The COVID-19 RT-PCR Test: How to Mislead All Humanity. Using a “Test” To Lock Down Society
It is time for everyone to come out of this negative trance, this collective hysteria, because famine, poverty, massive unemployment will kill, mow down many more people than SARS-CoV-2!



First published by Global Research on November 5, 2020
Introduction: using a technique to lock down society
All current propaganda on the COVID-19 pandemic is based on an assumption that is considered obvious, true and no longer questioned:
Positive RT-PCR test means being sick with COVID. This assumption is misleading.
Very few people, including doctors, understand how a PCR test works.
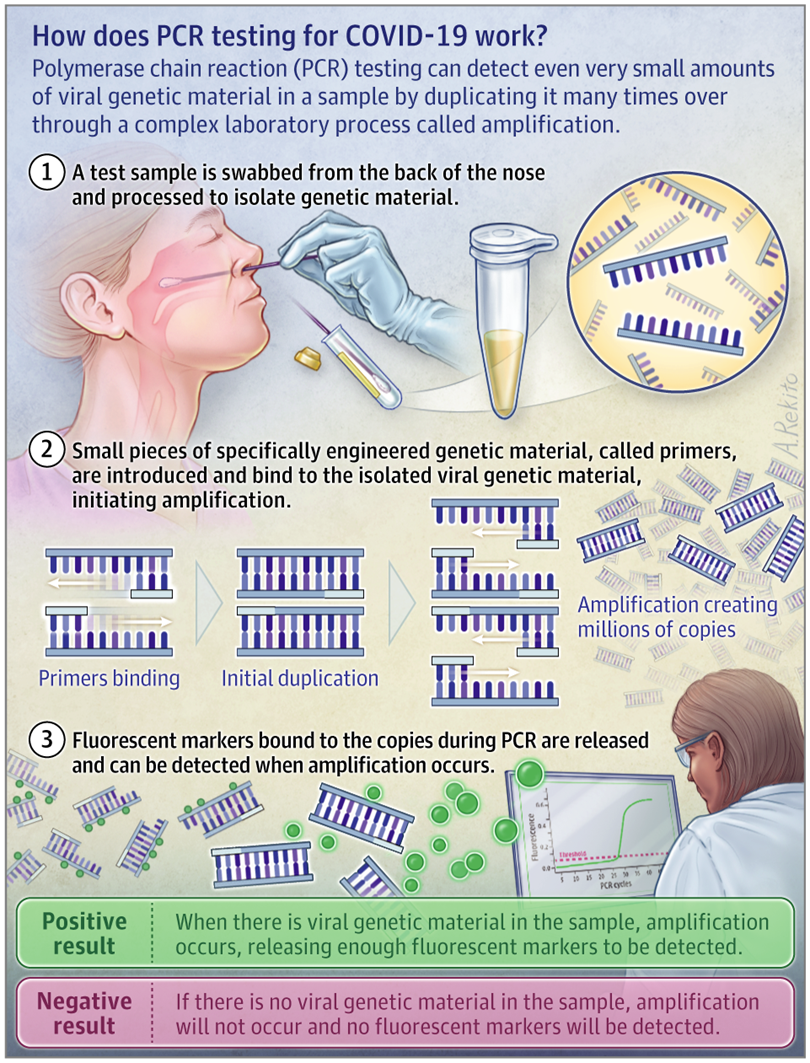
RT-PCR means Real Time-Polymerase Chain Reaction.
In French, it means: Réaction de Polymérisation en Chaîne en Temps Réel.
In medicine, we use this tool mainly to diagnose a viral infection.
Starting from a clinical situation with the presence or absence of particular symptoms in a patient, we consider different diagnoses based on tests.
In the case of certain infections, particularly viral infections, we use the RT-PCR technique to confirm a diagnostic hypothesis suggested by a clinical picture.
We do not routinely perform RT-PCR on any patient who is overheated, coughing or has an inflammatory syndrome!
It is a laboratory, molecular biology technique of gene amplification because it looks for gene traces (DNA or RNA) by amplifying them.
In addition to medicine, other fields of application are genetics, research, industry and forensics.
The technique is carried out in a specialized laboratory, it cannot be done in any laboratory, even a hospital. This entails a certain cost, and a delay sometimes of several days between the sample and the result.
Today, since the emergence of the new disease called COVID-19 (COrona VIrus Disease-2019), the RT-PCR diagnostic technique is used to define positive cases, confirmed as SARS-CoV-2 (coronavirus responsible for the new acute respiratory distress syndrome called COVID-19).
These positive cases are assimilated to COVID-19 cases, some of whom are hospitalized or even admitted to intensive care units.
Official postulate of our managers: positive RT-PCR cases = COVID-19 patients. [1]
This is the starting postulate, the premise of all official propaganda, which justifies all restrictive government measures: isolation, confinement, quarantine, mandatory masks, color codes by country and travel bans, tracking, social distances in companies, stores and even, even more importantly, in schools [2].
