The Forgotten History of Neurological Vaccine InjuriesCrippling brain injuries used to be a well recognized complication of vaccination. What changed?Story at a Glance: •One of the most frequent complications of vaccination is neurological injury, and ever since the smallpox vaccine hit the market over a century ago, severe and unusual injuries have been reported throughout the medical literature. •Rather than disclose these injuries to the public, the medical profession chose to conceal them under the erroneous belief that the public good of vaccination justified hiding anything which would create vaccine hesitancy—a cruel mentality that is still used to push unsafe and ineffective vaccines. •Many of those injuries such as a spreading paralysis of the body mirror the “one in a million” injuries we still see from vaccination but to preserve the mythology of vaccines being “safe and effective” centuries of vaccine toxicity was erased from memory, thereby allowing the same vaccine disasters to keep repeating. •These concerns peaked in the 1980s, leading to widespread attention on the harms of vaccination and the enactment of a Federal law to prevent these neurological injuries. To protect the industry, its key provisions were all deliberately violated, and the injuries it recognized (e.g., severe brain damage) were renamed so they could be swept under the rug. •In tandem, widespread censorship was enacted, with both the media and medical journals refusing to publish further reports of injury, thereby creating a societal illusion that these injuries were rare to non-existent. •Thanks to the MAHA moment, we have a once in a lifetime opportunity to change this dysfunctional paradigm. This article will hence review those forgotten injuries and exactly what caused them, as without that knowledge, these injuries will continue to repeat, and those injured will continue to suffer in silence while being told their injuries are “extremely rare” or “not linked to vaccination” rather than receiving the help they need. From birth, we are taught that vaccines were one of the most remarkable discoveries in history, and were so safe and effective that many now unimaginable plagues vanished with few to no side effects occurring in the process. In truth, give or take every part of that mythology is false and because it has never been dispelled, remarkably similar vaccine disasters occur every few decades. Much of this results from the fact that it is very difficult to make safe vaccines due to both how they work and how they are produced. As such, the best “solution” which could be found to this problem was to insist in lockstep that vaccines were safe and erase any memory that vaccine disasters had in fact occurred, thereby making it possible to gaslight anyone who was severely injured by a vaccine and claim their injury was just anecdotal or a product of anti-vaccine hysteria. For example, recently I discussed how vaccines cause autism, and focused on a central argument used to debunk the link between the two—that the only reason people believe vaccines cause autism is because a disgraced British doctor published a fraudulent 1998 study claiming they did and then made everyone start hallucinating that vaccine injuries were occurring. This mythology however, ignores that brain injuries were a longstanding problem of vaccination. For example, this 1982 NBC news program revealed that many parents were having children develop “post-pertussis encephalopathy” after taking the DPT vaccine, that most doctors refused to report this, and that:
Likewise, in 1985, one of the most popular talk shows in America (the Donahue show) hosted a segment where doctors from both sides (and neurologically injured members of the audience) debated the risks and benefits of vaccination and the ethics of mandates. To the best of my knowledge, this was the last time an open debate of vaccination aired on mainstream television, something I suspect was due to a recognition that allowing a public one would only increase vaccine skepticism due to how strong the evidence against vaccines was (e.g., Peter Hotez recently turned down 2.62 million to debate RFK Jr.). Diagnostic ObfuscationIn both of these 1980s TV programs and many of the earlier studies cited throughout this article, the vaccine brain damaged children were described as becoming “mentally retarded” or “severely retarded.” Likewise, a famous 1964 government film (fully intended to be compassionate) was titled “Introducing the Mentally Retarded.” In the mid to late 1990s, “retarded” began to be phased out due to it being deemed too stigmatizing, momentum gradually built to use less offensive terminology, and eventually, in 2010, Obama signed a law that replaced all instances in Federal statutes of “mentally retarded” “mental retardation” with “intellectual disability” (which is the only time a US law was passed that erased a word in such a targeted fashion). As such, this term is rarely used now, and you can get in trouble for uttering it out loud (although many doctors I know will informally use the phrase “MR” to explain the clinical situation of mentally disabled patients to colleagues). In turn, one of the classic tricks in propaganda is to constantly manipulate and redefine words so that it becomes possible for their client to justify contradictory and unjustifiable positions. In the case of autism, it is commonly argued that the increase in it is not due to an environmental toxin (e.g., vaccines) but rather more and more “normal” things being reclassified as autism. One of the primary studies that supported that argument, a 2009 study from California, indeed shows the reclassification occurred, but what it actually showed is that 26.4% of children who had previously been diagnosed as “mentally retarded” became “autistic” (as did another commonly cited study). Since autism is deliberately undefined, it encapsulates both profound (severe) autism (25-30% of cases) and autistic traits (e.g., having manageable neurological deficits or “being on the spectrum”). While there are certain traits shared between these two groups, they are very different (e.g., being nonverbal or minimally verbal, having intellectual disability, and requiring substantial lifelong support for daily living vs. being socially awkward with personality quirks or having high functioning autism like Elon Musk). A key point I’ve emphasized throughout this publication is that when most toxins harm people, the injuries distribute on a bell curve where more severe injuries are much rarer than less severe (and hard to spot) ones, so if you see a cluster of severe injuries, it tells you far more mild ones are hiding under the surface, and likewise that if you see many moderate injuries, more severe ones are present too. As such, of those with “autism” roughly 26.7% of children have “profound autism,” and likewise, while both have increased in tandem with increasing vaccination, per the CDC non-severe autism has increased at a faster rate.
This wordplay then leads to both being blended together to deflect any criticisms of severe autism (e.g., by attacking anyone who states severe autism is a “problem” by claiming that is stigmatizing to all the people with high-functioning autism) and to argue that any claims vaccines cause autism is actually due to the people with autism quirks being given an autism diagnosis (thereby removing the clear increase in severe autism from the debate). Likewise, having the softer label of autism (and pro-autism words like “neurodiverse” or “neurodivergent”) to encapsulate and normalize these injuries makes it much easier to keep the uncomfortable topic out of sight and mind for those who do not have to directly deal with the reality of these injuries (e.g., the parent of a child with severe autism). It hence prevents enough people from speaking out about the issue for something to be done. I mention all of this for two reasons: •We believe obfuscating these definitions was deliberately done to conceal the epidemic of vaccine injuries. •In much of the earlier literature, brain damage we now associate with “severe autism” was described but instead labeled with terms such as “mental retardation” or “encephalitis” or “encephalopathy.” Note: since I have a large audience, I feel I have a responsibility to use measured language that avoids unnecessarily harming others or inadvertently supporting malicious linguistic propaganda. At the same time, I detest this, in part because I deeply value personal liberty and hate having my language policed and in part because I feel using euphemisms to avoid overtly addressing uncomfortable topic has been responsible for an immense amount of carnage and suffering throughout human history (as critical topics that need to be widely understood to prevent a catastrophe aren’t because no one wants to directly describe them in an uncomfortable way that everyone can clearly understand). For a moment, imagine how different the entire vaccine discussion would be if people instead had simply said things like “vaccines can make you severely retarded” or “Bill’s son became mentally retarded after the shot Sue’s daughter had issues with” or “in just eight years, the number of severely retarded children doubled” rather than how it’s been obfuscated within the ambiguous “autism” label. Exempting Brain DamageThe 1986 Vaccine Injury Act was made in response to public pressure against vaccine injuries (e.g., the 1982 NBC program) and had numerous provisions intended to help parents of vaccine-injured children. One was that since DPT brain injury lawsuits were challenging (but possible) to win in court, a “no-fault” system funded by a tax on vaccines was created to replace them (which protected vaccine manufacturers from liability). For this system, a table of injuries was created through extensive negotiation when the law was passed. Then, if a child suffered an injury on the table shortly after vaccination, compensation was awarded, and friends who worked at the vaccine court have told me the program is very fair for individuals who have covered injuries. Finally, since it was recognized that new science and vaccines would emerge, the H.H.S. Secretary was given the authority to add new injuries to the table as science advanced. Unfortunately, in one way or another, most of the helpful provisions of the law were undermined. For example, since the Federal Government ultimately pays for these injuries, it incentivizes: •Never having the HHS Secretary add anything else to the schedule. At the time the original injury table was made, every vaccine on the schedule (excluding the inactivated polio vaccine) had covered injuries, most of which were neurological in nature:
Since that time twelve new vaccines were added to the schedule while all but MMR were replaced with alternative vaccines. However, if you look at the current table, despite nearly 40 years of “science” other than Guillain-Barré Syndrome from influenza, brachial neuritis from acellular DPT, and fainting within an hour of vaccination (from a few vaccines), no neurological injuries have been added to the table. As such: •The vast body of literature (which was well known in the 1980s) showing vaccines cause neurological damage became “forgotten.” •It became almost impossible to get compensation for a neurological injury. In fact, the only time a regressive autism case ever won compensation was in 2010 due to the father being a prestigious neurologist. There, the court concluded a cluster of vaccines (including MMR) “significantly aggravated an underlying mitochondrial disorder, which predisposed her to deficits in cellular energy metabolism, and manifested as a regressive encephalopathy with features of autism spectrum disorder.” •There was a strong incentive to remove the remaining covered brain injury (MMR’s encephalopathy) from colloquial use, replace it with non-compensable “autism” and then perpetually demonize anyone who claimed MMR caused autism (which is what happened to Andrew Wakefield). Note: Peter Marks, the head FDA official who relentlessly covered up all the reports of COVID vaccine injuries they were receiving and overrode the FDA’s top vaccine experts to rush a formal approval for it and the boosters (so the unconscionable mandates could be enacted) recently went on national television and made many false statement about MMR including that it “does not cause encephalitis.” Additionally, a systematic effort was made to prevent any further research into these neurological injuries from occurring or being published. For example, dogma was instilled that vaccines are so safe and effective that it’s “unethical” to conduct a placebo-controlled vaccine trial (as this would deny children a “lifesaving” vaccine), while simultaneously proclaiming all research showing the harms of vaccine injuries is “junk science” because that data does not have placebo controls. As such, in each case where researchers nonetheless conducted the science (e.g., by reviewing large numbers of patient charts) their data was blocked from publication, and in many cases the researchers were retaliated against (e.g., an Oregon pediatrician lost his medical license). As you might guess, those data sets (which I summarized here) all show a massive increase in common infectious, autoimmune, and neurological diseases of childhood. These for example, were the increases in neurological diseases found across those studies (where for context a 1.1-1.2 [10-20%] increase would normally be enough to get a product a red flag, particularly one given to large numbers of people).
