid is combined with a starch indictor, the diatomic iodine liberated by the reaction would turn the starch blue.
|
Figure
2. Corresponding Characteristics of Activator X and Vitamin K2
|
|
|
Activator
X
|
Vitamin
K2
|
|
Found
in the butterfat of mammalian milk, the eggs of fishes, and the organs and
fats of animals.
|
Found
in the butterfat of mammalian milk and the organs and fats of animals.
Analyses of fish eggs are not available.
|
|
Synthesized
by animal tissues, including the mammary glands, from a precursor in rapidly
growing, green grass.
|
Synthesized
by animal tissues, including the mammary glands, from vitamin K1,
which is found in association with the chlorophyll of green plants in
proportion to their photosynthetic activity.
|
|
The
content of this vitamin in butterfat is proportional to the richness of its
yellow or orange color.
|
Its
precursor is directly associated with beta-carotene, which imparts a yellow
or orange color to butterfat.
|
|
Liberates
diatomic iodine from hydriodic acid during chemical testing.
|
Liberates
diatomic iodine from hydriodic acid during chemical testing.
|
|
Acts
synergistically with vitamins A and D.
|
Activates
proteins that cells are signaled to produce by vitamins A and D.
|
|
Plays
an important role in reproduction.
|
Synthesized
by the reproductive organs in large amounts from vitamin K1 and
preferentially retained by these organs on a vitamin K-deficient diet. Sperm
possess a K2-dependent protein of unknown function.
|
|
Plays
a role in infant growth.
|
Contributes
to infant and childhood growth by preventing the premature calcification of
the cartilaginous growth zones of bones.
|
|
Plays
an essential role in mineral utilization and is necessary for the control of
dental caries.
|
Activates
proteins responsible for the deposition of calcium and phosphorus salts in
bones and teeth and the protection of soft tissues from calcification.
|
|
Increases
mineral content and decreases bacterial count of saliva.
|
Is
found in the second highest concentration in the salivary glands, and is
present in saliva.
|
|
Intake
is inversely associated with heart disease.
|
Protects
against the calcification and inflammation of blood vessels and the
accumulation of atherosclerotic plaque.
|
|
Increases
learning capacity.
|
The
brain contains one of the highest concentrations of vitamin K2,
where it is involved in the synthesis of the myelin sheath of nerve cells,
which contributes to learning capacity.
|
|
Resolved
chronic fatigue in one boy.
|
Deficiency
induces fatigue in laboratory animals.
|
|
Resolved
seizures in one boy.
|
Involved
in the synthesis of lipids called sulfatides in the brain, an absence of
which induces seizures in laboratory animals.
|
Figure 3. Vitamin K-Dependent Carboxylation
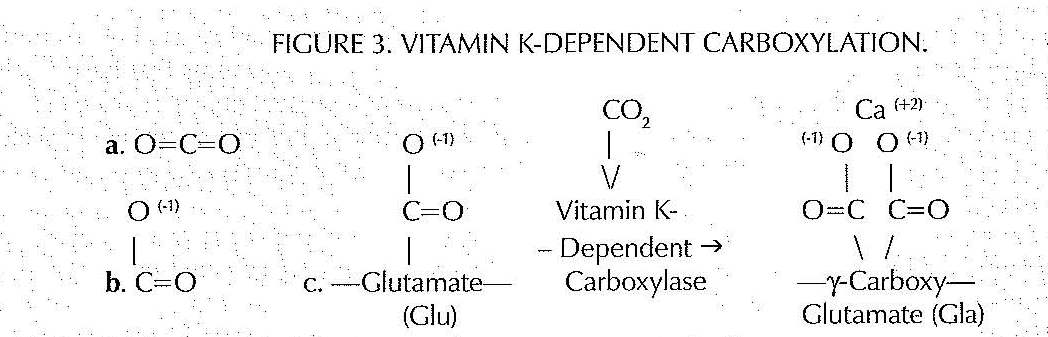
a.) A carbon dioxide molecule
b.) a carboxyl group
c.) Vitamin K-dependent carboxylation
The vitamin K-dependent carboxylase rearranges the chemical bonds within carbon dioxide molecules. Carboxyl groups contain carbon and oxygen atoms and carry a charge of negative one. Calcium carries a charge of positive two. The side chains of the amino acid glutamate normally carry one carboxyl group; the vitamin K-dependent addition of a second carboxyl group gives these side chains a charge of negative two and thus allows them to bind to calcium, which has the equal and opposite charge. This process transforms glutamate into γ-carboxyglutamate, abbreviated Gla. For this reason, many vitamin K-dependent proteins, such as matrix Gla protein (MGP), contain “Gla” in their name.
https://www.blogger.com/null
Figure 4: Vitamin K2 Contents of Selected Foods22, 26
The
percentage of vitamin K2 present as MK-4 represents that synthesized
by animal tissues, while the remainder represents that synthesized by bacteria
during fermentation.
|
FOOD
|
VITAMIN K2
|
(MCG/100G)
|
|
Natto
|
1103.4
|
(0%
MK-4)
|
|
Goose
Liver Paste
|
369.0
|
(100%
MK-4)
|
|
Hard
Cheeses
|
76.3
|
(6%
MK-4)
|
|
Soft
Cheeses
|
56.5
|
(6.5%
MK-4)
|
|
Egg
Yolk (Netherlands)
|
32.1
|
(98%
MK-4)
|
|
Goose
Leg
|
31.0
|
(100%
MK-4)
|
|
Curd
Cheeses
|
24.8
|
(1.6%
MK-4)
|
|
Egg
Yolk (United States)
|
15.5
|
(100%
MK-4)
|
|
Butter
|
15.0
|
(100%
MK-4)
|
|
Chicken
Liver
|
14.1
|
(100%
MK-4)
|
|
Salami
|
9.0
|
(100%
MK-4)
|
|
Chicken
Breast
|
8.9
|
(100%
MK-4)
|
|
Chicken
Leg
|
8.5
|
(100%
MK-4)
|
|
Ground
Beef (Medium Fat)
|
8.1
|
(100%
MK-4)
|
|
Bacon
|
5.6
|
(100%
MK-4)
|
|
Calf
Liver
|
5.0
|
(100%
MK-4)
|
|
Sauerkraut
|
4.8
|
(8%
MK-4)
|
|
Whole
Milk
|
1.0
|
(100%
MK-4)
|
|
2%
Milk
|
0.5
|
(100%
MK-4)
|
|
Salmon
|
0.5
|
(100%
MK-4)
|
|
Mackerel
|
0.4
|
(100%
MK-4)
|
|
Egg
White
|
0.4
|
(100%
MK-4)
|
|
Skim
Milk
|
0.0
|
|
|
Fat-Free
Meats
|
0.0
|
|
The Activator X Test
The
chemical test that Price eventually came to use for the quantification of
Activator X in foods was originally suggested as an indirect test for vitamin
D by Lester Yoder of the Agricultural Experiment Station of Iowa State College
in 1926.8 The basic principle of the test, called iodometric
determination, was most commonly utilized in the United States for detecting
the presence of organic peroxides.9 Since peroxides are capable of
oxidizing ionic iodide to diatomic iodine, researchers can detect them by
combining the test substance with hydriodic acid and a starch indicator.
Hydriodic acid releases iodide ions into a solution. If peroxides are present,
they convert these iodide ions to diatomic iodine, which then turns the starch
blue or purple.
This is somewhat similar to the amylase test that is used as a demonstration in many high school or college biology classes. In that test, however, preformed iodine is used; in the absence of amylase, the iodine turns the starch blue, while in the presence of amylase, the starch is broken down into sugar and the color change does not occur.
At the time, the only way to test a food for vitamin D was to feed it to rats on a mineral-deficient diet, kill the rats, and analyze the mineral content of their bones. The richer the food was in vitamin D, the more it would stimulate absorption of the small amounts of calcium and phosphorus in the diet and the higher the bone mineral content would be. Yoder suggested, however, that there was a general correlation between the ability of an oil to peroxidize (become rancid) and its vitamin D content, and advocated testing an oil’s ability to oxidize iodide as an indirect indicator of its level of vitamin D. Having no other convenient chemical test, Price adopted this as his test for vitamin D.