This misuse of RT-PCR technique is used as a relentless and intentional strategy by some governments, supported by scientific safety councils and by the dominant media, to justify excessive measures such as the violation of a large number of constitutional rights, the destruction of the economy with the bankruptcy of entire active sectors of society, the degradation of living conditions for a large number of ordinary citizens, under the pretext of a pandemic based on a number of positive RT-PCR tests, and not on a real number of patients.
Technical aspects: to better understand and not be manipulated
The PCR technique was developed by chemist Kary B. Mullis in 1986. Kary Mullis was awarded the Nobel Prize in Chemistry in 1993.
Although this is disputed [3], Kary Mullis himself is said to have criticized the interest of PCR as a diagnostic tool for an infection, especially a viral one.
He stated that if PCR was a good tool for research, it was a very bad tool in medicine, in the clinic [4].
Mullis was referring to the AIDS virus (HIV retrovirus or HIV) [5], before the COVID-19 pandemic, but this opinion on the limitation of the technique in viral infections [6], by its creator, cannot be dismissed out of hand; it must be taken into account!
PCR was perfected in 1992.
As the analysis can be performed in real time, continuously, it becomes RT (Real-Time) – PCR, even more efficient.
It can be done from any molecule, including those of the living, the nucleic acids that make up the genes:
- DNA (deoxyribonucleic acid)
- RNA (Ribonucleic Acid)
Viruses are not considered as “living” beings, they are packets of information (DNA or RNA) forming a genome.
It is by an amplification technique (multiplication) that the molecule sought is highlighted and this point is very important.
RT-PCR is an amplification technique [7].
If there is DNA or RNA of the desired element in a sample, it is not identifiable as such.
This DNA or RNA must be amplified (multiplied) a certain number of times, sometimes a very large number of times, before it can be detected. From a minute trace, up to billions of copies of a specific sample can be obtained, but this does not mean that there is all that amount in the organism being tested.
In the case of COVID-19, the element sought by RT-PCR is SARS-CoV-2, an RNA virus [8].
There are DNA viruses such as Herpes and Varicella viruses.
The most well known RNA viruses, in addition to coronaviruses, are Influenza, Measles, EBOLA, ZIKA viruses.
In the case of SARS-CoV-2, RNA virus, an additional specific step is required, a transcription of RNA into DNA by means of an enzyme, Reverse Transcriptase.
This step precedes the amplification phase.
It is not the whole virus that is identified, but sequences of its viral genome.
This does not mean that this gene sequence, a fragment of the virus, is not specific to the virus being sought, but it is an important nuance nonetheless:
RT-PCR does not reveal any virus, but only parts, specific gene sequences of the virus.
At the beginning of the year, the SARS-CoV-2 genome was sequenced.
It consists of about 30,000 base pairs. The nucleic acid (DNA-RNA), the component of the genes, is a sequence of bases. In comparison, the human genome has more than 3 billion base pairs.
Teams are continuously monitoring the evolution of the SARS-CoV-2 viral genome as it evolves [9-10-11], through the mutations it undergoes. Today, there are many variants [12].
By taking a few specific genes from the SARS-CoV-2 genome, it is possible to initiate RT-PCR on a sample from the respiratory tract.
For COVID-19 disease, which has a nasopharyngeal (nose) and oropharyngeal (mouth) entry point, the sample should be taken from the upper respiratory tract as deeply as possible in order to avoid contamination by saliva in particular.
ll the people tested said that it is very painful [13].
The Gold Standard (preferred site for sampling) is the nasopharyngeal (nasal) approach, the most painful route.
If there is a contraindication to the nasal approach, or preferably to the individual being tested, depending on the official organs, the oropharyngeal approach (through the mouth) is also acceptable. The test may trigger a nausea/vomiting reflex in the individual being tested.
Normally, for the result of an RT-PCR test to be considered reliable, amplification from 3 different genes (primers) of the virus under investigation is required.
“The primers are single-stranded DNA sequences specific to the virus. They guarantee the specificity of the amplification reaction. » [14]
“The first test developed at La Charité in Berlin by Dr. Victor Corman and his associates in January 2020 allows to highlight the RNA sequences present in 3 genes of the virus called E, RdRp and N. To know if the sequences of these genes are present in the RNA samples collected, it is necessary to amplify the sequences of these 3 genes in order to obtain a signal sufficient for their detection and quantification. »[15].
The essential notion of Cycle Time or Cycle Threshold or Ct positivity threshold [16].
An RT-PCR test is negative (no traces of the desired element) or positive (presence of traces of the desired element).
However, even if the desired element is present in a minute, negligible quantity, the principle of RT-PCR is to be able to finally highlight it by continuing the amplification cycles as much as necessary.
RT-PCR can push up to 60 amplification cycles, or even more!
Here is how it works:
Cycle 1: target x 2 (2 copies)
Cycle 2: target x 4 (4 copies)
Cycle 3: target x 8 (8 copies)
Cycle 4: target x 16 (16 copies)
Cycle 5; target x 32 (32 copies)
Etc exponentially up to 40 to 60 cycles!