Finally, there are numerous large databases containing both vaccinated and unvaccinated individuals which could “ethically” get that data without withholding vaccines, yet despite decades of legal petitions, these were consistently withheld from independent researchers because it was “not ethical” to provide (easily anonymized) personal health information. RFK in turn campaigned on actually studying this database but remarkably, right before his team got access to it, H.H.S. employees illegally deleted it. “Rare” Vaccine Side EffectsSince all of these tactics are often insufficient to cover up vaccine injuries, another common approach is to dismiss them by insisting they are “rare” and only affect “one in a million.” A classic example is Guillain-Barré Syndrome (GBS), a neurological disorder where the immune system attacks the peripheral nervous system, leading to muscle weakness, numbness, and, in severe cases, paralysis, with roughly 2-10% of cases being fatal. Symptoms often start in the legs and can progress rapidly, sometimes requiring hospitalization. Most people recover with treatment, but recovery can take weeks to months. In medical school, students are taught that most cases of GBS are from certain infections, but it can also be a “one in a million” side effect of the flu vaccine (a risk that is further minimized by noting that influenza infections have a higher risk of GBS, so it is in your best interest to vaccinate if you want to prevent GBS—not unlike how it was claimed COVID-19 was more likely than the vaccine to give you myocarditis). I hence took notice of the fact I kept on hearing of “one in a million” GBS cases (e.g., most recently Tucker Carlson disclosing to Dr. Mary Bowden his young son got GBS from a flu shot). Similarly, at a small hospital I worked at, I met two nurses who’d had a patient or co-worker develop it after a flu shot and later I learned of a community with roughly 100,000 people where one GBS patient had identified at least 20 different people (most of whom were healthcare workers) who developed GBS after a flu shot. Since experiences like that would require roughly 1 in 1,000 flu recipients to get GBS, I suspected the “one in a million” figure is incorrect. Note: similarly, at the start of the COVID vaccine rollout, like many, I saw an extraordinarily high level of vaccine injuries, and hence concluded the people telling is they were “very rare” were lying, and then also lying when that changed to “injuries occasionally happen, but COVID causes far more problems so you need to vaccinate.” This was then corroborated by subsequent surveys showing 34% of vaccine recipients reported minor side effects while 7% reported major ones severely impacting their quality of life (again demonstrating the toxicity bell curve) and a large study showing the vaccine increases your likelihood of getting COVID. The Swine Flu FiascoThe vaccine most strongly associated with GBS was the 1976 Swine Flu vaccine, a completely unnecessary experimental vaccine which was rushed to market despite the FDA’s own scientist (who later participated in the 1985 Donahue debate) warning it was not safe (which, in turn, the CDC responded to by not testing the vaccines given to the public). It caused a significant number of injuries, and numerous political earthquakes followed (e.g., like Biden and the COVID vaccines, the swine flu vaccine fiasco played a key role in Ford losing the 1976 election). Since the press had not yet been bought out by the pharmaceutical industry, there were many scathing pieces on it (e.g., the New York Times wrote one piece on “Swine Flu Fiasco” and another piece on the myriad of injuries along with all the pharmaceutical companies “threatening to stop production completely until Congress protected them from lawsuits by people who suffered side effects from the vaccination”). Of these, the most iconic and well-remembered ones was a 1978 program 60 Minutes put together: While a variety of injuries such as numerous deaths were associated with the vaccine all standard sources say the only problem was a “slight increase in GBS affecting roughly 1 in 100,000 recipients” (e.g., there was one instance where three elderly people who had received shots within the same hour at the same clinic all had fatal heart attacks, but their deaths were deemed “unrelated”). If you look at this with a critical eye, the fixation on the 1 in 100,000 GBS figure doesn’t make sense, as if injuries were “that rare,” it would not have turned into a national fiasco. This I believe, is best demonstrated by a physician (whom I recently verified this chronology with) that: •Entered practice in 1976 Note: 45 years later, that doctor had an almost identical experience with the COVID vaccine, with many long-term patients (who had a great deal of trust in the doctor) nonetheless succumbing to the government’s push for the COVID vaccine and now has a shocking number of very sick patients with characteristic COVID-19 injuries (e.g., turbo cancers). Likewise, one patient I met during the COVID-19 vaccine roll-out shared with me that they had refused to get the COVID vaccine because they suffered a permanent lung injury from the 1976 vaccine and were “not falling for the government’s lies again.” Much of this is encapsulated by a 1961 German paper that highlighted that variolation (what preceded smallpox vaccination) had a 2% mortality rate, that the smallpox vaccines also had a high complication rate and that the medical profession and health authorities “overlooked” “minimized” or “denied” complications to maintain public trust in vaccines so as it was paramount smallpox would be eradicated. As such, the injuries only began to be acknowledged once smallpox was no longer a threat (e.g., a 1913 paper referred to those injuries as “anomalies” whereas in 1927, the term “vaccine injury” began being used), and stated honestly admitting the rare dangers was necessary to ensure public trust in vaccination. The Hazards of ImmunizationIn 1966, an eminent bacteriologist wrote “The Hazards of Immunization” which disclosed a large number of forgotten vaccine disasters he’d collected (both through his team surveying the medical literature and insiders sharing their private files with him) in the hope it could lead to safer vaccines as the same disasters kept on repeating and would likely continue to do so unless his profession acknowledged those risks (which sadly they still have not).
Additionally, many of these forgotten injuries happened in soldiers across the globe, who due to the nature of their occupation, had no opportunity to refuse vaccination and limited avenues for reporting the injuries.
Note: Wilson emphasized that despite his best efforts, he could only access a small sampling of the total number of injuries caused by vaccines and serums. Thus, the injuries he presented only represented the tip of the iceberg, mirroring the situation we still see today (where it’s estimated over 99% of vaccine injuries go unreported). As the lessons from this book are just as relevant then as they are now, I’ve gradually been extracting them into readable articles, and thus far have covered: •How many vaccines have been shown to cause immune suppression and makes latent infections become severe and hence suddenly appear. •How the mentality behind manufacturing vaccines makes hot lots almost unavoidable and has led to many vaccine disasters throughout history—a problem which was sadly “solved” by simply giving vaccine manufacturers immunity from injury lawsuits. Landry’s ParalysisAnother key theme Wilson focused on was the tendency of vaccines to cause unusual neurological injuries. Guillain-Barré' syndrome (GBS) was coined in 1916 after two neurologists (for whom GBS is named) wrote a detailed case history of two French soldiers who had developed GBS. However, what many do not know is that: •They published a 1919 paper that discussed a French soldier who developed fatal GBS from a typhoid vaccine. It began with numbness and stiffness in the legs a day after the injection, then the following day in his hands. Paralysis gradually came on and by the 9th day was complete in the legs, arms, and face. Bulbar symptoms (e.g., cranial nerve dysfunction) developed on the 7th day, and on the 10th day the patient died. •Prior to the adoption of the GBS terminology, this ascending paralytic syndrome was referred to as Landry's paralysis (e.g., that’s what it was called in Guillain and Barré's 1919 paper). •That same year, another case of Laundry’s paralysis was reported from a typhoid vaccine. •As Wilson showed, there were many cases in the early literature of vaccines causing Landry's paralysis (and likewise, other vaccines cause GBS—for example, I’ve met people who got GBS from a COVID vaccine, and the 1976 NYT article acknowledged it is linked to the rabies vaccine). Early Vaccine DesignsAt the time, when early vaccines were produced, modern biological quality controls did not exist (hence why vaccines were frequently contaminated with other diseases). The smallpox vaccine for example, was created by taking skin pustules from a cow with cowpox, scraping them into the arm of a person, and then infecting other people with the pustules from that person’s arm (while later it was simply produced in livestock rather than transferred from human to human). The subsequent early vaccines (e.g., tetanus, diphtheria, pertussis, typhoid) were made by culturing the bacteria, killing them, and then filtering down to the bacterial manner or the toxoid (which was then inactivated by formaldehyde)—a process which had many opportunities for something to go awry (which it frequently did). Likewise, viral vaccines required either chemically inactivating them (e.g., with formaldehyde) or repeatedly passaging them through cell cultures to weaken them so that the virus no longer endangered the recipient but still was intact enough to create a robust immune response (which like the bacterial vaccines frequently led to hot lots that caused the disease being “prevented”). Finally, antiserums (introduced in the 1890s) were widely used as therapeutics (or prophylactic therapeutics) for illnesses. These worked by injecting a horse with the infectious agent or toxin, having the horse mount an immune response to it, and then crudely filtering their blood for antibodies that were produced in response to the agent and injecting the filtrate in humans. Due to their toxicity, the advent of antibiotics, and the ability to make serums from pooled human plasma, their use declined in the 1940s-1960s, and by the 1970s-80s (when it began becoming possible to make monoclonal antibodies with bioengineering) they were largely phased out except for poorer areas which could not afford the modern technologies and for niche uses like making anti-venoms. Each of these agents had significant toxicity (which led to many other schools of medicine criticizing their use), with one major complication they all shared being nerve damage. Note: typically when people are being exposed to a profitable but toxic agent, regardless of the evidence and decades of public protest against it, its use typically only stops when an economically viable alternative to it is found (e.g., serums, ultrasounds replacing routine prenatal x-rays) or outside pressures forcing the industry to invest in developing the alternative (e.g., scientists tried for almost 50 years remove neurotoxic lead from gasoline, but it was only the introduction of catalytic converters making lead no longer work in gasoline which spurred the development of lead alternatives or the 1986 Vaccine Injury Act forcing the development of the less toxic DTaP vaccine to replace DTwP). Nerve InjuriesThe nervous system is divided into two parts, the central protected part (the brain and spinal cord) and the nerves that branch off the central nervous system into the periphery (known as the peripheral nervous system). Since the central nervous system (CNS) controls so much of the body and typically won’t regenerate after being damaged (unless an agent like DMSO is used), injuries to it tend to be much more life-threatening and disabling. Likewise, as the functions of the nervous system have been extensively mapped out, one’s area of neurological injury can often be inferred from their symptoms. For example: •Paralysis on one side of the body (hemiplegia) normally indicates damage to one side of the brain (e.g., due to a stroke), while full paralysis (paraplegia) denotes a wider CNS injury. •Loss of automatic functions of the body (e.g., breathing, temperature control, or consciousness) often indicate an issue in the brainstem. •Loss of normal functions of the face (e.g., eye movements) indicates an issue with the peripheral cranial nerves. As almost all these nerves originate in the brainstem, an issue with them often indicates an issue within the brainstem as well (e.g., a drooping face is used to diagnose strokes). •Loss of control below a certain level of the body often indicates a spinal cord injury above that point. Additionally: •When nerve issues (e.g., numbness, weakness, a loss of reflexes or muscle atrophy) are localized in one area, or an area and everything which branches off it, it is typically a peripheral nerve issue. •In some cases, a peripheral nerve issue can spread (e.g., GBS) and eventually affect a large portion of the body like CNS issues. •Both central and peripheral nerves rely upon an insulating coating (myelin) to function. Frequently, autoimmune processes (e.g., vaccine-induced ones) can trigger an attack on myelin, which in turn can cause either a central issue (e.g., multiple sclerosis or transverse myelitis of the spine) or a peripheral one (e.g., GBS). In most of the early literature, the following terms were commonly used: •Neuritis—a peripheral nerve issue. In many of these cases, because the injuries were severe, multiple issues were occurring concurrently (e.g., encephalomyelitis) and in some cases, exactly where the nerve was occurring is debatable. Lastly, many of these injuries led to agonizing deaths. Still, due to the number of cases discussed, there is no space to describe the immense suffering associated with these injuries fully. Note: Wilson found most neurological complications after vaccines were of the myelitic or encephalitic type. While I generally agree with this statement, peripheral injuries of the cranial nerves are also frequently seen (especially acutely). Serum InjuriesLike vaccines, serums could cause both central and peripheral nerve injuries. For example, one type of injury (Erb's palsy) which arises from damage to some of the key nerves which control the arms was a well-recognized complication of horse serums (especially tetanus ones).
