50 Reasons to Oppose Fluoridation
By Paul Connett, PhD (updated in September 2012)
· A A A
Introduction
Dr.
Paul Connett
In
Europe,
only Ireland (73%), Poland (1%), Serbia (3%), Spain (11%), and the U.K.
(11%) fluoridate any of their water. Most developed countries, including
Japan and 97% of the western European population, do not consume fluoridated
water.
In
the U.S., about 70% of public water supplies are fluoridated. This equates to
approximately 185 million people, which is over half the number
of people drinking artificially fluoridated water worldwide. Some countries
have areas with high natural fluoride levels in the water. These include India,
China and parts of Africa. In these countries measures are being taken to remove
the fluoride because of the health problems that fluoride can cause.
Fluoridation is a bad medical practice
1) Fluoride is the only chemical
added to water for the purpose of medical treatment. The U.S. Food and Drug
Administration (FDA) classifies fluoride as a drug when
used to prevent or mitigate disease (FDA 2000). As a matter of basic logic,
adding fluoride to water for the sole purpose of preventing tooth decay (a
non-waterborne disease) is a form of medical treatment. All other water
treatment chemicals are added to improve the water’s quality or safety, which
fluoride does not do.
2) Fluoridation is unethical. Informed
consent is standard practice for all medication, and one of the key reasons
why most of Western Europe has ruled against fluoridation. With water
fluoridation we are allowing governments to do to whole communities (forcing
people to take a medicine irrespective of their consent) what individual
doctors cannot do to individual patients.
Put
another way: Does a voter have the right to require that their neighbor ingest
a certain medication (even if it is against that neighbor’s will)?
3) The dose cannot be controlled. Once fluoride is put in the water
it is impossible to control the dose each individual receives because people
drink different amounts of water. Being able to control the dose a patient
receives is critical. Some people (e.g., manual laborers, athletes, diabetics,
and people with kidney disease) drink substantially more water than others.
4) The fluoride goes to everyone
regardless of age, health or vulnerability. According to Dr. Arvid Carlsson, the
2000 Nobel Laureate in Medicine and Physiology and one of the scientists who
helped keep fluoridation out of Sweden:
“Water
fluoridation goes against leading principles of pharmacotherapy, which is
progressing from a stereotyped medication — of the type 1 tablet 3 times a day
— to a much more individualized therapy as regards both dosage and selection of
drugs. The addition of drugs to the drinking water means exactly the opposite
of an individualized therapy” (Carlsson 1978).
5) People now receive fluoride from
many other sources besides water. Fluoridated water is not the only way people are
exposed to fluoride. Other
sources of fluoride include food and beverages processed with fluoridated
water (Kiritsy 1996; Heilman 1999), fluoridated dental products (Bentley 1999;
Levy 1999), mechanically deboned meat (Fein 2001), tea (Levy 1999), and
pesticide residues (e.g., from cryolite) on food (Stannard 1991; Burgstahler
1997). It is now widely acknowledged that exposure to non-water sources of
fluoride has significantly increased since the water fluoridation program first
began (NRC 2006).
6) Fluoride is not an essential
nutrient. No
disease, not even tooth decay, is caused by a “fluoride
deficiency.”(NRC 1993; Institute of Medicine 1997, NRC 2006). Not a single
biological process has been shown to require fluoride. On the contrary there is
extensive evidence that fluoride can interfere with many important biological
processes. Fluoride interferes with numerous enzymes (Waldbott 1978). In
combination with aluminum, fluoride interferes with G-proteins (Bigay 1985,
1987). Such interactions give aluminum-fluoride complexes the potential to
interfere with signals from growth factors, hormones and neurotransmitters
(Strunecka & Patocka 1999; Li 2003). More and more studies indicate that
fluoride can interfere with biochemistry
in fundamental ways (Barbier 2010).
7) The level in mothers’ milk is
very low.
Considering reason #6 it is perhaps not surprising that the level of fluoride
in mother’s
milk is remarkably low (0.004 ppm, NRC, 2006). This means that a bottle-fed
baby consuming fluoridated water (0.6 – 1.2 ppm) can get up to 300 times more
fluoride than a breast-fed baby. There are no benefits (see reasons #11-19),
only risks (see reasons #21-36), for infants ingesting this heightened level of
fluoride at such an early age (an age where susceptibility to environmental
toxins is particularly high).