When we say that the Ct (Cycle Time or Cycle Threshold or RT-PCR positivity threshold) is equal to 40, it means that the laboratory has used 40 amplification cycles, i.e. obtained 240 copies.
This is what underlies the sensitivity of the RT-PCR assay.
While it is true that in medicine we like to have high specificity and sensitivity of the tests to avoid false positives and false negatives, in the case of COVID-19 disease, this hypersensitivity of the RT-PCR test caused by the number of amplification cycles used has backfired.
This over-sensitivity of the RT-PCR test is deleterious and misleading!
It detaches us from the medical reality which must remain based on the real clinical state of the person: is the person ill, does he or she have symptoms?
That is the most important thing!
As I said at the beginning of the article, in medicine we always start from the person: we examine him/her, we collect his/her symptoms (complaints-anamnesis) and objective clinical signs (examination) and on the basis of a clinical reflection in which scientific knowledge and experience intervene, we make diagnostic hypotheses.
Only then do we prescribe the most appropriate tests, based on this clinical reflection.
We constantly compare the test results with the patient’s clinical condition (symptoms and signs), which takes precedence over everything else when it comes to our decisions and treatments.
Today, our governments, supported by their scientific safety advice, are making us do the opposite and put the test first, followed by a clinical reflection necessarily influenced by this prior test, whose weaknesses we have just seen, particularly its hypersensitivity.
None of my clinical colleagues can contradict me.
Apart from very special cases such as genetic screening for certain categories of populations (age groups, sex) and certain cancers or family genetic diseases, we always work in this direction: from the person (symptoms, signs) to the appropriate tests, never the other way around.
This is the conclusion of an article in the Swiss Medical Journal (RMS) published in 2007, written by doctors Katia Jaton and Gilbert Greub microbiologists from the University of Lausanne :
PCR in microbiology: from DNA amplification to result interpretation:
“To interpret the result of a PCR, it is essential that clinicians and microbiologists share their experiences, so that the analytical and clinical levels of interpretation can be combined.”
It would be indefensible to give everyone an electrocardiogram to screen everyone who might have a heart attack one day.
On the other hand, in certain clinical contexts or on the basis of specific evocative symptoms, there, yes, an electrocardiogram can be beneficial.
Back to RT-PCR and Ct (Cycle Time or Cycle Threshold).
In the case of an infectious disease, especially a viral one, the notion of contagiousness is another important element.
Since some scientific circles consider that an asymptomatic person can transmit the virus, they believe it is important to test for the presence of virus, even if the person is asymptomatic, thus extending the indication of RT-PCR to everyone.
Are RT-PCR tests good tests for contagiousness? [17]
This question brings us back to the notion of viral load and therefore Ct.
The relationship between contagiousness and viral load is disputed by some people [18] and no formal proof, to date, allows us to make a decision.
However, common sense gives obvious credence to the notion that the more virus a person has inside him or her, especially in the upper airways (oropharynx and nasopharynx), with symptoms such as coughing and sneezing, the higher the risk of contagiousness, proportional to the viral load and the importance of the person’s symptoms.
This is called common sense, and although modern medicine has benefited greatly from the contribution of science through statistics and Evidence-Based Medicine (EBM), it is still based primarily on common sense, experience and empiricism.
Medicine is the art of healing.
No test measures the amount of virus in the sample!
RT-PCR is qualitative: positive (presence of the virus) or negative (absence of the virus).
This notion of quantity, therefore of viral load, can be estimated indirectly by the number of amplification cycles (Ct) used to highlight the virus sought.
The lower the Ct used to detect the virus fragment, the higher the viral load is considered to be (high).
The higher the Ct used to detect the virus fragment, the lower the viral load is considered to be (low).
Thus, the French National Reference Centre (CNR), in the acute phase of the pandemic, estimated that the peak of viral shedding occurred at the onset of symptoms, with an amount of virus corresponding to approximately 108 (100 million) copies of SARS-CoV-2 viral RNA on average (French COVID-19 cohort data) with a variable duration of shedding in the upper airways (from 5 days to more than 5 weeks) [19].
This number of 108 (100 million) copies/μl corresponds to a very low Ct.
A Ct of 32 corresponds to 10-15 copies/μl.
A Ct of 35 corresponds to about 1 copy/μl.
Above Ct 35, it becomes impossible to isolate a complete virus sequence and culture it!
In France and in most countries, Ct levels above 35, even 40, are still used even today!
The French Society of Microbiology (SFM) issued an opinion on September 25, 2020 in which it does not recommend quantitative results, and it recommends to make positive up to a Ct of 37 for a single gene [20]!
With 1 copy/μl of a sample (Ct 35), without cough, without symptoms, one can understand why all these doctors and scientists say that a positive RT-PCR test means nothing, nothing at all in terms of medicine and clinic!
Positive RT-PCR tests, without any mention of Ct or its relation to the presence or absence of symptoms, are used as is by our governments as the exclusive argument to apply and justify their policy of severity, austerity, isolation and aggression of our freedoms, with the impossibility to travel, to meet, to live normally!
There is no medical justification for these decisions, for these governmental choices!