In his book, Wilson cites individual case reports of serum neuritis occurring in 1897, 1904, 1908, 1912, 1917, 1918, 1949 and 1963 (four of which affected an arm, one of which affected a leg and one of which was labeled as “polyneuritis”) along with: •A 1926
case where a serum after 12 days caused a near fatal Landry’s paralysis
in all 4 limbs and the face, with the facial paralysis persisting for a
prolonged period. Wilson
also cited a variety of papers which evaluated multiple cases to piece
together the common (and often severe) symptoms of this condition. They
included: •A 1922 report of three cases of optic neuritis, along with a 1929 report of left-sided amblyopia (impaired eye movement) and optic disc swelling. •A
1924 review that identified 25 cases of polyneuritis following the
injection of serum (with 18 from a tetanus antiserum and 4 from a
diphtheria antiserum). •A 1932 review described numerous cases where patients, after receiving serums, experienced severe reactions upon a subsequent dose, typically 3 days to a month later, including seven where brain damage occurred (half of which were fatal). Symptoms included generalized urticaria, followed by convulsions, tetanus like muscle spasms, coma, rapid irregular pulse, irregular breathing, and sometimes death along with residual paralysis and muscular atrophy when the spine was involved. That review also covered 40 cases (plus one of the author observed), including two neuritis cases due to a typhoid vaccine and one due to a staphylococcal vaccine. •A 1937 paper
discussed disturbances of the CNS after intraspinal injection of serum,
characterized either by nuchal rigidity, convulsions, coma, pleocytosis
(immune cells in the CSF) and death, or by bizarre manifestations such
as urticaria, aphasia, partial hemiplegia, hemianopsia and papilloedema. •A 1942 review identified 4 cases of paralytic CNS involvement resulting from non-spinal serum injections (including one which was eventually fatal due to respiratory paralysis). •A 1944 summary of 3 hospital patients who developed serum neuritis (two from tetanus and one from typhoid), with the typhoid case developing a central type characterized by paralysis on half of their body.A 1942 review which identified 4 cases of paralytic CNS involvement resulting from non-spinal serum injections (including one which was eventually fatal due to respiratory paralysis). •A 1944 summary of 3 hospital patients at a hospital who developed serum neuritis (two from tetanus and one from typhoid), with the typhoid case developing a central type characterized by paralysis on half of their body. •A 1953 report
of 20 cases, 2 of which had features of cerebral neuritis and noted
that “the pain in serum neuritis is often so severe that the early
paralytic features are masked.”
Vaccine Neurological InjuriesIn his book, Wilson attempted to compile every documented report of injuries he could identify, with the exception of smallpox vaccine injuries as these were so frequently reported it was not feasible to have every single one in the text. Likewise, while he compiled many reports of pertussis injuries, since the DTwP vaccine remained in use for decades after his book’s publication, many more reports emerged, and likewise, other authors were able to identify early injury reports Wilson did not come across (some of which I’ve included). Additionally, in many cases, non-neurological injuries were also reported, but to keep this focused, they will be omitted. Note: to the best of my ability, I attempted to locate every case Wilson referenced. Some of them came from sources like old French medical journals that are not widely indexed, and despite my best efforts, I could not locate every case. Still, I found Wilson accurately represented the publication’s findings in those that I did. The citations for all of Wilson’s references can be viewed here. TyphoidPrior
to antibiotics (e.g., in the age of trench warfare) typhoid fever
epidemics were a frequent challenge for armies. As such, military
commanders frequently mass-vaccinated soldiers despite the vaccine often
having significant complications. •A 1916 case of polyneuritis in a soldier following his second round of vaccination beginning with shoulder pain, that spread to his knees and other leg joints. A year later, he was diagnosed with polyneuritis having experienced disturbed deep sensation, unsteady and slow movements, balance problems when standing or sitting, and ongoing, treatment-resistant pain in muscles and around joints, worsened by walking. He also had excessive sweating on the right side of his face and left hand, bulging of the right eye, and paralysis of a muscle in the left eye. •A 1919 paper reported on two soldiers who had reactions. One immediately had severe reaction with fever lasting over a week, and on the third night, became blind for 10 days (due to optic neuritis and partial optic nerve damage), after which his vision only partially returned. The other had a strong reaction lasting four days and after two weeks developed repeated convulsions in his left arm and face, sometimes spreading body-wide, with jaw clenching, bloody saliva, loss of cranial reflexes, and fainting. A year later, his left arm was weak and still had frequent convulsions attributed to brain irritation in the right Rolandic cortex. •A 1920 report covered 10 documented cases by three authors of neurological injuries between 1918-1920. Symptoms typically started within hours to days of the injection. They included severe headaches, vomiting, fever, stiff necks, seizures, syncope, weakness or paralysis on one side of the body (hemiplegia), trouble speaking (aphasia), or unsteady movements (ataxia). One developed signs of Graves’ disease (with bulging eyes and shaky hands), another suffered a fatal case of GBS-like acute ascending paralysis, another had mania (which was observed in other vaccine injuries) and memory impairment, another lost the ability to have erections, and one partially lost the ability of their pupils to dilate (accommodate). •A 1924 case of incoordination of the legs leading to a staggering gait. •A 1928 case described a case of persistent leg paralysis and temporary incontinence that was diagnosed as polio. •A 1929 case where a 34-year-old man, after his second vaccine, had a severe reaction with high fever and hives. He developed numbness in his feet that spread to his waist and fingers, trouble focusing on close objects, partial loss of sensation in a "glove-and-stocking" pattern, weak and clumsy grip, and extreme fatigue. Symptoms lasted eight weeks before slowly improving. •A 1932 report of three patients with partial or complete limb paralysis, with one also showing vision loss on one side, inability to speak, and deafness in the right ear. •A fatal 1933 case of Laundry’s paralysis. •A 1937 paper discussed a patient who developed flaccid leg paralysis for 3.5 months after vaccination. •A 1939 JAMA report of 5 cases with the author stating that about 115 instances of authentic vaccine neuritis had been reported in the literature thus far, 20% of which resulted in permanent weakness or muscle atrophy. •A 1941 case that began with weakness, followed by being unable to sit or walk, then breathing trouble, after which they collapsed and died from encephalitis eight days after an injection. •A 1942 case of fever, headache, nausea, delirium, seizures, coma, followed by death 26 days after an injection, with autopsy showing brain hemorrhages and hemorrhagic necrosis (tissue death). •A 1943 report of acute paraplegia. •A 1944 summary of four vaccine neuritis cases. Three cases followed typhoid vaccine: one patient developed right arm paralysis ten days later, recovering within three months; two others experienced shoulder weakness 10 and 14 days later—one fully recovered, the other had persistent muscle wasting. Additionally, one, ten days after tetanus toxoid injections, developed slurred speech, eye twitching, and left-side weakness, with partial recovery after four months. •A 1945 case where a soldier developed right-sided arm weakness, pain, and tingling one week after a booster (which was followed by shoulder muscle wasting). A 1948 report of a fatal case of typhoid vaccine-induced paralysis (hemiplegia) and encephalitis, with brain autopsy showing many lesions including oligodendral proliferation in the baso-frontal region, widespread and complete demyelination in the right occipital lobe with perivascular collections of large fat-laden phagocytes in the softened areas. •A 1954 paper that reviewed over 50 cases of neurological injuries including 12 cases of nerve inflammation (radiculitis, plexitis, or mononeuritis) after typhus vaccine, 10 cases of widespread nerve damage, (transverse myelitis or GBS) and 20 cases in which various manifestations of cerebral or meningeal disturbance were observed.