The test was far from perfect. Yoder found peroxidation in substances with no vitamin D activity such as turpentine, a thirteen-year-old sample of cholesterol, and an aged sample of mineral oil. He further found that irradiating foods to the point at which their vitamin D activity was destroyed actually increased their score on the test.8
As Price used this test on over 20,000 samples of dairy foods sent to him from around the world, he realized that the physiological effects that correlated with a food’s ranking were different from those attributable to isolated vitamin D, and began using the term “Activator X” to describe the nutritional substance that the test was measuring. He observed that the vitamin content of these butter samples varied fifty-fold, and that the samples richest in Activator X were the most potent for controlling dental caries. Clearly, Price’s test was detecting something besides rancid oils.
While researchers who published in English language journals traditionally used this test to detect peroxides, researchers publishing in Russian and German language journals had been using it to detect the synthetic compound benzoquinone all along.10,11 Benzoquinone belongs to a class of chemicals called quinones that includes biological molecules such as coenzyme Q10 and the K vitamins. These quinones possess oxygen-containing ring structures whose oxygens will steal electrons and hydrogen ions from hydriodic acid and thereby oxidize ionic iodide to diatomic iodine, causing the starch to become a bluish purple color (see Figure 1).
In the 1970s, researchers from Britain and Denmark were debating whether or not healthy rat tissues contained lipid peroxides. The British researchers used the iodometric method to determine peroxide levels and argued that healthy rat tissues did contain peroxides, while the Danish researchers used a different method and argued that they did not. In a 1972 paper published in the British Journal of Nutrition, the Danish researchers demonstrated that the iodometric method was not showing the existence of peroxides in the rat tissues, but rather the existence of coenzyme Q10 and probably other quinones.12
Price’s test, therefore, was not specific to any one particular chemical compound. When used for fresh oils, however, it would be able to detect a number of nutrients that include coenzyme Q10 and the K vitamins. As shown in this article, it is the K vitamins that we should expect to vary in direct proportion to the amount of richly green grass in the diet of the animals, while the physiological effects Price identified with Activator X are specifically attributable to vitamin K2.
This is somewhat similar to the amylase test that is used as a demonstration in many high school or college biology classes. In that test, however, preformed iodine is used; in the absence of amylase, the iodine turns the starch blue, while in the presence of amylase, the starch is broken down into sugar and the color change does not occur.
At the time, the only way to test a food for vitamin D was to feed it to rats on a mineral-deficient diet, kill the rats, and analyze the mineral content of their bones. The richer the food was in vitamin D, the more it would stimulate absorption of the small amounts of calcium and phosphorus in the diet and the higher the bone mineral content would be. Yoder suggested, however, that there was a general correlation between the ability of an oil to peroxidize (become rancid) and its vitamin D content, and advocated testing an oil’s ability to oxidize iodide as an indirect indicator of its level of vitamin D. Having no other convenient chemical test, Price adopted this as his test for vitamin D.
The test was far from perfect. Yoder found peroxidation in substances with no vitamin D activity such as turpentine, a thirteen-year-old sample of cholesterol, and an aged sample of mineral oil. He further found that irradiating foods to the point at which their vitamin D activity was destroyed actually increased their score on the test.8
As Price used this test on over 20,000 samples of dairy foods sent to him from around the world, he realized that the physiological effects that correlated with a food’s ranking were different from those attributable to isolated vitamin D, and began using the term “Activator X” to describe the nutritional substance that the test was measuring. He observed that the vitamin content of these butter samples varied fifty-fold, and that the samples richest in Activator X were the most potent for controlling dental caries. Clearly, Price’s test was detecting something besides rancid oils.
While researchers who published in English language journals traditionally used this test to detect peroxides, researchers publishing in Russian and German language journals had been using it to detect the synthetic compound benzoquinone all along.10,11 Benzoquinone belongs to a class of chemicals called quinones that includes biological molecules such as coenzyme Q10 and the K vitamins. These quinones possess oxygen-containing ring structures whose oxygens will steal electrons and hydrogen ions from hydriodic acid and thereby oxidize ionic iodide to diatomic iodine, causing the starch to become a bluish purple color (see Figure 1).
In the 1970s, researchers from Britain and Denmark were debating whether or not healthy rat tissues contained lipid peroxides. The British researchers used the iodometric method to determine peroxide levels and argued that healthy rat tissues did contain peroxides, while the Danish researchers used a different method and argued that they did not. In a 1972 paper published in the British Journal of Nutrition, the Danish researchers demonstrated that the iodometric method was not showing the existence of peroxides in the rat tissues, but rather the existence of coenzyme Q10 and probably other quinones.12
Price’s test, therefore, was not specific to any one particular chemical compound. When used for fresh oils, however, it would be able to detect a number of nutrients that include coenzyme Q10 and the K vitamins. As shown in this article, it is the K vitamins that we should expect to vary in direct proportion to the amount of richly green grass in the diet of the animals, while the physiological effects Price identified with Activator X are specifically attributable to vitamin K2.
Interactions between Vitamins A, D, and K2
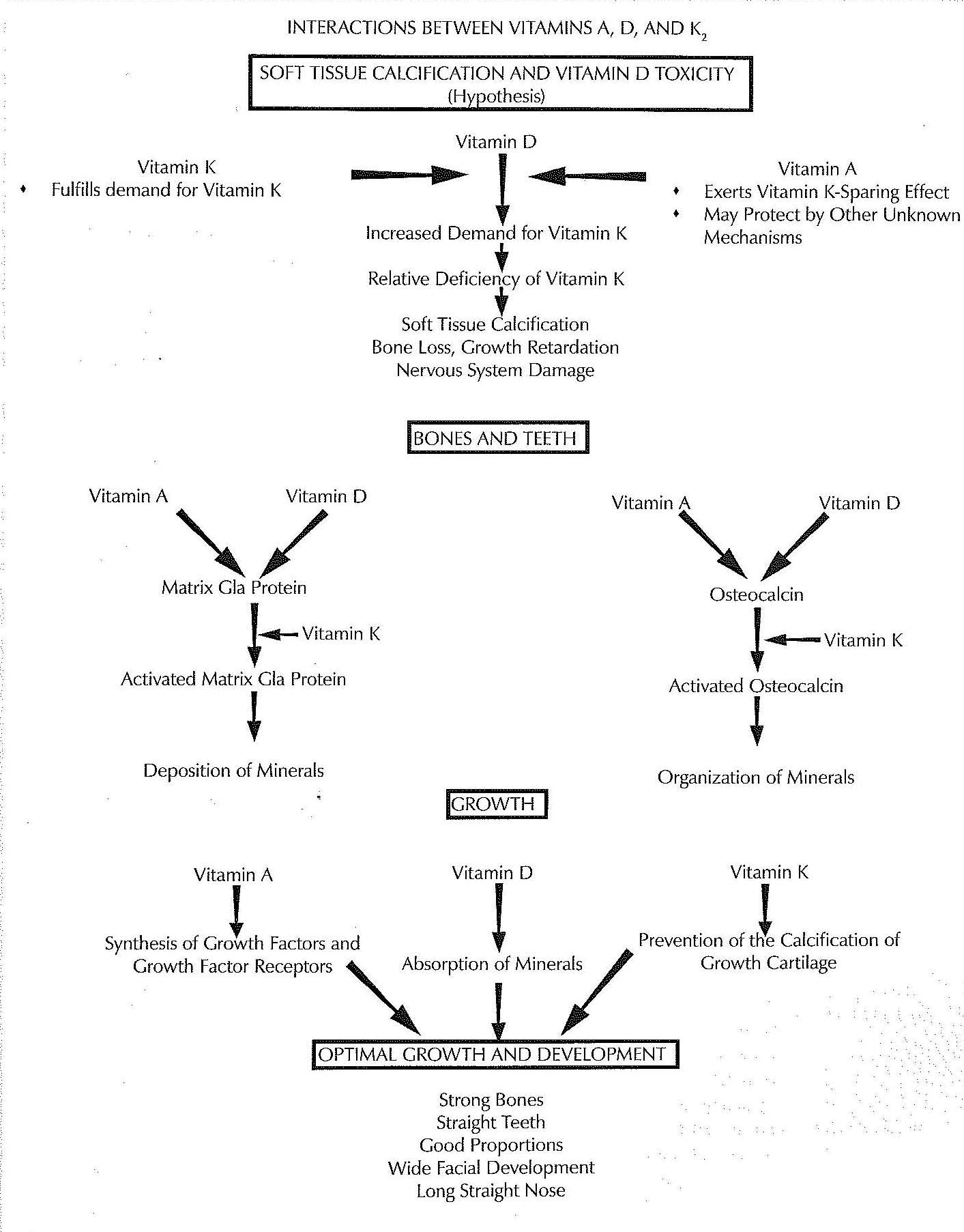
Is Vitamin K2 an Essential Nutrient?