In an article published on the website of the New York Times (NYT) on Saturday, August 29, American experts from Harvard University are surprised that RT-PCR tests as practiced can serve as tests of contagiousness, even more so as evidence of pandemic progression in the case of SARS-CoV-2 infection [21].
According to them, the threshold (Ct) considered results in positive diagnoses in people who do not represent any risk of transmitting the virus!
The binary “yes/no” answer is not enough, according to this epidemiologist from the Harvard University School of Public Health.
“It’s the amount of virus that should dictate the course of action for each patient tested. »
The amount of virus (viral load); but also and above all the clinical state, symptomatic or not of the person!
This calls into question the use of the binary result of this RT-PCR test to determine whether a person is contagious and must follow strict isolation measures.
These questions are being raised by many physicians around the world, not only in the United States but also in France, Belgium (Belgium Health Experts Demand Investigation Of WHO For Faking Coronavirus Pandemic), France, Germany, Italy, the United Kingdom, the United States and the United Kingdom. in Germany, Spain…
According to them: “We are going to put tens of thousands of people in confinement, in isolation, for nothing. » [22]. 22] And inflict suffering, anguish, economic and psychological dramas by the thousands!
Most RT-PCR tests set the Ct at 40, according to the NYT. Some set it at 37.
“Tests with such high thresholds (Ct) may not only detect live virus but also gene fragments, remnants of an old infection that do not represent any particular danger,” the experts said.
A virologist at the University of California admits that an RT-PCR test with a Ct greater than 35 is too sensitive. “A more reasonable threshold would be between 30 and 35,” she adds.
Almost no laboratory specifies the Ct (number of amplification cycles performed) or the number of copies of viral RNA per sample μl.
Here is an example of a laboratory result (approved by Sciensano, the Belgian national reference center) in an RT-PCR negative patient:

No mention of Ct.
In the NYT, experts compiled three datasets with officials from the states of Massachusetts, New York and Nevada that mention them.
Conclusion?
“Up to 90% of the people who tested positive did not carry a virus. »
The Wadworth Center, a New York State laboratory, analyzed the results of its July tests at the request of the NYT: 794 positive tests with a Ct of 40.
“With a Ct threshold of 35, approximately half of these PCR tests would no longer be considered positive,” said the NYT.
“And about 70% would no longer be considered positive with a Ct of 30! “
In Massachusetts, between 85 and 90% of people who tested positive in July with a Ct of 40 would have been considered negative with a Ct of 30, adds the NYT. And yet, all these people had to isolate themselves, with all the dramatic psychological and economic consequences, while they were not sick and probably not contagious at all.
In France, the Centre National de Référence (CNR), the French Society of Microbiology (SFM) continue to push Ct to 37 and recommend to laboratories to use only one gene of the virus as a primer.
I remind you that from Ct 32 onwards, it becomes very difficult to culture the virus or to extract a complete sequence, which shows the completely artificial nature of this positivity of the test, with such high Ct levels, above 30.
Similar results were reported by researchers from the UK Public Health Agency in an article published on August 13 in Eurosurveillance: “The probability of culturing the virus drops to 8% in samples with Ct levels above 35.” [23]
In addition, currently, the National Reference Center in France only evaluates the sensitivity of commercially available reagent kits, not their specificity: serious doubts persist about the possibility of cross-reactivity with viruses other than SARS-CoV-2, such as other benign cold coronaviruses. [20]
It is potentially the same situation in other countries, including Belgium.
Similarly, mutations in the virus may have invalidated certain primers (genes) used to detect SARS-CoV-2: the manufacturers give no guarantees on this, and if the AFP fast-checking journalists tell you otherwise, test their good faith by asking for these guarantees, these proofs.
If they have nothing to hide and if what I say is false, this guarantee will be provided to you and will prove their good faith.
- We must demand that the RT-PCR results be returned mentioning the Ct used because beyond Ct 30, a positive RT-PCR test means nothing.
- We must listen to the scientists and doctors, specialists, virologists who recommend the use of adapted Ct, lower, at 30. An alternative is to obtain the number of copies of viral RNA/μl or /ml sample. [23]
- We need to go back to the patient, to the person, to his or her clinical condition (presence or absence of symptoms) and from there to judge the appropriateness of testing and the best way to interpret the result.
Until there is a better rationale for PCR screening, with a known and appropriate Ct threshold, an asymptomatic person should not be tested in any way.
Even a symptomatic person should not automatically be tested, as long as they can place themselves in isolation for 7 days.
Let’s stop this debauchery of RT-PCR testing at too high Ct levels and return to clinical, quality medicine.
Once we understand how RT-PCR testing works, it becomes impossible to let the current government routine screening strategy, inexplicably supported by the virologists in the safety councils, continue.
My hope is that, finally, properly informed, more and more people will demand that this strategy be stopped, because it is all of us, enlightened, guided by real benevolence and common sense, who must decide our collective and individual destinies.
No one else should do it for us, especially when we realize that those who decide are no longer reasonable or rational.
Summary of important points :
- The RT-PCR test is a laboratory diagnostic technique that is not well suited to clinical medicine.