Note: many vaccines will cause an immune suppression which causes latent infections to spiral out of control. Since typhoid fever frequently did not display symptoms as it transmitted through an army, typhoid vaccines would often be mass deployed to see who became ill with typhoid fever so that they could be quarantined from the army. Yellow FeverThere have been long standing issues with the yellow fever vaccine, many of which I believe resulted from the difficulty of correctly attenuating it (leading to numerous hot lots being produced): •A fatal 1934 case began with fever, headache, giddiness, and neurological symptoms in the lower limbs, including fatigue, cramps, cold sensations, and the feeling of insects crawling on his skin. These resolved, then reappeared alongside severe leg weakness, weight loss, urinary and fecal difficulties, and progressive sensory loss extending to the thighs and forearms, eventually becoming bedridden and then deceased 14 months after vaccination. Autopsy showed extensive myelin degeneration, vascular lesions in the spinal cord, and cytolytic changes in brain cells (encephalomyelitis). •A 1936 case where a yellow fever vaccine (and a serum) were followed 11 days later by acute meningitis, lymphocytosis, altered colloidal benzoin reaction, high fever, headache, general convulsions, epilepsy, narcolepsy, mental confusion, and intracranial hypertension, with recovery taking 1-2 months. Another paper revealed that the lot the patient received had caused nervous disturbance in at least three other persons. •A 1936 report discussed 5699 people who received a yellow fever vaccine between 1934 and 1935, of whom roughly a third had reactions with the serious ones being either neurological or visceral in nature and mirrored neurological reactions observed in other yellow fever vaccine reports. •A 1943 report showed that one lot given in Brazil caused 1.65% of recipients to develop encephalitis, while another caused 0.06% to develop encephalitis. •A 1953 WHO report stated the yellow fever vaccine campaigns had caused 12 encephalitis cases with 3 deaths in Costa Rica (1951), 83 encephalitis cases with 32 deaths in Nigeria (1952), 254 encephalitis or meningoencephalitis cases (e.g., violent headaches, somnolence progressing to torpor, nausea, vomiting delirium, giddiness, photophobia, hyperexcitability, convulsions and 1 death) amongst 69,843 recipients in Brazil (1941) and a possible 1938 meningitis case. •A 1953 paper discussed a (likely hot) yellow fever vaccine given for an outbreak in Nigeria, with 0.3-0.4% of recipients developing encephalitis often starting with fever followed by hourly convulsions, irritability, disorientation, loss of speech or slurred speech with 40% of the afflicted children dying. Two cases also showed residual paresis and mental deterioration, while autopsies of five fatal cases showed focal necrosis, blood vessel cuffing (immune cells coating the outside of the vessel), and congestion in the brain along with yellow fever vaccine virus being present in three of four brains tested. Equine EncephalomyelitisA 1954 paper discussed a hot Venezuelan equine encephalomyelitis vaccine that caused 14 of 327 recipients to develop roughly a day of symptoms such as sudden fever, chills, severe headache, muscle pain, lethargy, prostration, visual blurring, and occasionally nausea, vomiting, and diarrhea with no fatalities. Rabies
Note: this situation existed largely because it was difficult to find a dose of the rabies vaccine that was strong enough to prevent rabies but weak enough not to cause paralysis. Other than local reactions, rabies vaccine injuries were almost all neuroparalytic in nature, averaged a 10-16.85% fatality rate, and were one of the four following types: •Dorsolumbar
myelitis, the most common, characterized by weakness, lassitude, and
fainting, which has a 5% fatality rate and leaves some with disability
(e.g., partial paralysis of the legs or difficulty controlling the
bladder). In 1927, a researcher collected 329 cases of paralysis amongst 1,164,264 who were treated and estimated the real figure likely lay between 500 and 1,000. Following this, a variety of other data sets were collected, which like the smallpox vaccine, greatly varied in their neurological injury rate (ranging from 86 to 2,367 incidents of paralysis per million vaccinated individuals). 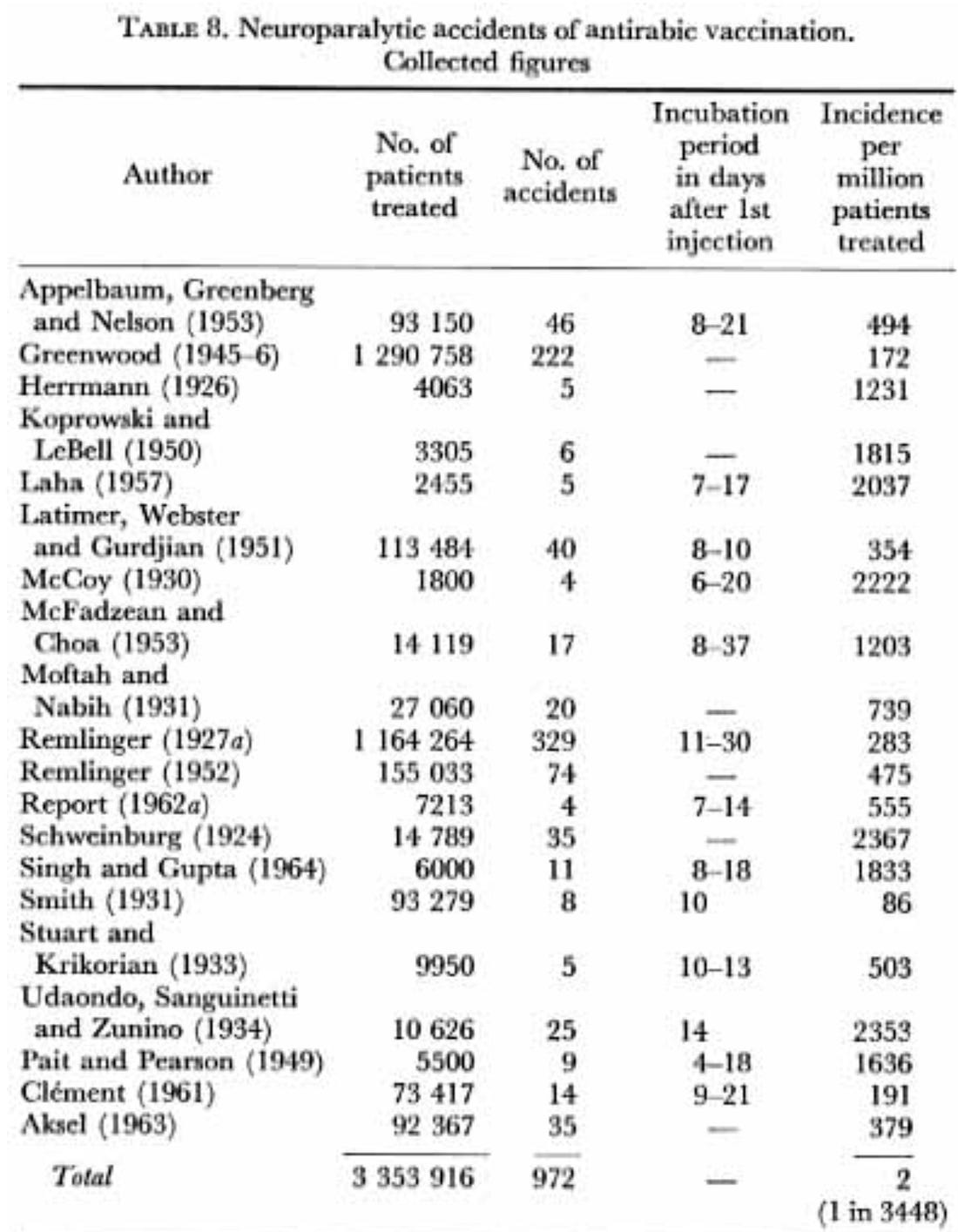 Note: these rates were also influenced by the type of vaccine used and the number of injections given (e.g., those who received 14 injections were five times as likely to get it as those who received 7 or fewer). Additionally, it was noted that those who engaged in intellectual work were at greater risk. A 1926 paper discussed eight fatal rabies vaccine reactions, three of which were reviewed (a likely transverse myelitis, along with two that had features of both myelitis and rabies). A 1952 paper reported 30 cases of paralysis resulting from insufficiently attenuated rabies vaccines. In 1960, a hot (insufficiently inactivated) rabies vaccine caused 18 out of 66 to develop acute encephalomyelitis and die with symptoms including malaise, muscle pain, neck pain, high fever, headache, spasms, convulsions, difficulty swallowing, double vision, vomiting, paralysis, breathing distress, excessive salivation, urinary incontinence, lethargy, coma, and death. Autopsy showed brain and spinal cord inflammation with perivascular infiltration and nerve cell damage. A 1950 study of 50 rabies vaccine recipients found 17 of the 34 who received the vaccine for 14 days developed antibodies that could react with brain tissue. Still, none of the patients who got it for only 7 days did, and in two out of three patients who developed encephalomyelitis, these antibody levels were high. Note: the existing rabies vaccines, while not completely safe, are produced in a much more advanced and safer manner than they were at Wilson’s time. Measles:A 1966 case occurred in a 14-month-old child who developed encephalitis 11 days after vaccination, first showing twitching on the left side of the face, then fever, a shaky left hand, stopped eating, and became semi-conscious. By day 15, the child had a 103°F fever, weakness on the left side, and was very sick and lethargic. The soft spot on the head bulged slightly, with twitching in the left hand’s fingers, limp left arm and leg, and reduced reflexes. In the hospital, the child had frequent severe seizures. After four months, the child was released but still had left-sided weakness and possible mental impairment. Polio:Wilson (and many authors) considered the polio vaccine, particularly the inactivated one, to have a very low injury rate (excluding notorious hot lots such as the Cutter incident where large numbers of people were injected with improperly activated poliovirus and ….. developed polio). While this appears to be true from the data Wilson gathered, it contradicts my own experience (before going to medical school I knew two people who developed polio from a childhood vaccination) and the frequent (and often large) polio outbreaks that follow the oral (live) polio vaccine’s more recent deployment in low-income countries (e.g., Gate’s recent campaign caused 491,000 polio cases in India). Wilson’s data was as follows: •A 1963 case where brachial neuritis followed a severe local reaction to Salk polio vaccine. •In 1963, the polio vaccine’s creator reported two fatal neurological injuries, a disseminated myelitis from the inactivated vaccine and a paralytic disseminated encephalomyelitis from the oral vaccine. Two 1963 papers1,2 analyzed neurological complications observed following live polio vaccination. In 150 cases of muscle paralysis, there were 23 instances of paralysis or abacterial meningitis—all which were linked to vaccination, 22 cases of isolated facial paralysis—3 of which were deemed to be linked to vaccination, and 10 cases of polyradiculoneuritis or encephalomyelitis where a link could not be proven. Additionally, in a sample of 22 million recipients, 52 injuries linked to vaccination that appeared to be associated with vaccination were reported. In 21 of these, the symptoms resembled those of poliomyelitis; they came on 3- 82 days after vaccination, mainly 5-15 days. In 31 of the 52 cases, the symptoms were those of facial paralysis, polyradiculoneuritis, or encephalitis. A 1964 report discussed 13 neurological injuries (mostly in children) detected amongst 6 million inactivated polio vaccine recipients, including a Laudry’s paralysis, a GBS, a meningomyeloradiculitis with leg paraplegia and meningitis, a left foot paralysis, three of polyneuritis affecting particularly the lower limbs, and six of neuritis with paresis of one foot and one death (a meningomyeloradiculitis, with fibrinoid changes in the walls of small blood-vessels in the medulla and spinal cord). As these cases were quite rare, it could either mean they were unrelated to the vaccine, they are an extremely rare complication, or that many injuries in the sample were missed. In 1965, two other authors reported on five neurological injuries following that vaccine (paralysis of the eye muscles, two acute psychoses, and two general convulsions), two of whom had previously suffered from a neurological disorder (which may have been exacerbated by the vaccine). Additionally, it is my belief many vaccine injuries were incorrectly labeled as “poliomyelitis” or bulbar polio (dangerous damage to the brainstem) as many of these neurologic syndromes have similar symptoms (e.g., to quote Wilson “The differential diagnosis of post-vaccinal [smallpox] encephalomyelitis is not always easy to make from poliomyelitis coming on after vaccination.”). It was not until the polio vaccine came out that a tight criteria was established for what constituted polio (which led to a massive drop in polio cases) whereas beforehand, there were numerous financial incentives to classify severe neurological complications as “infectious” polio.
This is particularly important as many polio outbreaks followed polio vaccination campaigns, and in looking at things retrospectively, I feel a strong case can be made both that those outbreaks were misdiagnosed neurologic vaccine injuries or that they were due to vaccine-triggered immune suppression or neural puncturing causing a benign polio infection to become poliomyelitis. In the 1950s, many papers (summarized here) were written on polio outbreaks in New York and England. They all found that vaccination, particularly with whole-cell pertussis (which is still distributed throughout the developing world), significantly increased the risk of subsequently developing polio, with paralysis being 1.5-3X as likely to develop in the affected limb. These papers included a 1950 paper (82 cases), a 1950 paper (14 cases), a 1950 paper (30 cases), a 1950 paper (31 cases), a 1951 paper (31 cases), a 1952 paper (53 cases), a 1952 paper (1300 cases), a 1953 paper (13 cases), and a 1956 report (355 cases). Wilson shared that the MoH received 31 reports of vaccination preceding polio between 1941 and 1946. Furthermore, a 1950 statistical analysis (authored by the epidemiologist credited with creating the standards for establishing causality) of 410 poliomyelitis patients under five corroborated the vaccination link. Likewise, a 1952 paper (reviewing 2137 New York poliomyelitis patients) found recent vaccination doubled the risk of polio, a 1952 paper on an English outbreak found vaccination quadrupled the risk of polio, and a 1953 paper found this happened to 1 in 1800 vaccinated children (0.056%).