Vitamins K1
and K2 are both effective cofactors for the enzyme that activates
vitamin K-dependent proteins,23 but the liver preferentially uses
vitamin K1 to activate clotting factors while most other tissues
preferentially use vitamin K2 to activate the other vitamin
K-dependent proteins.21 Although animals can convert vitamin K1
to vitamin K2,14 there are a number of lines of evidence
strongly suggesting that humans require preformed K2 in the diet to
obtain optimal health.
Humans appear to have a finite ability to absorb vitamin K1 from plant foods. In the United States, where the mean intake of vitamin K1 is less than 150 micrograms per day, blood levels increase with increasing dietary intake until the latter reaches two hundred micrograms per day, after which they plateau. In the Netherlands, where the mean intake of vitamin K1 is much higher (250 micrograms per day), plasma levels of vitamin K1 have no relationship to dietary intake at all.24 These results suggest that humans do not possess the ability to absorb much more than 200 micrograms of vitamin K1 per day from vegetables.
This interpretation is also supported by feeding experiments. Whereas the absorption of vitamin K2 from natto, a fermented soy food, is nearly complete, the absorption of vitamin K1 from servings of green vegetables ranging from two hundred to four hundred grams consumed without added fat is only between five and ten percent. The absorption of similarly sized servings of vegetables with added fat is still only between ten and fifteen percent.25-26 By contrast, smaller servings are absorbed more efficiently. For example, the absorption from a 150-gram serving of spinach is 17 percent and the absorption from a 50-gram serving of spinach is 28 percent.27 These results show that our absorption of the vitamin declines as the amount we consume increases and strengthens the interpretation that we might only be able to absorb about 200 micrograms per day. When study subjects consume a highly absorbable pharmacological preparation of vitamin K1, a dose of 1000 micrograms per day is required to maximize the activation of proteins important to bone metabolism.28 If we can only absorb one-fifth of this amount from vegetables, we cannot support our skeletal system with vitamin K1 regardless of how efficiently we may be able to convert it to vitamin K2.
The ability to convert K1 to K2 varies widely between species and breeds of animals. The German researchers who first reported this conversion found that rats made it poorly compared to birds and that pigeons made it most efficiently.14 Every tissue tested in male Wistar rats is capable of making the conversion,15 whereas the liver, kidneys and heart of male Lewis rats will preferentially accumulate preformed K2, but, unlike the pancreas and testes of these same animals, will not synthesize it from K1.16 The K2 content of human breast milk increases when mothers consume pharmacological preparations of K1, but the K2 content of their blood does not;17 since the conversion takes place in the target tissues rather than the blood, however, we do not know how efficiently other human tissues make this conversion.
Vitamins K1 and K2 share a common ring-structured nucleus but possess different types of side chains. The first step in the conversion of K1 to K2 appears to be the cleavage of its side chain in either the liver or the gastrointestinal tract, yielding a toxic oxidizing agent called menadione; much of this metabolite is detoxified by the liver and excreted in the urine, while the remaining portion can be used to synthesize K2 in tissues.29 After this cleavage takes place, menadione must be transported to its target tissues where cellular enzymes can add a side chain to it, completing the transformation to K2. Because they are transported in different types of lipoproteins, vitamin K1 is primarily sent to the liver, whereas vitamin K2 is primarily sent to the other tissues;30 we know very little, however, about the transport of menadione in the blood. We also know very little about the rate at which our cells are capable of adding side chains to these molecules; presumably, if the supply of menadione exceeds the rate at which the cell can add these side chains, the menadione will exert toxic effects and cause oxidative damage within the cell. Preliminary evidence indicates that doses of 1000 micrograms per day of supplemental K1 may contribute to periodontal disease,31 suggesting that our bodies’ resistance to absorbing this much K1 from vegetables may serve an important purpose.
The clearest demonstration that humans require dietary preformed vitamin K2 for optimal health is that epidemiological and intervention studies both show its superiority over K1. Intake of vitamin K2, for example, is inversely associated with heart disease in humans while intake of vitamin K1 is not,20 and vitamin K2 is at least three times more effective than vitamin K1 at activating proteins related to skeletal metabolism.32 This nutritional superiority makes it clear why the primitive groups that Weston Price studied expended so much effort procuring foods rich in vitamin K2 like the organs and fats of animals and the deeply colored orange butter from animals grazing on rich pastures.
Humans appear to have a finite ability to absorb vitamin K1 from plant foods. In the United States, where the mean intake of vitamin K1 is less than 150 micrograms per day, blood levels increase with increasing dietary intake until the latter reaches two hundred micrograms per day, after which they plateau. In the Netherlands, where the mean intake of vitamin K1 is much higher (250 micrograms per day), plasma levels of vitamin K1 have no relationship to dietary intake at all.24 These results suggest that humans do not possess the ability to absorb much more than 200 micrograms of vitamin K1 per day from vegetables.
This interpretation is also supported by feeding experiments. Whereas the absorption of vitamin K2 from natto, a fermented soy food, is nearly complete, the absorption of vitamin K1 from servings of green vegetables ranging from two hundred to four hundred grams consumed without added fat is only between five and ten percent. The absorption of similarly sized servings of vegetables with added fat is still only between ten and fifteen percent.25-26 By contrast, smaller servings are absorbed more efficiently. For example, the absorption from a 150-gram serving of spinach is 17 percent and the absorption from a 50-gram serving of spinach is 28 percent.27 These results show that our absorption of the vitamin declines as the amount we consume increases and strengthens the interpretation that we might only be able to absorb about 200 micrograms per day. When study subjects consume a highly absorbable pharmacological preparation of vitamin K1, a dose of 1000 micrograms per day is required to maximize the activation of proteins important to bone metabolism.28 If we can only absorb one-fifth of this amount from vegetables, we cannot support our skeletal system with vitamin K1 regardless of how efficiently we may be able to convert it to vitamin K2.
The ability to convert K1 to K2 varies widely between species and breeds of animals. The German researchers who first reported this conversion found that rats made it poorly compared to birds and that pigeons made it most efficiently.14 Every tissue tested in male Wistar rats is capable of making the conversion,15 whereas the liver, kidneys and heart of male Lewis rats will preferentially accumulate preformed K2, but, unlike the pancreas and testes of these same animals, will not synthesize it from K1.16 The K2 content of human breast milk increases when mothers consume pharmacological preparations of K1, but the K2 content of their blood does not;17 since the conversion takes place in the target tissues rather than the blood, however, we do not know how efficiently other human tissues make this conversion.
Vitamins K1 and K2 share a common ring-structured nucleus but possess different types of side chains. The first step in the conversion of K1 to K2 appears to be the cleavage of its side chain in either the liver or the gastrointestinal tract, yielding a toxic oxidizing agent called menadione; much of this metabolite is detoxified by the liver and excreted in the urine, while the remaining portion can be used to synthesize K2 in tissues.29 After this cleavage takes place, menadione must be transported to its target tissues where cellular enzymes can add a side chain to it, completing the transformation to K2. Because they are transported in different types of lipoproteins, vitamin K1 is primarily sent to the liver, whereas vitamin K2 is primarily sent to the other tissues;30 we know very little, however, about the transport of menadione in the blood. We also know very little about the rate at which our cells are capable of adding side chains to these molecules; presumably, if the supply of menadione exceeds the rate at which the cell can add these side chains, the menadione will exert toxic effects and cause oxidative damage within the cell. Preliminary evidence indicates that doses of 1000 micrograms per day of supplemental K1 may contribute to periodontal disease,31 suggesting that our bodies’ resistance to absorbing this much K1 from vegetables may serve an important purpose.
The clearest demonstration that humans require dietary preformed vitamin K2 for optimal health is that epidemiological and intervention studies both show its superiority over K1. Intake of vitamin K2, for example, is inversely associated with heart disease in humans while intake of vitamin K1 is not,20 and vitamin K2 is at least three times more effective than vitamin K1 at activating proteins related to skeletal metabolism.32 This nutritional superiority makes it clear why the primitive groups that Weston Price studied expended so much effort procuring foods rich in vitamin K2 like the organs and fats of animals and the deeply colored orange butter from animals grazing on rich pastures.