- It is a binary, qualitative diagnostic technique that confirms (positive test) or not (negative test) the presence of an element in the medium being analyzed. In the case of SARS-CoV-2, the element is a fragment of the viral genome, not the virus itself.
- In medicine, even in an epidemic or pandemic situation, it is dangerous to place tests, examinations, techniques above clinical evaluation (symptoms, signs). It is the opposite that guarantees quality medicine.
- The main limitation (weakness) of the RT-PCR test, in the current pandemic situation, is its extreme sensitivity (false positive) if a suitable threshold of positivity (Ct) is not chosen. Today, experts recommend using a maximum Ct threshold of 30.
- This Ct threshold must be informed with the positive RT-PCR result so that the physician knows how to interpret this positive result, especially in an asymptomatic person, in order to avoid unnecessary isolation, quarantine, psychological trauma.
- In addition to mentioning the Ct used, laboratories must continue to ensure the specificity of their detection kits for SARS-CoV-2, taking into account its most recent mutations, and must continue to use three genes from the viral genome being studied as primers or, if not, mention it.
Overall Conclusion
Is the obstinacy of governments to use the current disastrous strategy, systematic screening by RT-PCR, due to ignorance?
Is it due to stupidity?
To a kind of cognitive trap trapping their ego?
In any case, we should be able to question them, and if among the readers of this article there are still honest journalists, or naive politicians, or people who have the possibility to question our rulers, then do so, using these clear and scientific arguments.
It is all the more incomprehensible that our rulers have surrounded themselves with some of the most experienced specialists in these matters.
If I have been able to gather this information myself, shared, I remind you, by competent people above all suspicion of conspiracy, such as Hélène Banoun, Pierre Sonigo, Jean-François Toussaint, Christophe De Brouwer, whose intelligence, intellectual honesty and legitimacy cannot be questioned, then the Belgian, French and Quebec scientific advisors, etc., know all this as well.
So?
What’s going on?
Why continue in this distorted direction, obstinately making mistakes?
It is not insignificant to reimpose confinements, curfews, quarantines, reduced social bubbles, to shake up again our shaky economies, to plunge entire families into precariousness, to sow so much fear and anxiety generating a real state of post-traumatic stress worldwide, to reduce access to care for other pathologies that nevertheless reduce life expectancy much more than COVID-19! [24]
Is there intent to harm?
Is there an intention to use the alibi of a pandemic to move humanity towards an outcome it would otherwise never have accepted? In any case, not like that!
Would this hypothesis, which modern censors will hasten to label “conspiracy”, be the most valid explanation for all this?
Indeed, if we draw a straight line from the present events, if they are maintained, we could find ourselves once again confined with hundreds, thousands of human beings forced to remain inactive, which, for the professions of catering, entertainment, sales, fairgrounds, itinerants, canvassers, risks being catastrophic with bankruptcies, unemployment, depression, suicides by the hundreds of thousands. [25-26-27-28]
The impact on education, on our children, on teaching, on medicine with long planned care, operations, treatments to be cancelled, postponed, will be profound and destructive.
“We risk a looming food crisis if action is not taken quickly.” [29].
It is time for everyone to come out of this negative trance, this collective hysteria, because famine, poverty, massive unemployment will kill, mow down many more people than SARS-CoV-2!
Does all this make sense in the face of a disease that is declining, over-diagnosed and misinterpreted by this misuse of overly sensitively calibrated PCR tests?
For many, the continuous wearing of the mask seems to have become a new norm.
Even if it is constantly downplayed by some health professionals and fact-checking journalists, other doctors warn of the harmful consequences, both medical and psychological, of this hygienic obsession which, maintained permanently, is in fact an abnormality!
What a hindrance to social relations, which are the true foundation of a physically and psychologically healthy humanity!
Some dare to find all this normal, or a lesser price to pay in the face of the pandemic of positive PCR tests.
Isolation, distancing, masking of the face, impoverishment of emotional communication, fear of touching and kissing even within families, communities, between relatives…
Spontaneous gestures of daily life hindered and replaced by mechanical and controlled gestures …
Terrified children, kept in permanent fear and guilt…
All this will have a deep, lasting and negative impact on human organisms, in their physical, mental, emotional and representation of the world and society.
This is not normal!
We cannot let our rulers, for whatever reason, organize our collective suicide any longer.
Translated from French by Global Research. Original source: Mondialisation.ca
Dr Pascal Sacré is a physician specialized in critical care, author and renowned public health analyst, Charleroi, Belgium. He is a Research Associate of the entre for Research on Globalization (CRG)
****
Professionals whose references and comments are the basis of this article in its scientific aspect (especially and mainly on RT-PCR):
1) Hélène Banoun
https://www.researchgate.net/profile/Helene_Banoun
PhD, Pharmacist biologist
Former INSERM Research Officer
Former intern at the Paris Hospitals
2) Pierre Sonigo
Virologist
Research Director INSERM, worked at the Pasteur Institute
Heads the Virus Genetics Laboratory in Cochin, Paris.