Note: pertussis was repeatedly reported to be the most likely to cause polio (becoming even more harmful as other antigens were given concurrently), and likewise, more recently in Africa, was found to make children 4-10 times as likely die, with most of these deaths resulting from DTwP’s immune suppression causing them to succumb from dangerous endemic diseases. Lastly, a 1950 paper
tested five children who had developed paralysis following vaccination
(comprised of meningo-encephalitis and facial nerve paralysis following
smallpox vaccination, paralysis of both arms following DPT, paralysis in
the vaccinated arm following DPT, a “cold” and then injected arm
paralysis following DPT, and neck muscle paralysis following DPT). In
all five cases, active polio virus was found in the stools, but as the
author noted, it was not clear if polio caused the paralyses or if it
simply was endemic and hence present in the stool. Diphtheria:A few published reports existed of diphtheria vaccines causing neurologic injuries. •A 1965 chapter on producing the diphtheria vaccine which included a few cases of paralysis due to neuritis following the diphtheria vaccine. A 1948 case of aseptic meningitis (with recovery in a week) occurring 2-3 days after injection. •A 1954 case where a boy who’d received a diphtheria vaccine later received a Schick test (where a small amount of diphtheria toxin is injected into the skin to test one’s susceptibility to it) had a hypersensitivity reaction that caused acute bulbar encephalopathy left him with residual wasting of the left masseter and temporal muscles leading to difficulty in moving the jaw. Additionally, Wilson shared that the MoH received a report of a child developing encephalitis who died in two days and two cases where children developed bilateral optic neuritis (one of whom also had disseminated encephalomyelitis) following diphtheria vaccination. However, the majority of neurological issues following diphtheria vaccination resulted either from it provoking poliomyelitis or from diphtheria hot lots (discussed here) where the diphtheria toxin was not sufficiently inactivated prior to injection or diphtheria toxin was given instead of antitoxin, resulting in severe or lethal cases of diphtheria such as: A 1919 incident in Dallas, Texas, where several hundred doses of a hot lot were given, with the majority of recipients having severe reactions and 8.33% dying. Most followed a consistent progression that in the third week involved paralysis throughout the body (including the pupils, eyelids, and tongue). •A 1924 Massachusetts incident, where two hot lots severely injured 43 of the 54 recipients, with symptoms including dilated pupils and exaggerated or absent reflexes (but no deaths). •A 1927 incident in the U.S.S.R, where 14 children received diphtheria toxin, 12 of whom died. There, administering the antitoxin, appeared to prevent immediate death and instead caused them to die from a progressive paralytic disorder which affected the soft palate, legs, and diaphragm. •In Columbia in 1930, 48 children were accidentally given diphtheria toxin many became severely ill (often becoming comatose or convulsive) and 16 of them (with 14 dying in 1-3 days and the others dying from progressive neurological symptoms). •In Italy, in 1933, several hundred infants and children became severely ill (with 30 over dying). Initially, they experienced cranial nerve issues (e.g., loss of visual focusing and accommodation, strabismus, drooping eyelids,) fatigue and limb weakness, followed by paralysis throughout the body (including sometimes the diaphragm), loss of proprioception, and unusual sensations throughout the body. Additionally, one of their earliest symptoms was an exaggeration of the oculo-cardiac reflex where in several hundred patients it was observed that compression of the eyeball led to stoppage of the heart. •In 1948, in Kyoto and Shimane (Japan), hundreds of infants and children became severely ill and over a hundred died from muscular paralysis (e.g., of the diaphragm).1,2 Pertussis:With many of the vaccines Wilson discussed, he felt their real risks were counterbalanced by the benefits they provided. While I disagree with this argument (e.g., because the injuries were massively underreported and the vaccines were not 100% effective in preventing disease, many would never get regardless), I could understand his reasoning. However, Wilson felt differently on the pertussis vaccine, both due to its high rate of highly unusual injury and the fact that pertussis was no longer a significant concern that justified a risky vaccine:
Sadly, despite saying this in 1966, no efforts were made to remove the vaccine or produce a newer one until it caused so many injuries that widespread lawsuits occurred, critical media coverage was aired (e.g., that mentioned above) and the 1986 law forced the development of it. Note: many different combinations of whole cell pertussis vaccine (DTwP) were given (e.g., with Diphtheria and Tetanus [DPT], it alone, only with Diphtheria, or also with polio). Henceforth, for brevity I will refer to all cases as DPT even if that was not the exact pertussis combination. I will now review the cases Wilson and a few others compiled: •The MoH's files for 1963, 1964, and 1965 contained letters from medical practitioners and officers in all parts of England and Wales complaining of untoward reactions to DPT. The reactions include anorexia, fever, irritability, prolonged crying or screaming, vomiting, collapse, stiffness of the neck, drowsiness, and epileptic convulsions. Additionally, between 1958 to 1965 the MoH recorded seven fatal cases of encephalitis, meningoencephalitis or encephalopathy from DPT. •A 1954 paper noted that convulsions were the most common neurological complication of DPT and that unlike other vaccines, it tended only to injure the central nervous system but not the peripheral one (e.g., encephalitis was seen but GBS was not). •The 1933 case
of an infant less than a week old being seized by convulsions thirty
minutes after the first injection and then dying within the first two
minutes was the earliest case of a fatal encephalopathy Wilson could
identify from DPT. Seizures (often indicating encephalitis) have long been associated with the DPT vaccine (e.g., a 1936 report discussed three cases while a 1938 case report discussed another). •A 1945 collection of numerous cases of abscess formation after DPT, along with one case of angioneurotic edema of the eyelids and lips associated with transient anuria, and two instances of vomiting, diarrhea and convulsions •A 1947 case discussed a baby, possibly sick with undiagnosed whooping cough, got a DPT vaccine and two weeks later had mild encephalitis, which worsened a week later after another vaccine, worsened again after a third vaccination, and then after a spontaneous encephalitis exacerbation, get a fourth low-dose vaccination which within 12 hours led to severe flaccid paralysis which seven weeks later concluded as the child had died from a fatal broncho-pneumonia. •A 1948 report detailed 15 cases at a hospital of infants aged 5-18 months with no history of seizures who developed convulsions lasting minutes to days, followed by drowsiness or coma. Two died from pneumonia, five had paralysis, two had severe brain damage (becoming decerebrate and losing most conscious brain function), five had mental or neurological issues (e.g., developmental disability), and only one fully recovered. •A 1949 report detailed two cases of encephalopathy, one of which was fatal (with widespread disintegration of the brain being seen on autopsy). •A 1949 report was written by a doctor who wrote to several doctors and learned of 38 cases of severe DPT reactions, mostly convulsions, of which two at least were fatal, and at least 12 showed irreversible changes of the nervous system. •A 1950 case discussed a two-year-old boy who had seizures following DPT. Eight months later, doctors found an dilated left heart chamber and reduced activity in the left side of his brain and a year later was diagnosed as “mentally retarded.” •A 1953 article contained 84 cases of brain-related issues after DPT (primarily in infants) identified by the author (including two they’d witnessed). Of those summarized (many were not), 11 died, 24 had permanent complications like seizures, spastic paralysis, or developmental delay or personality changes. Following this, another author reviewed 107 cases of neurological injuries from the DPT vaccine (including those from the 1953 article) and found 8 were fatal within 48 hours, overall 15% were fatal, 30% had long-term complications, and roughly half recovered. •A 1958 report concluded that 1 in 3000 DPT recipients developed convulsions, •A 1958 review of 107 reported DPT injuries (which included those in the 1953 collection) found 8 were fatal within 48 hours, overall 15% died, 30% had significant long-term complications, and around 50% recovered. They also shared a case they’d witnessed where a healthy child developed a fever and unusual cry immediately after DPT, lost interest in everything, developed convulsions that progressed into elipesy and became permanently “mentally retarded.” In response, another doctor, in 1958 reported that in the last 10 years, they’d had 6 patients who had severe neurological reactions within 24 hours of DPT, one of whom died, and three who had permanent brain damage (e.g., “mental retardation” and motor impairments). The other neurological injuries they saw included convulsions (in all, with some cases progressing to status epilepticus), hemiplegia (in 2), brain congestion and edema (found in autopsy), prolonged coma (in 3), ataxia (in 3), restlessness and destructive behavior (in 2), stupors and lethargy. •A 1960 report from Sweden said that 36 cases of neurological complications had been reported from DPT vaccination, most of whom had convulsions, with four dying and nine suffering from a severe encephalopathy (e.g., mental retardation), working out to 1 in 6000 vaccinations •A 1961 series
of 1700 infants found that 40 of them became ill within 30 minutes to 4
hours of vaccination. Reactions included severe local and general
reactions, while others suffered from generalized eczema (which unlike
the rest took a few days to develop), a generalized macular rash,
persistent vomiting, persistent uncontrollable screaming, or collapse. •A 1962 report discussing the reported neurological injuries from the DPT vaccine found they fell into three categories. The mildest involves brief seizures, similar to those caused by a fever, which typically resolve without lasting effects. The second, more severe type resembles encephalitis, leading to unconsciousness, prolonged seizures, and a high chance of permanent neurological damage, sometimes even death. The third type involves a gradual mental decline, with or without seizures that may resemble infantile spasms. Wilson also knew a U.S. doctor who sent 104 questionnaires to university and state health departments about DPT reactions between 1955 to 1960. Within the 75 responses, 14 reported 21 cerebral complications, mostly in infants under one year of whom 14 had permanent mental damage or ongoing convulsions, 3 recovered fully, and 4 had unknown outcomes (again demonstrating the massive public underreporting of these injuries). A 1965 study found that intraperitoneally injecting rats with rat or guinea-pig spinal cord mixed with commercial DPT caused acute encephalomyelitis, with paralysis of the limbs progressing to quadriplegia in 6-11 days, followed by death 1-2 days later and autopsy showing extensive perivascular lesions in the central nervous system with enormous numbers of polymorphonuclear leucocytes and demyelination around the vessels. •A 1965 paper also attributed uncontrollable screaming (which began within an hour or two and typically lasted for up to 24 hours) to the vaccine. That author also shared that during the previous few years, several infants had been admitted to the hospital under his care who had collapsed and become pale, shocked, and apparently lifeless soon after receiving the DPT vaccine. •Lastly, while not a neurological injury, I feel a 1966 case is important to include as it demonstrates many of the pathologies which underlies neurological injuries. In it, a 45-year old volunteered to be hyperimmunized to donate pertussis antiserum. He was first given 7 injections over 6 weeks (as best as I can tell, not experiencing side effects), and then 2 months (when an allergy had now developed) later, he got his 8th injection and a week later became ill. Initially, he had fever, night sweats, arthralgia, and adenopathy, then coughing up blood and cramping abdominal pains. He deteriorated and died in about 3 months. Autopsy showed vasculitis throughout the large and small arteries that fed the internal organs, and numerous clots were found throughout the arteries and veins of the kidneys (which was fatal). SmallpoxSmallpox vaccination was preceded by smallpox variolation (giving a small dose of smallpox to create immunity), and cases of this practice causing encephalomyelitis were described as early as 1768. By 1800, they were regularly being reported for the vaccine (e.g., in Bohemia, between 1801 and 1802, 35 cases were reported out of 10,090 people vaccinated for smallpox). Wilson, in turn, considered the smallpox vaccine to have the highest rate of complications and deaths.