The Vitamin K-Dependent Carboxylase
Most known
functions of the K vitamins are mediated by the vitamin K-dependent
carboxylase. The carboxylase is an enzyme bound to the membrane of the
endoplasmic reticulum, a cellular organelle involved in the synthesis and
modification of proteins. It uses vitamin K as a cofactor to add carboxyl
groups to the side chains of the amino acid glutamate within certain vitamin
K-dependent proteins (see
Figure 3). This gives them a negative charge, allowing them to bind to
calcium, which carries a positive charge.40
Vitamin K-dependent proteins must be carboxylated before they leave the cell or insert themselves into its membrane. They may contain anywhere from three to thirteen glutamate residues (amino acids are called “residues” when they are bound up within proteins) that must be carboxylated; the carboxylase binds to them only once, however, and carboxylates each of these before it releases the protein. On the other hand, vitamin K can only be used for the carboxylation of a single glutamate residue and the carboxylase must release it after each carboxylation and allow it to be recycled and returned. A different enzyme, vitamin K oxidoreductase, recycles the vitamin; this enzyme is the target of the anticoagulant drug Warfarin and its relatives.40 Since Warfarin targets the recycling of vitamin K rather than the vitamin K-dependent coagulation proteins themselves, it not only acts as an anticoagulant, but also causes arterial and aortic valve calcification in both rats21 and humans41,42 and inhibits the mineralization of bone matrix.35
The distribution of the carboxylase among species and among tissues within an organism can help us understand its significance and that of its cofactor, vitamin K. With the exception of some microorganisms that have “stolen” the enzyme by incorporating the genetic material of other species,43 the carboxylase is present only in multicellular animals, underscoring its importance to intercellular communication. In the growing embryo, it is first expressed in skeletal and nervous tissue; vitamin K is therefore almost certainly essential to the development of the skeletal and nervous systems from their very beginnings.40
Vitamin K’s activity as a cofactor for the carboxylase may only be the tip of the iceberg. In osteoblasts, the cells responsible for bone growth, the greatest concentration of vitamin K2 exists in the nucleus where the genetic material is; the second greatest concentration exists in the mitochondria, the so-called “power house” of the cell; finally, only the third greatest concentration exists in the endoplasmic reticulum where the carboxylase is found.44 We do not currently have enough information to understand the role of the K vitamins in the mitochondria or the nucleus. Osteoblasts possess a nuclear receptor for vitamin K2, suggesting it has a role as a nuclear hormone. Vitamin K2 has a higher affinity than vitamin K1 both for the nuclear receptor44 and for the mitochondrial membrane.45 There is also evidence that vitamin K2 plays a role as an antioxidant within the cells that synthesize the myelin sheath, which forms the electrical insulation of nerves.46 Although it took until the 1970s to define the function of vitamin K as a cofactor for the carboxylase enzyme, the twenty-first century may well ring in a new revolution in our understanding of this amazing vitamin with the recognition that it is, to modify a phrase coined by Tufts University’s Dr. Sarah Booth, “not just for the carboxylase anymore.”
Vitamin K-dependent proteins must be carboxylated before they leave the cell or insert themselves into its membrane. They may contain anywhere from three to thirteen glutamate residues (amino acids are called “residues” when they are bound up within proteins) that must be carboxylated; the carboxylase binds to them only once, however, and carboxylates each of these before it releases the protein. On the other hand, vitamin K can only be used for the carboxylation of a single glutamate residue and the carboxylase must release it after each carboxylation and allow it to be recycled and returned. A different enzyme, vitamin K oxidoreductase, recycles the vitamin; this enzyme is the target of the anticoagulant drug Warfarin and its relatives.40 Since Warfarin targets the recycling of vitamin K rather than the vitamin K-dependent coagulation proteins themselves, it not only acts as an anticoagulant, but also causes arterial and aortic valve calcification in both rats21 and humans41,42 and inhibits the mineralization of bone matrix.35
The distribution of the carboxylase among species and among tissues within an organism can help us understand its significance and that of its cofactor, vitamin K. With the exception of some microorganisms that have “stolen” the enzyme by incorporating the genetic material of other species,43 the carboxylase is present only in multicellular animals, underscoring its importance to intercellular communication. In the growing embryo, it is first expressed in skeletal and nervous tissue; vitamin K is therefore almost certainly essential to the development of the skeletal and nervous systems from their very beginnings.40
Vitamin K’s activity as a cofactor for the carboxylase may only be the tip of the iceberg. In osteoblasts, the cells responsible for bone growth, the greatest concentration of vitamin K2 exists in the nucleus where the genetic material is; the second greatest concentration exists in the mitochondria, the so-called “power house” of the cell; finally, only the third greatest concentration exists in the endoplasmic reticulum where the carboxylase is found.44 We do not currently have enough information to understand the role of the K vitamins in the mitochondria or the nucleus. Osteoblasts possess a nuclear receptor for vitamin K2, suggesting it has a role as a nuclear hormone. Vitamin K2 has a higher affinity than vitamin K1 both for the nuclear receptor44 and for the mitochondrial membrane.45 There is also evidence that vitamin K2 plays a role as an antioxidant within the cells that synthesize the myelin sheath, which forms the electrical insulation of nerves.46 Although it took until the 1970s to define the function of vitamin K as a cofactor for the carboxylase enzyme, the twenty-first century may well ring in a new revolution in our understanding of this amazing vitamin with the recognition that it is, to modify a phrase coined by Tufts University’s Dr. Sarah Booth, “not just for the carboxylase anymore.”
Vitamin K2 and the Brain: A Closer Look
The
concentration of vitamin K2 is higher in myelinated regions than in
non-myelinated regions of the brain (myelin is the sheath that forms the
electrical insulation of neurons) and it is correlated with the presence of
important lipids such as sphingomyelin and sulfatides. The small amount of K1,
by contrast, is distributed more randomly,73 suggesting that it may
not be as functionally important. These lipids are part of a broader class of
compounds called sphingolipids that play essential roles in the brain as
structural constituents of membranes, signaling factors, and promoters of cell
survival. Vitamin K2 supports the activity of the enzyme that
catalyzes the initial reaction for the production of all sphingolipids as well
as the enzyme that catalyzes the final step in the synthesis of sulfatides.
Warfarin or dietary vitamin K deficiency cause marked decreases in the
activities of these enzymes and of the levels of sulfatides in the brains of
rats and mice, while the administration of either vitamin K1 or K2
restores them.46
In addition to the production of sulfatides and other sphingolipids, vitamin K2 plays at least two other important roles in the brain. The vitamin K-dependent protein gas6 promotes the survival of brain cells,74 and K vitamins, by an unknown mechanism, completely protect against the free radical-mediated death of the cells that synthesize myelin. Both an excess of glutamate and a deficiency of cystine can cause this type of cell death. Although K1 and K2 protect against glutamate toxicity equally, K2 is fifteen times more effective than K1 at counteracting the harmful effects of cystine depletion. Oxidative stress in the vulnerable infant brain can cause mental retardation, seizures, and cerebral palsy. Adequate intake of vitamin K2 during infancy may therefore protect against these diseases.75
In addition to the production of sulfatides and other sphingolipids, vitamin K2 plays at least two other important roles in the brain. The vitamin K-dependent protein gas6 promotes the survival of brain cells,74 and K vitamins, by an unknown mechanism, completely protect against the free radical-mediated death of the cells that synthesize myelin. Both an excess of glutamate and a deficiency of cystine can cause this type of cell death. Although K1 and K2 protect against glutamate toxicity equally, K2 is fifteen times more effective than K1 at counteracting the harmful effects of cystine depletion. Oxidative stress in the vulnerable infant brain can cause mental retardation, seizures, and cerebral palsy. Adequate intake of vitamin K2 during infancy may therefore protect against these diseases.75
Bacterial Production of Vitamin K2
“Vitamin K2”
actually refers to a group of compounds called menaquinones. While vitamins K1
and K2 have different types of side chains, the side chains of the
various menaquinones within the K2 group are all of the same type
but are of varying lengths. Each of these forms is abbreviated MK-n, where “n”
is a number that denotes the length of the side chain. Animal tissues
exclusively synthesize MK-4, but many anaerobic bacteria synthesize other
menaquinones, which they use for energy production much in the way that plants
use vitamin K1.80 We can therefore obtain vitamin K2
by absorbing that which is produced by our intestinal flora or by eating
fermented foods, in addition to eating animal foods which contain vitamin K2
synthesized from vitamin K1 found in grass.