Participated in 1985 in the sequencing of the AIDS virus.
3) Christophe De Brouwer
PhD in Public Health Science
Honorary Professor at the School of Public Health at ULB, Belgium
4) Jean-François Toussaint
Doctor, Professor of Physiology at the University of Paris-Descartes
Director of IRMES, Institute for BioMedical Research and Sports Epidemiology
Former member of the High Council of Public Health
***
Notes (French)
[1] “Une nette augmentation du nombre de cas dans toutes les provinces et toutes les tranches d’âge”, 7sur7 ACTU Belgique, 5-10-2020
[2] Le gouvernement belge renforce des mesures anti-Covid, VRT.be ; 6 octobre 2020.
[3] Non, l’inventeur du test PCR n’a pas dit que sa méthode était inefficace pour détecter les virus, dans Le Monde, 7 octobre 2020
[4] Kary Mullis : « Le test PCR ne permet pas de savoir si vous êtes malade », vidéo accessible sur YouTube, 9 octobre 2020.
[6] « The Truth about PCR Test Kit from the Inventor and Other Experts »
[7] PCR en microbiologie : de l’amplification de l’ADN à l’interprétation du résultat
[8] COVID : La PCR nasale peut-elle mentir ?, Dr Pascal Sacré, AIMSIB, 30 août 2020.
[9] https://www.youtube.com/watch?v=CaAcSJI0oMs&feature=youtu.be, 8 octobre 2020. Évolution génomique des virus ARN à l’Institut Pasteur, environ la moitié des nucléotides sont susceptibles d’avoir muté sur les 30 000 nucléotides de l’ARN viral. « Pour l’instant aucune mutation ou délétion n’a été associée à une perte de sévérité de la maladie sur une grande échelle géographique mais de nombreuses publications devraient bientôt préciser ces points. »
[10] https://www.mediterranee-infection.com/wp-content/uploads/2020/04/FD_Raoult_SARS-CoV-2_EID_Sep2020_vL2.pdf, Article IHU-Méditerranée, Professeur D. Raoult, Dramatic increase in the SARS-CoV-2 mutation rate and low mortality rate during the second epidemic in summer in Marseille, 7 septembre 2020
Conclusions :
Dans l’ensemble, comme l’ont récemment souligné Tomaszewski et al. (7) qui ont décrit pour les génomes viraux disponibles jusqu’en mai 2020 un déplacement mutationnel sur la spike et le complexe de réplication vers des gènes codant pour d’autres protéines non structurelles qui interagissent avec les voies de défense de l’hôte, il semble que le taux de mutation du SARS-CoV-2 s’accélère depuis mai, impliquant principalement des mutations C vers U. L’augmentation du taux de mutation du SRAS-CoV-2 génère des génotypes viraux plus éloignés de la souche Wuhan initiale que ceux observés de mars à avril. Cela semble entraîner des épidémies de durée limitée, du moins pour le premier nouveau génotype que nous avons identifié, et est associé à une gravité globalement moindre à ce stade du développement de cette nouvelle épidémie.
Mutations observed in these seven different viral genotypes are located in most SARS- CoV-2 genes including structural and non-structural genes among which nsp2, nsp3 (predicted phosphoesterase), nsp5 (membrane glycoprotein), nsp12 (RNA-dependent RNA polymerase), S (Spike glycoprotein), ORF3a, E (membrane glycoprotein), M (membrane glycoprotein), ORF8 and N (Nucleocapsid phosphoprotein).
[11] https://www.researchgate.net/profile/Helene_Banoun Evolution of SARS-CoV-2: Review of mutations, role of the host immune system, octobre 2020, mise à jour par Hélène Banoun,
PhD, Pharmacien biologiste, ancien Chargé de Recherches INSERM, ancien Interne des Hôpitaux de Paris.
[12] https://nextstrain.org/, We are incorporating SARS-CoV-2 genomes as soon as they are shared and providing analyses and situation reports. In addition we have developed a number of resources and tools, and are facilitating independent groups to run their own analysis. Please see the main SARS-CoV-2 page for more.
[13] Tutoriel prélèvement nasopharyngé : Un geste technique, essentiel à la fiabilité du test COVID-19
[14] Covid-19 : comment fonctionnent les tests et quelles sont leurs utilités ?