Note: Wilson pooled dozens of studies from around the world and found that out of 8 million people, 0.0015-0.0754% (depending on age) developed encephalomyelitis (specifically referred to as “post-vaccinal” as “vaccinal” was another term for the smallpox vaccine), while out of 18 million people, 0.0063% developed post-vaccinal encephalitis—figures likely low as many cases were not reported (e.g., one study found a 0.144% rate of post-vaccinal encephalitis). He then reviewed 2398 cases of post-vaccinal encephalitis, of whom 34% died (ranging from 9-57% depending on the study), and that a much higher death rate was seen in younger children. Since
so much literature was published on it causing nerve damage, Wilson did
not have the space to cite much of it. However, he cited: •A 1926 report of both case histories and pathology findings (e.g., of the central nervous system) from dissections of seven people (starting in 1912) who died from the smallpox vaccine (which noted the encephalitis had certain features resembling poliomyelitis) that was then followed by a 1928 pathology report of three patients which corroborated the 1926 report and a 1960 report which agreed with those findings but argued that a separate process that was primarily vascular in nature was happened in children under two who died. •A 1948 report on 222 severe cases (including 110 deaths) of post-vaccinal encephalomyelitis that were reported to the MoH. Nearly half the cases and deaths occurred in school-age children (5–15 years), while infants were twice as likely to die, 75% had comas or brain damage and 10% had spinal cord issues. •A 1956 German report which stated that the shift to animal production methods for the smallpox vaccine (or repeatedly passaging it through cells and tissues such as parts of animal brains and spinal cords) increased its virulence and made post vaccine encephalitis 4-6 times more common (e.g., between 1945-1951 in West Germany 263 cases of post-vaccinal encephalitis were reported, of which 106 were fatal). •A 1961 report of 265 cases of post-vaccinal brain damage (proven by autopsy) found it took between 4-18 days for the symptoms to emerge, and that on average encephalomyelitis was lethal 12 days later, while encephalopathy was lethal in 10 days. •A 1964 report of 39 patients who developed neurological disorders following a 1962 smallpox vaccination campaign, including 5 who suffered from polyneuritis and 2 from brachial neuritis. •A 1965 report stated that between 1960-1962, Bavaria received 36 reports of post-smallpox vaccine encephalitis and 15 cases of worsening brain damage. •A 1965 report
discussing 60 cases of post-vaccinal encephalomyelitis from the
smallpox vaccine that were reported between 1951-1958, with symptoms
such as headache, vomiting, drowsiness, or coma followed by flaccid and
then spastic paralysis that typically affects the legs. This final stage
can be accompanied by a wide range of eye issues (and sometimes
blindness) such as proptosis, nystagmus, photophobia, upward deviation
of the eyes, bilateral optic nerve neuritis, optic atrophy, spasm of the
central retinal artery, keratitis, chorioretinitis, central serous
retinopathy, thrombophlebitis, nystagmus, dilated pupils, photophobia,
small pupils, and blurring of the optic disks. Wilson also shared that after post-vaccinal encephalitis was made notifiable in Austria in 1927, over the next 8 years, 270 cases were reported, of which 240 were regarded as genuine. Finally, as I show in this article, many physicians (particularly in the early days of smallpox vaccination), observed a variety of highly unusual and severe neurological symptoms from the smallpox vaccine (particularly in those who did not have strong immediate reactions to the vaccines—something also seen with reactions to diphtheria hot lots and encapsulated by Hering’s Law of Cure).
Burnett in turn, described many unusual cases of severe neuralgia (nerve pain) throughout the body in his 1884 book. Likewise, he and other authors of the time noted the vaccine triggered a variety of neurological issues such as head pains, various types of paralysis (e.g., paresis, hemiplegia, general paralysis), cranial nerve issues (e.g., facial palsy, twitchings, impaired vision), along with autonomic dysfunction (e.g., hyperhydrosis or erectile dysfunction), seizure disorders, intense nervousness, memory loss, confusion, loss of consciousness. Finally, like many after them, they also frequently observed encephalopathies and myelitis. Additionally, they observed a variety of other issues (e.g., many different skin problems). The most notable of which was many different physicians highlighting a general loss of vitality following smallpox vaccination which made their patients both weaker and more susceptible to a variety of other illnesses (and which I now believe was an inflection point in the general decline of humanity’s health). Vaccine Injury SusceptibilityAn interesting point Wilson repeatedly mentions was that other physicians over the decades observed that constitutionally sensitive individuals (or those belonging to constitutionally sensitive families) were much more likely to be injured by the smallpox vaccine. This observation in turn led to many authors encouraging giving the vaccine at a later age and Bavaria’s ministry of health eventually postponed smallpox vaccination until the age of 2 so natural illnesses would not be mistaken for vaccine complications. Likewise, a study which compared 16 patients with severe reactions to the rabies vaccine to 45 who did not found that 80% of those who reacted had a past history of allergic disease ,whereas in those who did not, only 30% did. Similarly, the author of a 1953 article on DPT encephalitis concluded it was unwise to immunize any child with a history of convulsions or allergy, or of nervous or allergic disease in the family, is in poor general health, is suffering from an infectious disease, or has reacted strongly to a previous injection of DPT. Over the decades, many others through their observations of vaccine injuries have likewise offered similar advice on vaccination (as sensitive patients are more likely to become vaccine-injured). Still, authorities always reject those medical exemptions (which would reduce vaccine sales) since the only CDC sanctioned contraindications to most vaccinations are an anaphylactic reaction (to the point doctors often lose their licenses for writing exemptions for anything else). Note: Wilson also shared that post-vaccinal neuritis (like serum neuritis) typically appeared 7-10 days after injection and was more common after the second than the first injection. Mechanisms of NeurotoxicityIn reviewing these cases, a few common theme emerged: • Stroke-like symptoms (e.g., paralysis of a cranial nerve or of one side of the body) •A wide range of demyelinating syndromes that were likely due to autoimmunity. •Active virus (e.g., rabies or smallpox) or toxin (e.g. diphtheria) directly injuring tissues. In turn, a few mechanisms were proposed at the time (when much of our modern pathologic knowledge had not yet emerged). First, the peripheral nerve paralysis (which predominantly affected the arms) was frequently proposed to be due to: •A
“manifestation of allergy” as serum neuritis rarely occurred in the
absence of (allergic) serum sickness and took 4-12 days to appear (but
at the same time, sometimes that allergic response did not precede serum
neuritis. •Inflammatory edema compressing the nerve fibers (either at the radial groove at the spinal nerve trunks). There was also some debate about whether the edema was in the area surrounding the nerve (perineural) or within it, between the individual nerve fibers (interfascicular). Additionally, in more severe cases also involving the brain, one paper reported edema, small hemorrhages, and interstitial neuritis of the brain, cord, and nerve roots while another on fatal fatal cases of infectious polyneuritis reported strangulation of the nerves at their points of exit from the dura mater. In cases where the brain was directly affected, in addition to a wide range of severe neurological damage occurring, many of changes mirrored what would be expected from a stroke (e.g., half of the body being paralyzed, loss of ability to speak) and like a stroke many of their symptoms persisted for years after the event, while when autopsies that were conducted, most showed extensive demyelination. Of the forms of vaccine encephalitis, post-vaccinal (smallpox) encephalitis was the most studied. Originally, this was viewed as related to encephalitis lethargica, a brain disease which swept across the world between 1915-1926 (affecting roughly 1 million people and killing 500,000)—of which the cause still remains one of the greatest medical mysteries of the 20th century. Notably, the personality changes and behavioral disorders seen in its survivors were very similar to those observed follow DPT brain injuries (e.g., a brilliant book I discussed here made a strong case widespread DPT encephalitis completely changed America society and created many new diseases like ADHD—which previously was widely diagnosed as “minimal brain damage”). Subsequent research showed that the brain lesions of post-vaccinal encephalitis were “indistinguishable” from those seen from viruses like smallpox, chickenpox, measles, and influenza. Attempts to isolate the smallpox vaccine virus (cowpox) from the affected brain or spinal cord tissue all failed, leading to the conclusion that an unknown latent virus was being activated or some type of allergic sensitization was occurring. Key changes detected in the autopsy included: Note: rabies vaccine encephalitis resembled post-infection (or post-vaccine) demyelinating encephalitis, with slight irregular inflammation of the meninges, along with perivascular demyelination and immune cells in the perivascular space and varying degrees of tissue death in both the white and grey matter resembling (and sometimes an elevation in immune cells and protein in the CSF). Lastly, no signs of the rabies virus were found in the brain or upon injection of brain tissue into animals (who instead died from congestion, hemorrhage, perivascular infiltration, diffuse or focal glial and neuronal lesions, and demyelination). •In
children under two, the damage was primarily vascular (e.g., excessive
blood in the brain, blood congestion, perivascular edema, general edema,
and sometimes perivascular hemorrhages) along with widespread
degenerative changes of ganglion cells—all of which were typically
classified as encephalopathy rather than encephalitis. This
encephalopathy was typically sudden, rapidly progressing with severe
neurological symptoms, and in over half the cases fatal within the first
day, at which point a wide range of other lesions were also often
found. However, while the vaccine virus was isolated from throughout the
body, it was typically not found in the congested brain tissue. •“In two or three of the [typhoid] cases it looks rather as if the vaccine had activated a latent or incipient [early stage] disease such as multiple sclerosis,” which dovetails with the longstanding observation vaccines exacerbate pre-existing autoimmune disorders (e.g., I know numerous people who had their MS or Lupus become much worse following COVID vaccination). •While acute encephalitis due to a virus in the brain was seen, this was typically seen following the yellow fever vaccine. •With DPT encephalitis, clinical histories suggested an allergy-mediated form of encephalitis, and in a 1982 report of 70 deaths (and potentially encephalitis or encephalopathy) following DPT, brain edema alongside petechiae (microbleeding) of the internal organs was observed. In one animal experiment, encephalitis was induced by injected rats with rat of guinea pic spinal cords mixed with the pertussis vaccine, which caused extensive perivascular lesions in the central nervous system with enormous numbers of polymorphonuclear leucocytes and demyelination around the vessels, but given the design of the experiment, this could not conclusively be attributed to the vaccine. Note: more modern research on “unexplained” deaths following vaccination has determined that brain congestion and edema are frequently seen (e.g., a 2014study found this in all 13 autopsies of the brain stem, and a 2008 study observed cerebral edema), while more rarely, overt damage is observed (e.g., in one of those 13 autopsies, necrosis, degeneration of myelin-sheaths, and breaking of nerve fibers were observed). Additionally, one study found small intraparenchymal hemorrhages of the spleen and adrenal glands. Vaccine Induced MicrostrokesThe following qualities stand out in these findings: •In
many cases, the damage in the brain occurred without a virus being
present, leading to it being unclear what the mechanism of injury was. •Cranial nerve deficits were often observed. •Congestion was often seen in other parts of the body. •Small hemorrhages were observed from leaking blood vessels. •Many of the observed pathological changes mirrored what was seen in certain severe viral infections Collectively, I believe these can all be explained through zeta potential—a concept that states fluids with suspended particles (colloids) will have varying degrees of dispersion (separation) or aggregation (clumping), which is strongly influenced by the net charge of each particle present, specifically if there is a high density of negative charges that repel each other. Note: the zeta potential concept underlies many diseases (particularly vaccination injuries) and hence was covered in much more detail here (e.g., improving zeta potential cures or improves many complex diseases). Since
this is a systemic effect, it will show up in many parts of the body,
and typically it is easiest to observe via changes in the cranial nerves
(as certain ones are particularly sensitive to a loss of blood flow
from systemic vascular congestion). •This process is not exclusive to vaccines and will also be seen in severe infections (although it is much more frequently caused by vaccination). •Since blood vessels also depend on their own blood supply for nourishment, if that blood supply is cut off, the blood vessels will gradually die and then have small hemorrhages. •When an autoimmune response occurs (which also underlies many of these encephalitic processes and is likewise linked to many vaccines), it will worsen the existing vascular congestion as white blood cells are larger than red blood cells and hence obstruct small blood vessels when they enter them. •In Chinese medicine, “poor zeta potential” is equivalent to “blood stasis” , a condition that in Chinese medicine’s millennia-long history, suddenly came to be viewed as a root cause of disease shortly after the smallpox vaccine entered China. A classic symptom of blood stasis is unusual sharp shooting pains identical to the highly unusual neuralgias observed by Burnett and others. Finally, one author (who I believe drew upon Dr. Andrew Moulden’s work), after noticing how frequently people’s faces were, noticed that in photography from a century ago, those asymmetries were quite rare and argued they were due to vaccine injuries damaging cranial nerves (as the cranial nerves govern many aspects of the face such as the eyes being centered and the facial muscles being even).