Lactic acid bacteria mostly produce MK-7 through MK-10,18 while MK-10 and MK-11 accumulate in the human liver over time, presumably originating from bacterial production in the gut.81 It was once thought that intestinal bacteria were a major contributor to vitamin K status: the menaquinone content of stools is high, antibiotics have been associated with defects in blood clotting that resolve with vitamin K supplementation, and autopsies show that the great majority of vitamin K in the liver is present as “higher” menaquinones of bacterial origin. The balance of the evidence, however, challenges this view. Most of the menaquinones produced in the intestine are embedded within bacterial membranes and unavailable for absorption. Antibiotics produce vitamin K-responsive clotting defects not by reducing the intestinal production of K vitamins, but by inhibiting the enzyme within the human body that recycles them. Finally, the liver appears to accumulate higher menaquinones not because it is supplied with them abundantly but because it does not use them efficiently. Intestinal production of menaquinones therefore likely makes some contribution to vitamin K status, but one that is very small.80
Fermented foods such as sauerkraut, cheese, and natto, a soy dish popular in Eastern Japan, contain substantial amounts of vitamin K2. Natto, in fact, contains the highest amount of any food measured; nearly all of it is present as MK-7.26 MK-7 is highly effective: one recent study showed that it increased the percentage of activated osteocalcin in humans three times more powerfully than did vitamin K1.32 There are no studies available, however, comparing the efficacy of MK-7 to that of the MK-4 found in animal products. MK-9, and presumably MK-7, stays in the blood for a longer period of time than does MK-4, but this appears to be because tissues take up MK-4 much more rapidly.30 Whether the rapid uptake of MK-4 or the longer time spent in the blood by bacterial menaquinones have particular benefits or drawbacks is unclear. Future research will have to clarify whether the vitamin K2 synthesized by animal tissues and by bacteria are interchangeable, whether one is superior to the other, or whether each presents its own unique value to our health.
Lactic acid bacteria mostly produce MK-7 through MK-10,18 while MK-10 and MK-11 accumulate in the human liver over time, presumably originating from bacterial production in the gut.81 It was once thought that intestinal bacteria were a major contributor to vitamin K status: the menaquinone content of stools is high, antibiotics have been associated with defects in blood clotting that resolve with vitamin K supplementation, and autopsies show that the great majority of vitamin K in the liver is present as “higher” menaquinones of bacterial origin. The balance of the evidence, however, challenges this view. Most of the menaquinones produced in the intestine are embedded within bacterial membranes and unavailable for absorption. Antibiotics produce vitamin K-responsive clotting defects not by reducing the intestinal production of K vitamins, but by inhibiting the enzyme within the human body that recycles them. Finally, the liver appears to accumulate higher menaquinones not because it is supplied with them abundantly but because it does not use them efficiently. Intestinal production of menaquinones therefore likely makes some contribution to vitamin K status, but one that is very small.80
Fermented foods such as sauerkraut, cheese, and natto, a soy dish popular in Eastern Japan, contain substantial amounts of vitamin K2. Natto, in fact, contains the highest amount of any food measured; nearly all of it is present as MK-7.26 MK-7 is highly effective: one recent study showed that it increased the percentage of activated osteocalcin in humans three times more powerfully than did vitamin K1.32 There are no studies available, however, comparing the efficacy of MK-7 to that of the MK-4 found in animal products. MK-9, and presumably MK-7, stays in the blood for a longer period of time than does MK-4, but this appears to be because tissues take up MK-4 much more rapidly.30 Whether the rapid uptake of MK-4 or the longer time spent in the blood by bacterial menaquinones have particular benefits or drawbacks is unclear. Future research will have to clarify whether the vitamin K2 synthesized by animal tissues and by bacteria are interchangeable, whether one is superior to the other, or whether each presents its own unique value to our health.
Supplementing with Vitamin K2
The best
sources of vitamin K2 are fermented foods and grass-fed animal
fats. These foods contain a wide array of nutrients that may act
synergistically with vitamin K2 in ways we do not yet understand.
Price ‘s vitamin-rich butter and butter oil concentrate provided not only
vitamin K2 but also vitamin E, vitamin A, vitamin D, conjugated
linoleic acid (CLA) and other nutrients. Nevertheless, some people may wish to
supplement with vitamin K2 if they do not have access to high-quality
food, wish to use a higher dose to treat a health condition, or want extra
insurance.
Two forms of vitamin K2 supplements are commercially available: menaquinone-4 (MK-4), also called menatetrenone, and menaquinone-7 (MK-7). MK-4 is a synthetic product that is believed to be chemically and physiologically identical to the vitamin K2 found in animal fats. This form has been used in most of the animal experiments and in the Japanese osteoporosis studies. Although synthetic, it is effective, and there is no known toxicity. MK-7 is a natural extract of natto, a fermented soy food popular in Eastern Japan. MK-4 is much less expensive than MK-7, but no studies have yet compared the efficacy of these two forms.
Menaquinone-4 Supplements: Thorne Research and Carlson Laboratories both offer cost-effective MK-4 supplements. Thorne’s product is a liquid supplement. The MK-4 is dissolved in a medium-chain triglyceride base (the fats found in coconut oil) with mixed tocopherols (vitamin E). Carlson’s product is less expensive than Thorne’s, but comes in dry capsules primarily composed of cellulose and other fillers, and allows the user less control over the dose.
Menaquinone-7 Supplements: Jarrow Formulas and Source Naturals both offer cost-effective MK-7 supplements. Source Naturals’ product is less expensive, but Jarrow’s contains fewer additives and certifies that the soy used to make the product is not genetically modified. Vitamin K2 supplements interfere with the activity of oral anticoagulants such as warfarin. Patients who are using warfarin should only use vitamin K2 supplements with the knowledge of the prescribing physician.
Two forms of vitamin K2 supplements are commercially available: menaquinone-4 (MK-4), also called menatetrenone, and menaquinone-7 (MK-7). MK-4 is a synthetic product that is believed to be chemically and physiologically identical to the vitamin K2 found in animal fats. This form has been used in most of the animal experiments and in the Japanese osteoporosis studies. Although synthetic, it is effective, and there is no known toxicity. MK-7 is a natural extract of natto, a fermented soy food popular in Eastern Japan. MK-4 is much less expensive than MK-7, but no studies have yet compared the efficacy of these two forms.
Menaquinone-4 Supplements: Thorne Research and Carlson Laboratories both offer cost-effective MK-4 supplements. Thorne’s product is a liquid supplement. The MK-4 is dissolved in a medium-chain triglyceride base (the fats found in coconut oil) with mixed tocopherols (vitamin E). Carlson’s product is less expensive than Thorne’s, but comes in dry capsules primarily composed of cellulose and other fillers, and allows the user less control over the dose.
Menaquinone-7 Supplements: Jarrow Formulas and Source Naturals both offer cost-effective MK-7 supplements. Source Naturals’ product is less expensive, but Jarrow’s contains fewer additives and certifies that the soy used to make the product is not genetically modified. Vitamin K2 supplements interfere with the activity of oral anticoagulants such as warfarin. Patients who are using warfarin should only use vitamin K2 supplements with the knowledge of the prescribing physician.
- Price, Weston A. Nutrition and Physical Degeneration. Self-published, 1945.
- Lee, Royal. “Butter, Vitamin E and the ‘X’ Factor of Dr. Price.” In The Dr. Royal Lee Historical Archive Collection from Selene River Press. Not Dated. http://www.seleneriverpress.com/media/pdf_docs/39_butter.pdf Accessed February 5, 2006.
- Bland, Jeffrey. “Combating Cardiovascular Disease: The Search for Dr. Weston Price’s Factor X.” Price-Pottenger Nutrition Foundation. 1980; 5(1).
- Baggio B. Fatty acids, calcium and bone metabolism. J Nephrol. 2002; 15: 601-604.
- Price Pottenger Nutrition Foundation, personal communication.
- Whitney NJ, Mortimore CG. Isolation of the antifungal substance, 6-methoxybenzoxazolinone, from field corn (Zeamays L.) in Canada. Nature. 1959; 184(Suppl 17): 1320.