[15] COMMENT FONCTIONNENT LES TESTS DE DÉPISTAGE DU COVID-19 ? 7 avril 2020, Laboratoire de biologie et pharmacologie appliquée (LBPA), Clémence Richetta, maître de conférences au département biologie de l’ENS Paris-Saclay et chercheuse en virologie au LBPA : https://www.youtube.com/watch?v=hNVDHCf8bGA
Independent researcher, PhD 9
Former research fellow at INSERM (French Institute for Health and Medical Research)
[16] Par Pierre Sonigo, virologiste (un des découvreurs du VIH), MD PhD, CSO at Sebia, clinical diagnostics
Diagnostic du COVID19 : comprendre les tests PCR, leur interprétation et leurs limites, publié le 16 septembre 2020
La PCR utilise un principe très particulier : la cible du test, un fragment d’ARN viral, est massivement amplifiée afin de permettre sa détection. Au cours de l’analyse, une réaction enzymatique associée à des « cycles » de variation de température permet une série de « réplications » successives de l’acide nucléique cible. Chaque cycle correspond à une multiplication théorique de la cible par 2. On multiplie donc par 2 en un cycle, par 4 en 2 cycles, par 8 en 3 cycles, par 16 en 4 cycles, et ainsi de suite de manière exponentielle. A l’heure actuelle, l’amplification est généralement pratiquée sur 40 cycles, soit une amplification théorique de 2^40, environ mille milliards de fois ! En réalité, la réplication n’est pas efficace à 100%, mais la cible est amplifiée environ un million de fois, ce qui permet de détecter moins d’une dizaine de fragments d’ARN dans le volume analysé.
Lorsque l’acide nucléique viral est détectable après un petit nombre de cycles, cela signifie que la quantité de virus dans l’échantillon de départ est grande. Au contraire, lorsqu’il faut un grand nombre de cycles de réplication pour détecter l’ARN viral, cela signifie que l’échantillon de départ contient une quantité de virus très faible. On parle alors en nombre de cycles, ou Ct, qui signifie « cycle time », pour définir, au moins de façon semi quantitative, la quantité d’ARN présent dans l’échantillon de départ. Ainsi, un petit Ct correspond à un grand nombre de copies, un grand Ct à un petit nombre de copies.
Cette spectaculaire sensibilité n’est pas sans inconvénient et nécessite des précautions particulières. En effet, un échantillon positif amplifié un million de fois contient une très haute concentration de cible et le risque qu’il contamine (carry over) d’autres échantillons est particulièrement élevé. La saturation des laboratoires peut encore accroître ce risque et générer des faux positifs accidentels. Dans ces conditions, il est important que les résultats positifs soient confirmés par un second test, à plus forte raison lorsqu’un test positif présente des conséquences significatives, qu’elles soient médicales, professionnelles ou liées à l’obligation d’isolement.
La deuxième question importante concernant la PCR, une fois encore conséquence de sa spectaculaire sensibilité, est celle de sa signification clinique. Un sujet parfaitement asymptomatique présentant une PCR positive ne peut être qualifié de « malade », comme on le lit dans les médias qui rapportent la progression de l’épidémie ! Peut-on même parler de « cas » ? C’est pourtant le terme utilisé dans les dénombrements officiels. Ne sommes-nous pas en train d’oublier le patient pour se focaliser sur la technologie ? Est-ce une épidémie d’ARN dans des tubes que nous surveillons ou une maladie grave et potentiellement mortelle ?
Des publications récentes soulignent que la dose détectable par PCR est inférieure à la dose infectieuse ou contagieuse : aucun virus infectieux n’a pu être retrouvé chez les patients asymptomatiques présentant des tests PCR positifs avec un Ct élevé. Suite à ces résultats, la question du seuil de Ct qui permet de déclarer un échantillon positif est débattue. Peut-on rendre un résultat négatif chez un sujet asymptomatique dont la positivité apparaît au-delà de 35 cycles ? A défaut, est-il utile de retester ces échantillons ? Comme souvent en matière de diagnostic médical, lorsqu’un seuil de positivité est déterminé, faut-il privilégier la sensibilité ou la spécificité du test ?
De plus, un échantillon confirmé positif d’un point de vue analytique reste un faux positif du point de vue de la clinique, si la personne testée est en parfaite santé, parfois même prêt à affronter une compétition de tennis ou de football professionnels ! La question devient uniquement celle de sa potentielle contagiosité. C’est la question de la transmission éventuelle par des sujets asymptomatiques, qui sans être eux-mêmes en danger, pourraient en représenter un pour les autres.
Par rapport à cette question, il est important de raisonner quantitativement. La virologie, ce n’est pas du tout ou rien. De manière générale, au cours des infections virales aiguës, le risque de contagion et la gravité de l’infection varient en fonction de la quantité de virus présents dans l’organisme et de leur excrétion dans le milieu extérieur. Quelques copies de virus tapis dans les sinus n’ont pas la dangerosité d’un million projetés par la toux. Un sujet asymptomatique produit moins de virus qu’un sujet symptomatique et les sécrète moins vers l’extérieur. La quantité de virus produite et donc le risque de contagion sont corrélés à la gravité des symptômes. Même si elle n’est pas de zéro, le risque de transmission est donc vraisemblablement faible pour un sujet asymptomatique. Malheureusement, répéter sans cesse que la contagion venant d’un sujet parfaitement asymptomatique est possible sans aucune précision sur le niveau de risque pousse à prendre des mesures disproportionnées avec le risque.
De même, la stratégie « dépister-isoler » n’est pas réaliste lorsque le dépistage n’est pas suffisamment fiable et surtout lorsque le virus est déjà largement répandu dans la population. Il est bien trop tard pour appliquer une méthode conçue pour bloquer une épidémie à sa naissance. Comme pour une invasion de coccinelles ou de frelons, on ne peut stopper un virus qui est déjà partout avec une passoire trouée à 25% et bouchée par endroits. L’échec de la stratégie actuelle est plutôt lié à sa conception naïve et inapplicable qu’aux mauvais comportements des citoyens.