Additionally, he observed that those asymmetries were more common in children with autism and was able to propose logical connections between the unusual behaviors autistic children have and specific cranial nerve dysfunctions (many of which I agreed with). Note: because of how doctors are trained, when diagnostic signs of a stroke occur in children, they often aren’t viewed as such (since children don’t “get strokes”) and instead given other diagnoses that recognize the asymmetry but provide no explanation for its cause (e.g., strabismus). Moulden, after realizing many children were developing signs of strokes after vaccination (which often correlated with subsequent neurological injuries) concluded strokes were indeed happening, and that those facial changes provided a critical means to diagnose the brain injuries early on. Revisiting 1986Many consider the 1986 Vaccine Injury Act to have been a turning point in America’s health. By removing the legal liability for producing dangerous products, it incentivized a glut of vaccines to enter the market (e.g., prior to the act, three vaccines [DPT, polio, and MMR] were given, whereas now fifteen are—many of which are given multiple times and, in some cases, annually). In return for this liability exemption, a variety of things were promised to ensure vaccine safety. Unfortunately, in one way or another, much in the same way very few new injuries were added to the vaccine injury table, other than a legal requirement being instituted for vaccines records to include lot numbers (as vaccine companies had gotten out of legal convictions by stating the documentation could not definitively prove it was their vaccine) virtually none of the lawsuits provisions were followed. For example: •Since doctors and health authorities had habitually refused to report vaccine injuries and then used the absence of those reports to argue anyone’s injury was unrelated to vaccination )” there’s no evidence), VAERS, a database the public could directly report to and anyone could analyze was created that physicians were legally required to report. Since that was a huge problem for industry, the CDC deliberately understaffed VAERS (so most reports could not be processed), made it very difficult to report into the system (so most doctors never had the time to) and never enforced mandatory reporting. At the same time, in tandem, the government, medical profession and media for decades denigrated VAERS claiming it was “anecdotal” and often false reports (when in reality extensive studies have shown VAERS captures less than 1% of vaccine injuries—much in the same way the published reports I cited here are likely a tiny fraction of the injuries that actually occurred). Note: had VAERS not been available and provided a way to bypass the widespread censorship of COVID-19 vaccine injuries, it would have been much harder to stop the shots as virtually all other safety data was withheld from the public. Remarkably, we were able to subsequently demonstrate that the CDC broke the law and either did not enter VAERS reports or deleted ones that had been in the system (as members of React19 jointly audited what happened to their injury reports). •Individuals who could not be compensated through the injury program, in certain instances (e.g., from a defective vaccine being made that then injured them), were supposed to be able to sue through the conventional courts. However, in 2011, the Supreme Court effectively removed this provision from the law thereby making it virtually impossible to sue a dangerous vaccine. •A
National Vaccine Advisory Committee (which required at least one member
to come from a vaccine safety group) was to be established in part to
help facilitate the production of safe vaccines. Reviewing their entire history since 1987,
I noticed that they had done much to promote vaccination and assert
their safety but very little to ensure their safety. Specifically the
only instances I could find were a 1996 proposal they proposed adding a $0.05 tax to vaccines to pay for safety studies (which was never implemented), a 2002 determination
that a rotavirus vaccine which was withdrawn in 1999 for causing
intussusception caused intussusception (very rarely) caused it and
publishing a 2011 white paper with very basic suggestions for improving vaccine safety. •In
1986, there were significant concerns that the pertussis antigen was
linked to hemolytic anemia, hypsarrhythmia, infantile spasms, Reye’s
syndrome, peripheral mononeuropathy, SIDS, aseptic meningitis, juvenile
diabetes, autism, learning disabilities,
and hyperactivity. While evidence supported these links, the scientific
community rejected it since it was not “robust” enough. As such, the law
mandated that the H.H.S. would conduct studies on its link to each of
these. To the best of my knowledge, none of those studies were ever
done, and instead for each condition, the Institute of Medicine (IOM)
assessed the link, and concluded, based on the available literature,
that there was no link. As I was extensively familiar with the
literature on SIDS and Autism, I reviewed those reports, had serious
disagreements with their methodology and conclusions, and hence assumed
something similar happened for the other IOM vaccine reports. •Required reports every 1-2 years to be sent by H.H.S. leadership (e.g., the H.H.S. Secretary) to Congress about the progress being made towards vaccine safety. In 2018, ICAN and RFK Jr. sued the H.H.S. through the Freedom of Information Act, and after 8 months of H.H.S. stalling, learned that no reports were ever made. A New HopeIf you look at the history of vaccination, the same issues have recurred ever since they were first created (e.g., unusual but similar neurologic injuries, everyone robotically existing they are “safe and effective” even while fully aware of evidence to the contrary and the medical community doing all it could to cover most of them up for the “greater good”). In turn, this lack of accountability has led to more and more brazen attempts to push these profitable products on the marketplace. Since this led to more and more toxic products being unleashed (culminating in the COVID vaccines caused a previously inconceivable degree of neurological and autoimmune injuries) more and more aggressive censorship measures were needed to preserve their illusion of safety. Sadly however, COVID-19 was not the first time this playbook of silence was needed:
Note: preventing “vaccine hesitancy” is continually used as an excuse by doctors and health authorities for covering up vaccine injuries (e.g., to quote a recent NYT article COVID vaccine injuries: “and vaccine supporters, including federal officials, worry that even a whisper of possible side effects feeds into misinformation spread by a vitriolic anti-vaccine movement”). Had a basic accountability level been implemented, the COVID vaccine disaster likely would have never happened. This is demonstrated by the FDA’s rushed 2006 approval for an unproven, unneeded, and already known to be very dangerous HPV vaccine which quickly severely injured a large number of children with a wide range of neurological and autoimmune disorders. However, in response to the deluge of injuries from the vaccine and public protest against these injuries, the FDA simply said “safe and effective” then in response to public pressure conducted a 2009 study on its relative rate of adverse events compared to other vaccines. That study found over three times as many injuries were being reported for Gardasil as all other vaccines combined, a finding the FDA then chose to deem “unrelated” and ignored. Fortunately, COVID-19 at last passed the breaking point and because of how harmful and ineffective the mandatory “100% safe and effective” vaccines were, a political movement was born which put RFK, someone who had litigated against the H.H.S. for years on its failure to ensure vaccine safety in charge of