- Sweat FW, Berger PJ. Uterotropic 6-methoxybenzoxazolinone is an adrenergic agonist and a melatonin analog. Moll Cell endocrinol. 1988; 57(1-2): 131-8.
- Yoder L. The relation between peroxidation and antirachitic vitamin. J Biol Chem. 1926; 70(1): 297-307.
- Mair RD, Graupner J. Determination of Organic Peroxides by Iodine Liberation Procedures. Anal Chem. 1964; 36(1): 194-203.
- Willstatter R, Majima R. Über die quantitative Bestimmung der Chinone. Zurch-Ber. 1910; 43: 1171-1175.
- Malyshev AI, Iofe II. Potentiometric titration of benzoquinone in maleic acid solutions. J Anal Chem USSR (Engl Trans). 1958; 13: 427-429.
- Glavind J. On the existence of lipid peroxides in rat tissue. Br J Nutr. 1972; 27: 19-26.
- Chitnis PR. Photosystem I: Function and Physiology. Annu Rev Plant Physiol Plant Mol Biol. 2001; 52: 593-626.
- Billeter M, Martius C. Über die Umwandlung von Phyllochinon (Vitamin K1) in Vitamin K2(20) im Tierkörper. Biochem Z. 1960; 333: 430-439.
- Thijssen HHW, Drittij-Reijnders MJ. Vitamin K distribution in rat tissues: dietary phylloquinone is a source of tissue menquinone-4. Br J Nutr. 1994; 72: 415-425.
- Ronden JE, Thijssen HHW, Vermeer C. Tissue distribution of K-vitamins under different nutritional regimens in the rat. Biochim Biophys Acta. 1998; 1379: 16-22.
- Thijssen HHW, Drittij M-J, Vermeer C, Schoffelen E. Menaquinone-4 in breast milk is derived from dietary phylloquinone. Br J Nutr. 2002; 87: 219-226.
- Morishita T, Natsuko T, Makino T, Kudo S. Production of Menaquinones by Lactic Acid Bacteria. J Dairy Sci. 1999; 82: 1897-1903.
- Vermeer C, Hamulyak K. Vitamin K: lessons from the past. J Thromb Haemost. 2004; 2(12): 2115-7.
- Geleijnse JM, Vermeer C, Grobbee DE, Schurgers LJ, Knapen MHJ, van der Meer IM, Hofman A, Witteman JCM. Dietary Intake of Menaquinone Is Associated with a Reduced Risk of Coronary Heart Disease: The Rotterdam Study. J Nutr. 2004; 134: 3100-3105.
- Spronk HMH, Soute BAM, Schurgers LJ, Thijssen HHW, De Mey JGR, Vermeer C. Tissue-Specific Utilization of Menaquinone-4 Results in the Prevention of Arterial Calcification in Warfarin-Treated Rats. J Vasc Res. 2003; 40: 531-537.
- Elder SJ, Haytowitz DB, Howe J, Peterson JW, Booth SL. Vitamin K Contents of Meat, Dairy, and Fast Food in the U.S. Diet. J Agric Food Chem. 2006; 54: 463-467.
- Buitenhuis HC, Soute BAM, Vermeer C. Comparison of the vitamins K1, K2 and K3 as cofactors for the hepatic vitamin K-dependent carboxylase. Biochim Biophys Acta. 1990; 1034: 170-175.
- McKeown NM, Jacques PF, Gundberg CM, Peterson JW, Tucker KL, Kiel KP, Wilson PWF, Booth SL. Dietary and nondietary determinants of vitamin K biochemical measures in men and women. J Nutr. 2002; 132(6): 1329-1334.
- Gijsbers BLMG, Jie K-SG, Vermeer C. Effect of food composition on vitamin K absorption in human volunteers. Br J Nutr. 1996; 76: 223-229.
- Schurgers LJ, Vermeer C. Determination of Phylloquinone and Menaquinones in Food. Haemostasis. 2000; 30: 298-307.
- Garber AK, Binkley NC, Krueger DC, Suttie JW. Comparison of Phylloquinone Bioavailability from Food Sources or a Supplement in Human Subjects. J Nutr. 1999; 129: 1201-1203.
- Binkley NC, Grueger DC, Kawahara TN, Engelke JA, Chappell RJ, Suttie JW. A high phylloquinone intake is required to achieve maximal osteocalcin gamma-carboxylation. Am J Clin Nutr. 2002; 76: 1055-60.
- Thijssen HHW, Vervoot LMT, Schurgers LJ, Shearer MJ. Menadione is a metabolite of oral vitamin K. Br J Nutr. 2006; 95: 266.
- Schurgers LJ, Vermeer C. Differential lipoprotein transport pathways of K-vitamins in healthy subjects. Biochim Biophys Acta. 2002; 1570: 27-32.
- Vermeer C, Shearer MJ, Zittermann A, Bolton-Smith C, Szulc P, Hodges S, Walter P, Rambeck W, Stocklin E, Weber P. Beyond deficiency: potential benefits of increased intakes of vitamin K for bone and vascular health. Eur J Nutr. 2004; 43: 325-335.
- Schurgers LJ, Teunissen KJF, Hamulyak K, Knapen MHJ, Hogne V, Vermeer C. Vitamin K-containing dietary supplements: comparison of synthetic vitamin K1 and natto-derived menaquinone-7. Blood. 2006; [Epub ahead of print].
- Berkner KL, Runge W. The physiology of vitamin K nutriture and vitamin K-dependent protein function in atherosclerosis. J Thromb Haemost. 2004; 2(12): 2118-32.
- Oliva A, Ragione FD, Fratta M, Marrone G, Palumbo R, Zappia V. Effect of retinoic acid on osteocalcin gene expression in human osteoblasts. Biochem Biophys Res Commun. 1993; 191(3): 908-14.
- Koshihara Y, Hoshi K. Vitamin K2 enhances osteocalcin accumulation in the extracellular matrix of human osteoblasts in vitro. J Bone Miner Res. 1997; 12(3): 431-8.
- Farzanheh-Far A, Weissberg PL, Proudfoot D, Shanahan CM. Transcriptional regulation of matrix gla protein. Z Kardiol. 2001; 90(Suppl. 3): 38-42.
- Kirfel J, Kelter M, Cancela LM, Price PA, Schule R. Identification of a novel negative retinoic acid responsive element in the promoter of the human matrix Gla protein gene. Proc Natl Acad Sci USA. 1997; 94(6): 2227-32.
- Luo G, Ducy P, McKee MD, Pinero GJ, Loyer E, Behringer RR, Karsenty G. Spontaneous calcification of arteries and cartilage in mice lacking matrix GLA protein. Nature. 1997; 386: 78-81.
- Masterjohn C. Vitamin D toxicity redefined: Vitamin K and the molecular mechanism. Med Hypotheses. 2006; [Epub ahead of print].
- Berkner KL. The Vitamin K-Dependent Carboxylase. Annu Rev Nutr. 2005; 25: 127-49.
- Schori TR, Stungis GE. Long-term warfarin treatment may induce arterial calcification in humans: case report. Clin Invest Med. 2004; 27(2): 107-9.
- Schurgers LJ, Aebert H, Vermeer C, Bultmann B, Janzen J. Oral anticoagulant treatment: friend or foe in cardiovascular disease? Blood. 2004; 104: 3231-3232.
- Rishavy MA, Hallgren KW, Yakubenko AV, Zuerner RL, Runge KW, Berkner KL. The vitamin K-dependent carboxylase has been acquired by Leptospira pathogens and shows altered activity that suggests a role other than protein carboxylation. J Biol Chem. 2005; 280(41): 34870-7.
- Hoshi K, Kohi N, Yoshihisa S, Koshihara Y. Nuclear Vitamin K2 Binding Protein in Human Osteoblasts. Homologue to Glyceraldehyde-3-Phosphate Dehydrogenase. Biochem Pharmacol. 1999; 58: 1631-1638.
- Konishi T, Baba S. Intracellular and Intramitochondrial Distribution of Vitamin K: Biochemical and Electron Microscopic Radioautographic Study. Chem Pharm Bull. 1973; 21(1): 2479-2487.
- Denisova NA, Booth SL. Vitamin K and Sphingolipid Metabolism: Evidence to Date. Nutr Rev. 2005; 63(4): 110-121.
- Calandra JC, Fancher OE, Fosdick LS. The effect of synthetic vitamin K and related compounds on the rate of acid formation in saliva. J Dent Res. 1945; 24: 31-37.