Si, comme on l’observe en ce moment, la diffusion virale reprend, faut-il dépister plus massivement ou revoir la stratégie de protection de la population ?
Cette question ne relève pas de la science. Elle dépend des risques acceptables par un individu ou par un groupe. Si on est dans la recherche du risque minimal, proche de zéro, parce que le risque n’a pas été quantifié, ou pour des raisons de responsabilité juridique, on doit prendre les précautions maximales. Si on accepte un risque même faible, on peut reprendre certaines libertés et protéger ceux qui en ont réellement besoin.
Le scientifique doit mesurer la grandeur des risques et ne pas se contenter d’affirmer qu’un événement adverse est « possible ». Mais ce n’est pas son rôle de décider si ces risques peuvent être pris par autrui.
Les tests PCR permettent une détection extrêmement sensible de l’ARN viral. Ils sont indispensables mais ne sont pas la solution ultime et unique qui permettra de contrôler l’épidémie et de gérer efficacement les risques de contagion. Appliquée lorsque le virus est largement disséminé dans la population, la stratégie « dépister isoler » est vouée à l’échec. Du fait de la sensibilité très élevée et des limites de leur spécificité, les tests PCR doivent être pratiqués et interprétés avec précaution, et comme toujours en lien avec le contexte clinique et épidémiologique. N’oublions pas qu’un sujet asymptomatique doit plutôt être considéré comme immunisé que comme malade.
[17] Les tests RT-PCR du Covid-19 se révèlent être de très mauvais tests de contagiosité, Xavier Boisinet, mis à jour le 3/9/2020.
[19] Mise au point du CNR sur la réalisation des prélèvements et la sensibilité des tests RT-PCR pour la détection du SARS-CoV-2, 9 mai 2020
[20] Avis du 25 septembre 2020 de la Société Française de Microbiologie (SFM) relatif à l’interprétation de la valeur de Ct (estimation de la charge virale) obtenue en cas de RT-PCR SARS-CoV-2 positive sur les prélèvements cliniques réalisés à des fins diagnostiques ou de dépistage, 25 septembre 2020
[21] Coronavirus – Les tests PCR inadaptés contre l’épidémie? « Jusqu’à 90% de personnes testées ne seraient pas contagieuses », basé sur une étude d’une équipe de Harvard ( Harvard TH Chan School of Public Health) de Michael Mina, département d’épidémiologie, je vous mets en fichier joint le PDF correspondant, une étude, reprise par le NY Times :
« Pour eux, la limite du test PCR (prélèvement par voie nasale ou salivaire) réside dans la brutalité et la simplicité du résultat qu’il donne. La personne est soit positive, soit négative. Pas plus de renseignement, notamment sur la contagiosité du malade.
Or, les scientifiques d’Harvard soulèvent le problème de la quantité de virus que ce test PCR ne donne pas et qui pourrait, selon eux, permettre de donner des clés supplémentaires pour contrer l’épidémie.
« Les tests standards diagnostiquent un grand nombre de personnes qui peuvent être porteuses de quantités relativement insignifiantes du virus », explique ainsi le Dr. Michael Mina, épidémiologiste à la Harvard TH Chan School of Public Health. »
[22] « Au rythme actuel avec nos tests RT-PCR, nous allons confiner des dizaines de milliers de gens pour rien », alerte le Dr. Yvon Le Flohic, manuel Moragues, 3 septembre 2020.
[23] Tests de diagnostic ultra sensibles, les tests RT-PCR sortent positifs même pour des individus qui portent trop peu de virus pour être encore contagieux. Pour en faire de meilleurs tests de contagiosité, certains appellent à baisser leur seuil de détection. Est-ce une bonne idée ? Quelles sont les limites de cette solution ? Décryptage.Xavier Boinivet, 15 septembre 2020
[24] Jean-Luc Gala (UCL) estime que les futures mesures de la Celeval, tel le lockdown, vont tuer l’économie, provoquer des suicides et déstabiliser l’État. Le Celeval, ou Cellule d’évaluation, est le groupe d’experts qui conseillent le gouvernement belge dans la gestion du COVID.
[25] L’OMS plaide pour éviter à tout prix les confinements : ‘Cela ne rend que les pauvres plus pauvres’
[26] Voici comment la pandémie risque de faire exploser la pauvreté mondiale, une première en 22 ans
[27] ‘Le coronavirus menace 500 millions de personnes de pauvreté’, prévient l’Oxfam. Ce n’est pas le coronavirus, la menace, mais l’attitude de nos gouvernants face au coronavirus !
[28] Le chômage de masse est désormais mondial
[29] ‘Nous risquons une crise alimentaire imminente si des mesures ne sont pas prises rapidement’. Encore une fois, ce n’est pas à cause du coronavirus, mais à cause de notre attitude face à cette crise.
No comments:
Post a Comment