it. Since the failures of the 1986 law were essentially due to the H.H.S. Secretary having the discretion to implement the provisions aimed at vaccine safety (all of which every Secretary then never did), RFK’s nomination was an existential threat to an industry that had relied upon blanket immunity and no government scrutiny. As such, during his confirmation hearings, he was relentlessly attacked by Democrats over his positions on vaccination. Within that exchange, a few points stood out: •RFK said he would not ban vaccines, but rather wanted better research on their safety. In response, his detractors all said all the research had already been done and vaccine safety was settled science, so there was no need for more of it—when in reality, the basic (and required) studies needed to assess vaccine safety conclusively still have not been done. •RFK was repeatedly accused of having a massive conflict of interest to “make it easier to sue vaccine manufacturers” since he had previously worked in vaccine litigation, whereas in contrast I’ve never seen a pharmaceutical CEO be criticized for then leading the H.H.S. (and remarkably, RFK was actually criticized by a hostile Senator for not being a pharmaceutical CEO). •Those “conflicts” were then used by multiple senators to pressure RFK into agreeing not to change anything related to H.H.S. vaccine policy that could make it easier for lawsuits to be filed (e.g., here Elizabeth Warren belligerently attacked RFK for the possibility he would do what the 1986 law explicitly requires the H.H.S. Secretary to do), and repeatedly argued it would be a national disaster if RFK did anything to make it easier to have vaccine injury lawsuits as that would bankrupt the [“very safe”] industry. •Cassidy, a pro-vaccine doctor and Republican Senator used his pivotal confirmation vote to force RFK Jr. to agree to a variety of highly unusual provisions (that greatly handicapped his ability to improve vaccine safety) such as RFK Jr. having to run his appointees by Cassidy, have monthly meetings to ensure RFK Jr.’s compliance, prohibiting RFK Jr. from fixing VAERS or creating another vaccine monitoring system, requiring any changes he made to vaccines to be approved by a committee Cassidy could place someone on, and having a Congressional hearing anytime RFK Jr. changed something affected vaccines. As such, since becoming HHS Secretary, RFK Jr. has had to take a much slower approach to ensuring vaccine safety and instead has focused on the “less controversial” aspects of MAHA (e.g., food safety), while a tremendous amount of work has gone into getting the right political appointees who can pass both the Senate and Cassidy, so despite working at a frantic speed, RFK Jr. has thus only just begun touching on vaccine safety. For example, on April 30th he announced all new vaccines would need to be tested against placebo (which never happens since vaccines have so many side effects using a real placebo that did not conceal injuries would cause them to fail their trials (e.g., half of the Gardasil trial participants developed “new medical conditions,” many of which were autoimmune or neurological, so to hide this, they were given a toxic “placebo” which also caused those injuries ). This seemingly reasonable decision created an uproar throughout the entire media (which fortunately woke many up to the fact the vaccines they assume are robustly tested have never actually been tested against placebo):
Note: in placebo trials, subjects are not exposed to the infection, and in the last 30 years, there has only been one case of polio in the United States (which came from a vaccine). ConclusionOne of the major problems in both government and medicine is that since everything is predicated on past actions (including how people are trained to approach problems), bad decisions have an incredible degree of inertia and frequently perpetuate for generations despite widespread outcry against them. For example, in a recent article, I showed how the first head of the FDA was unable to take toxic food additives off the market he fought for years to outlaw because Teddy Roosevelt did not like his favorite artificial sweetener being scrutinized. In turn, it is only now, over a century later that RFK Jr. is addressing that fiasco. Similarly, in the case of vaccines and serums, at the time they were developed, there were no (mainstream) alternatives to treat many of these deadly diseases. This hence lead to a mentality becoming entrenched that the harsh side effects of the vaccines or serums were justified to treat those life-threatening illnesses, and that it was ethical to lie about those harms so people would get the life saving therapies. Now, the circulating diseases are far less deadly and we have a myriad of mainstream therapies that can treat them (and leave the recipient with robust natural immunity), but again due to inertia, this outdated and erroneous mentality persists. At this moment, we have a once in a lifetime opportunity to break this inertia. The MAHA coalition was large enough to win the 2024 election that it not only earned RFK Jr. a seat at the table, but as mainstream sources acknowledge, led to the Trump administration giving RFK Jr. an extraordinary degree of freedom to enact the MAHA agenda as delivering for MAHA will be necessary to win the 2026 midterms. In America’s entire history, there has never been a dedicated public servant in the position RFK is in. However, even with that, there are still immense limitations on what he can do. For example, Cassidy has required “ironclad causational scientific evidence that can be accepted and defended before the mainstream scientific community and Congress” for RFK to take a vaccine off the market or even stop recommending it. Since that standard is impossible to meet (e.g., many in Congress continued to push the COVID vaccine even after it killed their children or gave them severe neurological injuries), there are only two options. The first is to continue building the momentum for MAHA (e.g., with political victories on softer topics like food dyes). The second is to create grassroots support for the policies we are all trying to implement (particularly complete data transparency surrounding vaccination) until it swells enough (e.g. due to costly pharmaceutical boycotts) that even industry holdouts are forced to acknowledge it. That will require understanding exactly what we’ve been lied to about vaccines, which is why I worked so hard to write this article. Many people I am close to over the decades have suffered similar severe neurologic injuries from vaccines, and now is when we need to work together to end that. Likewise, while many profoundly debilitating vaccine injuries are treatable, those treatments will never become available unless injuries are acknowledged in the first place (which has not been done as doing so would create vaccine-skepticism and reduce vaccine sales). Your incredible support is what makes it possible for me to set aside the time to create these articles (this one took a while). I deeply thank you for giving me the opportunity to finally be able to give a voice to all those injured by these products and at last make it possible to end this abhorrent cycle that has defined our society for centuries. To learn how other readers have benefitted from this publication and the community it has created, their feedback can be viewed here. Additionally, an index of all the articles published in the Forgotten Side of Medicine can be viewed here. You're currently a free subscriber to The Forgotten Side of Medicine. For the full experience, upgrade your subscription. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||
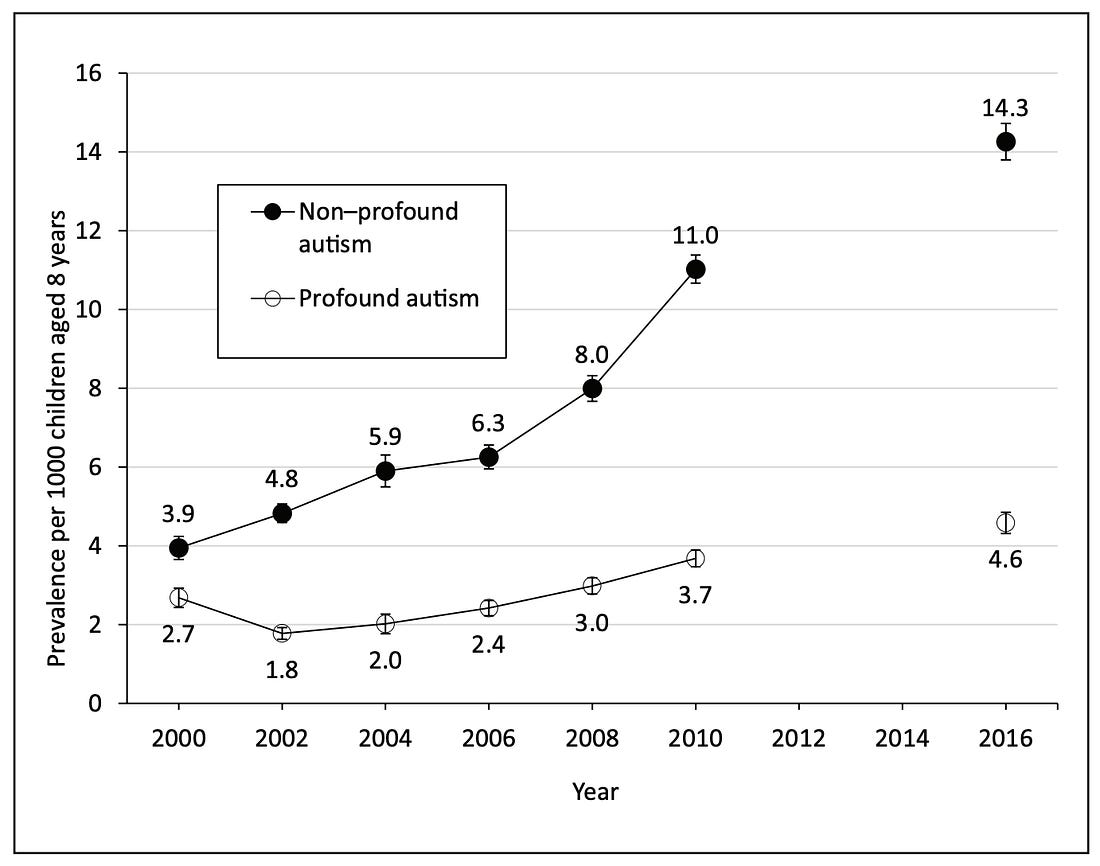
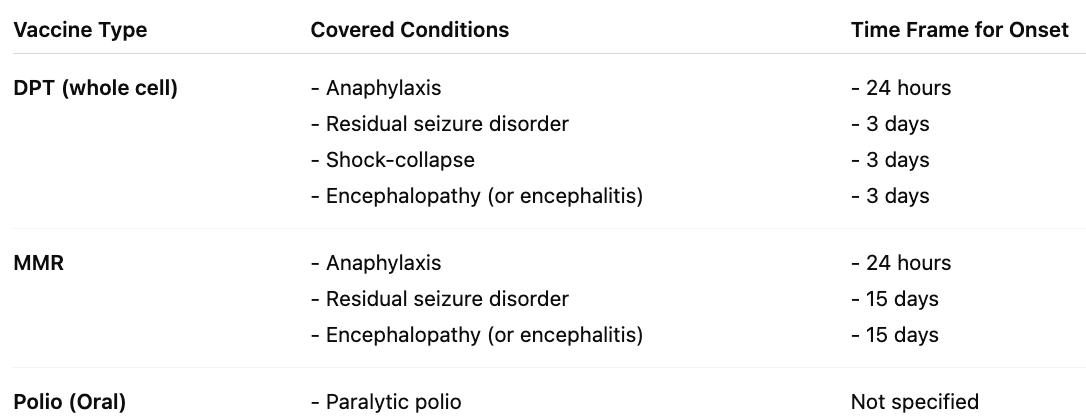
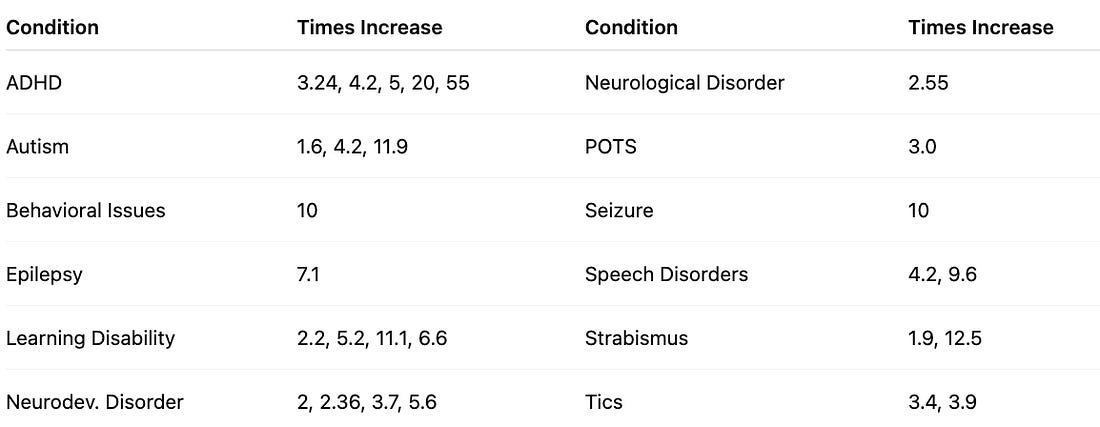
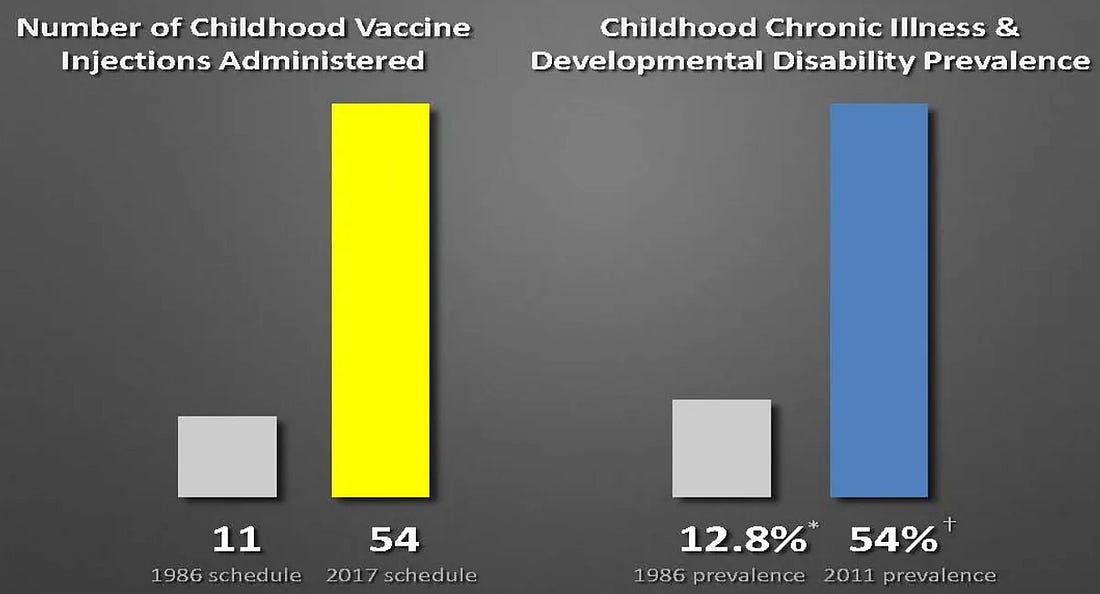
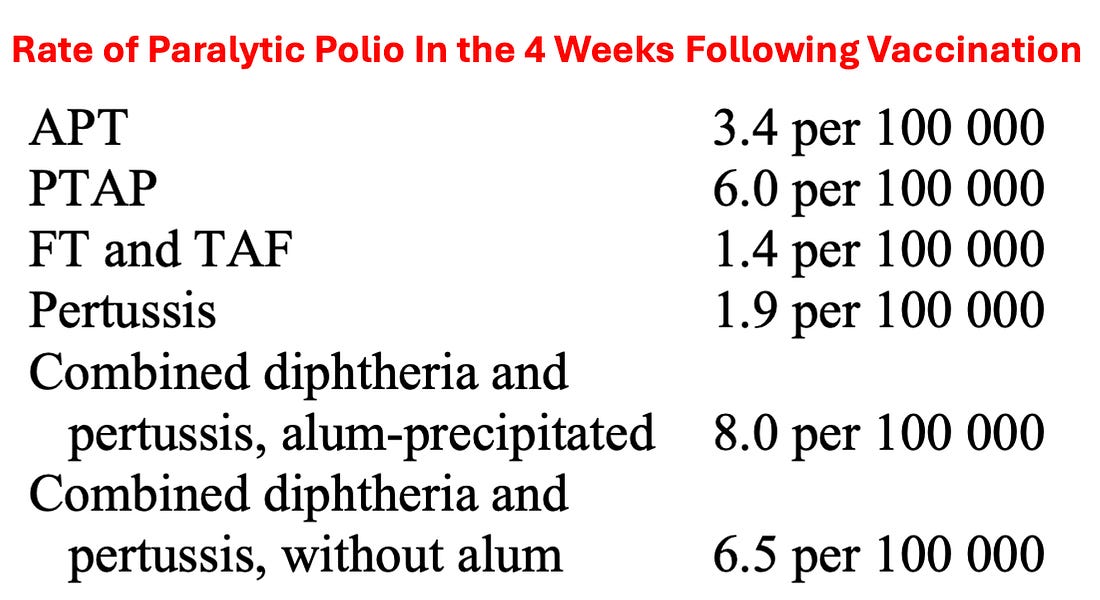


No comments:
Post a Comment