- Armstrong WD, Knutson JW. Effect of Quinones on Acid Formation in Saliva. Proc Soc Exper Biol & Med. 1942; 52: 307-310.
- Burrill DY, Calandra JC, Tilden EB, Fosdick LS. The effect of 2-methyl-1,4-naphthoquinone on the incidence of dental caries. J Dent Res. 1945; 24: 273-282.
- Medical Department Professional Service Schools. Bull YS. Army Med Dept. 1946; 5: 265. As cited in Makila E. Salivary Vitamins. Internat. Z. Vit. Forschung. 1968; 38: 260-269.
- Gebauer H. Vitamin K als Cariesprophylaktikum. Dtsch Zahnarztl Z. 1955; 10(7): 555-6.
- Glavind J, Granados H, Hansen A, Schilling K, Kruse I, Dam H. The Presence of Vitamins in the Saliva. Internat Z Vit Forschung. 1948; 20: 234-237.
- Zacharski LR, Rosenstein R. Reduction of Salivary Tissue Factor (Thromboplastin) Activity by Warfarin Therapy. Blood. 1979; 53(3): 366-374.
- Huang GT-J, Shagramanova K, Chan SW. Formation of Odontoblast-Like Cells from Cultured Human Dental Pulp Cells on Dentin In Vitro. J Endod. 2006; 32: 1066-1073.
- Trueb B, Taeschler S, Schild C, Lang NP. Expression of phosphoproteins and amelotin in teeth. Int J Mol Med. 2007; 19: 49-54.
- Thaweboon S, Thaweboon B, Choonharuangdej S, Chunhabundit P, Suppakpatana P. Induction of type I collagen and osteocalcin in human dental pulp cells by retinoic acid. Southeast Asian J Trop Med Public Health. 2005; 36(4): 1066-9.
- Shiba H, Uchida Y, Kamihagi K, Sakata M, Fujita T, Nakamura S, Takemoto T, Kato Y, Kurihara H. Transforming Growth Factor-ß1 and Basic Fibroblast Growth Factor Modulate Osteocalcin and Osteonectin/SPARC Syntheses in Vitamin-D-activated pulp cells. J Dent Res. 2001; 80(7): 1653-1659.
- Rhode CM, DeLuca HF. All-trans Retinoic Acid Antagonizes the Action of Calciferol and Its Active Metabolite, 1,25-Dihydroxycholecalciferol, in Rats. J Nutr. 2005; 135: 1647-1652.
- Boskey AL, Gadaleta S, Gundberg C, Doty SB, Ducy P, Karsenty G. Fourier transform infrared microspectropic analysis of bones of osteocalcin-deficient mice provides insight into the function of osteocalcin. Bone. 1998; 23(3): 187-96.
- Luukinen H, Kakonen SM, Pettersson K, Koski K, Laippala P, Lovgren T, Kivela SL, Vaananen HK. Strong prediction of fractures among older adults by the ratio of carboxylated to total serum osteocalcin. J Bone Miner Res. 2000; 15(12): 2473-8.
- Cockayne S, Adamson J, Lanham-New S, Shearer MJ, Gilbody S, Torgerson DJ. Vitamin K and the Prevention of Fractures. Arch Intern Med. 2006; 166: 1256-1261.
- Konishi T, Baba S, Sone H. Whole-body Autoradiographic Study of Vitamin K Distribution in Rat. Chem Pharm Bull. 1973; 21(1): 220-224.
- Schurgers LJ, Teunissen KJF, Knapen MHJ, Kwaijtall M, van Diest R, Appels A, Reutelingsperger CP, Cleutjens JPM, Vermeer C. Novel Conformation-Specific Antibodies Against Matrix gamma-Carboxyglutamic Acid (Gla) Protein. Undercarboxylated Matrix Gla Protein as Marker for Vascular Calcification. Arterioscler Thromb Basc Biol. 2005; 25: 1629-1633.
- Thijssen HHW, Drittij-Reijnders MJ, Fischer MAJG. Phylloquinone and Menaquinone-4 Distribution in Rats: Synthesis rather than Uptake Determines Menaquinone-4 Organ Concentrations. J Nutr. 1996; 126: 537-543.
- Schurgers LJ, Spronk HMH, Soute BAM, Schiffers PM, DeMey JGR, Vermeer C. Regression of warfarin-induced medial elastocalcinosis by high intake of vitamin K in rats. Blood. 2006; [Epub ahead of print].
- Erkkila AT, Booth SL, Hu FB, Jacques PF, Manson JE, Rexrode KM, Stampfer MJ, Lichtenstein AH. Phylloquinone intake as a marker for coronary heart disease risk but not stroke in women. Eur J Clin Nutr. 2005; 59: 196-204.
- Erkkila AT, Booth SL, Hu FB, Jacques PF, Lichenstein AH. Phylloquinone intake and risk of cardiovascular diseases in men. Nutr Metab Cardiovasc Dis. 2007; 17: 58-62.
- Braam L, McKeown N, Jacques P, Lichtenstein A, Vermeer C, Wilson P, Booth S. Dietary Phylloquinone Intake as a Potential Marker for a Heart-Healthy Dietary Pattern in the Framingham Offspring Cohort. J Am Diet Assoc. 2004; 104: 1410-1414.
- Thijssen HHW, Drittij-Reijnders MJ. Vitamin K status in human tissues: tissue-specific accumulation of phylloquinone and menaquionone-4. Br J Nutr. 1996; 75: 121-127.
- Han X, M Holtzman D, McKeel DW Jr, Kelley J, Morris JC. Substantial sulfatide deficiency and ceramide elevation in very early Alzheimer’s disease: potential role in disease pathogenesis. J Neurochem. 2002; 82(4): 809-18.
- Cocchetto DM, Miller DB, Miller LL, Bjornsson TD. Behavioral perturbations in the vitamin K-deficient rat. Physiol Behav. 1985; 34(5): 727-34.
- Bosio A, Binzeck E, Stoffel W. Functional breakdown of the lipid bilayer of the myelin membrane in central and peripheral nervous system by disrupted galactocerebroside synthesis. Proc Natl Acad Sci USA. 1996; 93: 13280-13285.
- Carrie I, Portoukalian J, Vicaretti R, Rochford J, Potvin S, Ferland G. Menaquinone-4 Concentration is Correlated with Sphingolipid Concentrations in Rat Brain. J Nutr. 2004; 134: 167-172.
- Shankar SL, O’Guin K, Cammer M, McMorris FA, Stitt TN, Basch RS, Varnum B, Shafit-Zagardo B. The Growth Arrest-Specific Gene Product Gas6 Promotes the Survival of Human Oligodendrocytes via a Posphatidylinositol 3-Kinase-Dependent Pathway. J Neurosci. 2003; 23(10): 4208-4218.
- Li J, Lin JC, Wang H, Peterson JW, Furie BC, Furie B, Booth SL, Volpe JJ, Rosenberg PA. Novel Role of Vitamin K in Preventing Oxidative Injury to Developing Oligodendrocytes and Neurons. J Neurosci. 2003; 32(13): 5816-5826.
- Sakamoto N, Nishiike T, Iguchi H, Sakamoto K. Possible effects of one week vitamin K (menaquinone-4) tablets intake on glucose tolerance in healthy young male volunteers with different descarboxy prothrombin levels. Clin Nutr. 2000; 19(4): 259-263.
- Vermeer C, Soute BAM, Ulrich MMW, van de Loo PGF. Vitamin K and the Urogenital Tract. Haemostasis. 1986; 16: 246-257.
- Howe AM, Lipson AH, de Silva M, Ouvrier R, Webster WS. Severe Cervical Dysplasia and Nasal Cartilage Calcification Following Prenatal Warfarin Exposure. Am J Med Genet.1997; 71: 391-396.
- Tokita H, Tsuchida A, Miyazawa K, Ohyashiki K, Katayanaqi S, Sudo H, Enomoto M, Takaqi Y, Aoki T. Vitamin K2-induced antitumor effects via cell-cycle arrest and apoptosis in gastric cancer cell lines. Int J Mol Med. 2006; 17(2):2355-43.
- Unden G, Bongaerts J. Alternative respiratory pathways of Escherichia coli: energetics and transcriptional regulation in response to electron acceptors. Biochim Biophys Acta. 1997; 1320: 217-234.
- Suttie JW. The importance of menaquinones in human nutrition. Annu Rev Nutr. 1995; 15: 399-417.
Follow Up Questions and Answers
Question:
How much K2 is recommended for adults and for children?
Answer: Unfortunately we do not have any solid numbers on the optimal or minimum intake of K vitamins, neither from modern scientific analysis nor from what people consumed in optimal traditional diets. However, we do know that virtually all adults have some degree of deficiency, whether this is very small or very substantial, and a recent study suggests that children are much more likely to be deficient, so children may actually need more because they are growing. The best thing to do would be to eat from the foods richest in vitamin K2: natto, cheese or goose liver, at least once a week and to eat from the other relatively rich foods—grass-fed butter, animal fats and fermented foods—on a daily basis. If you choose to take any of the supplements listed in the article in addition to this, there is currently no reason to believe that it is necessary to take more than the minimum dose (one drop of Thorne or one capsule of Jarrow). In the years ahead, we should see much more definitive information coming out on this, and hopefully we will also see some research reopen the questions that Price had raised about the agricultural practices that lead to the highest levels of Activator X in foods.
Question: What is the appropriate dose of vitamin K2 for maintenance and therapeutic purposes?
Answer: We do not have adequate information on dosage requirements for vitamin K2. I would think that for maintenance one should shoot for 100 mcg minimum, possibly more for children, but we will have to wait for further research to quantify this. There are unpublished anecdotes according to which some people have found up to 5-10 milligrams useful for treating specific conditions, such as autism or spider veins. At present, this is a matter that the individual must settle through experimentation.
Question: Do we know the levels of vitamin K2 in the primitive societies studied by Dr. Price?
Answer: We have no quantitative information on K2 as K2 or as Activator X in primitive societies or in Price’s practice because Price did not have a means of quantifying the levels by mass—for example, how many micrograms were contained in a given food sample. Price could only compare different foods based on the intensity of the blue color yielded by the test, which he then compared to standards made from numerous different dilutions of a blue dye. So Price could say that one food was a richer or poorer source than another, but he could not determine the precise amount contained within the food.
Question: Is the K2 found in animal products or fermented foods affected by cooking?
Answer: I have yet to see any hard data on cooking losses, but everything I have read indicates that vitamin K is very heat-stable (though it can apparently incur losses from exposure to light).
Question: Is the Wulzen anti-arthritis factor in butter a separate compound from K2?
Answer: I do not know whether the Wulzen factor is a separate compound; however, others have suggested that they are separate because Wulzen found this factor to be destroyed by pasteurization, whereas Price and maybe others found activator X to be heat-stable.
Question: Fermented foods are said to be good sources of K2 but in your article you say that most of the vitamin K2 produced by bacteria in the gut is now believed to be embedded in the bacterial membranes and unavailable for absorption. One might think therefore that the vitamin K2 produced in fermented foods is similarly unavailable. Are the bacteria in fermented foods different? Does stomach digestion free up the K2?
Answer: Whether it is because some bacteria secrete the K2 or because the acidic digestion of the stomach ruptures the membranes I do not know, but the absorption of K2 from natto is near complete.
Question: Does yogurt contain vitamin K2?
Answer: Yogurt has roughly the same amount of K2 as milk, with just a tiny bit produced. This is probably because commercial yogurt is only fermented for four hours, whereas hard cheese is fermented for at least two months.
Question: Can you calculate how much K2 is in commercial versus grass-fed butter?
Answer: I do not think this can be calculated. The primary confounder is that commercial butter comes from cows in confinement operations fed massive amounts of menadione, a portion of which can be converted into K2. We have no idea at what rate this is turned into K2 and how it compares to K1 from grass as a precursor to K2, so we have no baseline from which to calculate.
Question: I’d like to use natto as a source of K2, but I have an allergy to yeast. Do you know which microorganisms ferment soy to create natto, and whether yeast is used in other parts of the process?
Answer: Natto is fermented with Bacillus subtilus, subspecies natto. Yeast is not essential to the process as far as I know, but I do not know whether the cultures tend to pick up yeast or whether for some reason some products may also deliberately use yeast. You may want to inquire with a specific manufacturer or from whomever you buy the culture if you choose to make your own.
Editor’s note: Natto is definitely an acquired taste, one usually not acceptable to westerners.
Answer: Unfortunately we do not have any solid numbers on the optimal or minimum intake of K vitamins, neither from modern scientific analysis nor from what people consumed in optimal traditional diets. However, we do know that virtually all adults have some degree of deficiency, whether this is very small or very substantial, and a recent study suggests that children are much more likely to be deficient, so children may actually need more because they are growing. The best thing to do would be to eat from the foods richest in vitamin K2: natto, cheese or goose liver, at least once a week and to eat from the other relatively rich foods—grass-fed butter, animal fats and fermented foods—on a daily basis. If you choose to take any of the supplements listed in the article in addition to this, there is currently no reason to believe that it is necessary to take more than the minimum dose (one drop of Thorne or one capsule of Jarrow). In the years ahead, we should see much more definitive information coming out on this, and hopefully we will also see some research reopen the questions that Price had raised about the agricultural practices that lead to the highest levels of Activator X in foods.
Question: What is the appropriate dose of vitamin K2 for maintenance and therapeutic purposes?
Answer: We do not have adequate information on dosage requirements for vitamin K2. I would think that for maintenance one should shoot for 100 mcg minimum, possibly more for children, but we will have to wait for further research to quantify this. There are unpublished anecdotes according to which some people have found up to 5-10 milligrams useful for treating specific conditions, such as autism or spider veins. At present, this is a matter that the individual must settle through experimentation.
Question: Do we know the levels of vitamin K2 in the primitive societies studied by Dr. Price?
Answer: We have no quantitative information on K2 as K2 or as Activator X in primitive societies or in Price’s practice because Price did not have a means of quantifying the levels by mass—for example, how many micrograms were contained in a given food sample. Price could only compare different foods based on the intensity of the blue color yielded by the test, which he then compared to standards made from numerous different dilutions of a blue dye. So Price could say that one food was a richer or poorer source than another, but he could not determine the precise amount contained within the food.
Question: Is the K2 found in animal products or fermented foods affected by cooking?
Answer: I have yet to see any hard data on cooking losses, but everything I have read indicates that vitamin K is very heat-stable (though it can apparently incur losses from exposure to light).
Question: Is the Wulzen anti-arthritis factor in butter a separate compound from K2?
Answer: I do not know whether the Wulzen factor is a separate compound; however, others have suggested that they are separate because Wulzen found this factor to be destroyed by pasteurization, whereas Price and maybe others found activator X to be heat-stable.
Question: Fermented foods are said to be good sources of K2 but in your article you say that most of the vitamin K2 produced by bacteria in the gut is now believed to be embedded in the bacterial membranes and unavailable for absorption. One might think therefore that the vitamin K2 produced in fermented foods is similarly unavailable. Are the bacteria in fermented foods different? Does stomach digestion free up the K2?
Answer: Whether it is because some bacteria secrete the K2 or because the acidic digestion of the stomach ruptures the membranes I do not know, but the absorption of K2 from natto is near complete.
Question: Does yogurt contain vitamin K2?
Answer: Yogurt has roughly the same amount of K2 as milk, with just a tiny bit produced. This is probably because commercial yogurt is only fermented for four hours, whereas hard cheese is fermented for at least two months.
Question: Can you calculate how much K2 is in commercial versus grass-fed butter?
Answer: I do not think this can be calculated. The primary confounder is that commercial butter comes from cows in confinement operations fed massive amounts of menadione, a portion of which can be converted into K2. We have no idea at what rate this is turned into K2 and how it compares to K1 from grass as a precursor to K2, so we have no baseline from which to calculate.
Question: I’d like to use natto as a source of K2, but I have an allergy to yeast. Do you know which microorganisms ferment soy to create natto, and whether yeast is used in other parts of the process?
Answer: Natto is fermented with Bacillus subtilus, subspecies natto. Yeast is not essential to the process as far as I know, but I do not know whether the cultures tend to pick up yeast or whether for some reason some products may also deliberately use yeast. You may want to inquire with a specific manufacturer or from whomever you buy the culture if you choose to make your own.
Editor’s note: Natto is definitely an acquired taste, one usually not acceptable to westerners.
Posted by Baldwin Templeton at
2:29
AM
No comments:
Post a Comment