8 ) Fluoride accumulates in the body. Healthy adult kidneys excrete 50
to 60% of the fluoride ingested each day (Marier & Rose 1971). The
remainder accumulates in the body, largely in calcifying tissues such as the
bones and pineal
gland (Luke 1997, 2001). Infants and children excrete less
fluoride from their kidneys and take up to 80% of ingested fluoride into their
bones (Ekstrand 1994). The fluoride concentration in bone steadily increases
over a lifetime (NRC 2006).
9) No health agency in fluoridated
countries is monitoring fluoride exposure or side effects. No regular measurements are being
made of the levels of fluoride in urine, blood, bones, hair, or nails of either
the general population or sensitive subparts of the population (e.g.,
individuals with kidney
disease).
10) There has never been a single
randomized controlled trial to demonstrate fluoridation’s effectiveness or
safety. Despite the
fact that fluoride has been added to community water supplies for over 60
years, “there have been no randomized trials of water fluoridation” (Cheng
2007). Randomized trials
are the standard method for determining the safety and effectiveness of any
purportedly beneficial medical treatment. In 2000, the British Government’s
“York Review” could not give a single fluoridation trial a Grade A
classification – despite 50 years of research (McDonagh 2000). The U.S. Food
and Drug Administration (FDA) continues to classify fluoride as an “unapproved new drug.”
Swallowing fluoride provides no (or very little)
benefit
11) Benefit is topical not systemic. The Centers for Disease
Control and Prevention (CDC, 1999, 2001) has now acknowledged that the mechanism
of fluoride’s benefits are mainly topical,
not systemic. There is no need whatsoever, therefore, to swallow fluoride to
protect teeth. Since the purported benefit of fluoride is topical, and the
risks are systemic, it makes more sense to deliver the fluoride directly to the
tooth in the form of toothpaste. Since swallowing fluoride is unnecessary, and
potentially dangerous, there is no justification for forcing people (against their
will) to ingest fluoride through their water supply.
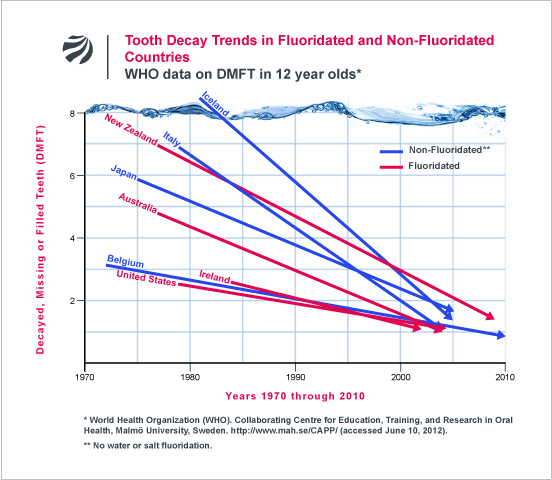
12) Fluoridation is not necessary. Most western, industrialized
countries have rejected
water fluoridation, but have nevertheless experienced the same decline in
childhood dental decay as fluoridated countries. (See data from World Health
Organization presented graphically in Figure).
13) Fluoridation’s role in the
decline of tooth decay is in serious doubt. The largest survey ever
conducted in the US (over 39,000 children from 84 communities) by the National
Institute of Dental Research showed little difference in
tooth decay among children in fluoridated and non-fluoridated communities
(Hileman 1989). According to NIDR researchers, the study found an average
difference of only 0.6 DMFS (Decayed, Missing, and Filled Surfaces) in the
permanent teeth of children aged 5-17 residing their entire lives in either
fluoridated or unfluoridated areas (Brunelle & Carlos, 1990). This
difference is less than one tooth surface, and less than 1% of the 100+ tooth
surfaces available in a child’s mouth. Large surveys from three Australian
states have found even less of a benefit, with decay reductions ranging from 0
to 0.3 of one permanent tooth surface (Spencer 1996; Armfield & Spencer
2004). None of these studies have allowed for the possible delayed eruption of
the teeth that may be caused by exposure to fluoride, for which there is some
evidence (Komarek 2005). A one-year delay in eruption of the permanent teeth
would eliminate the very small benefit recorded in these modern studies.
14) NIH-funded study on individual
fluoride ingestion and tooth decay found no significant correlation. A multi-million dollar, U.S.
National Institutes of Health (NIH)-funded study found no significant
relationship between tooth decay and fluoride intake among
children. (Warren 2009) This is the first time tooth decay has been
investigated as a function of individual exposure (as opposed to mere residence
in a fluoridated community).
15) Tooth decay is high in
low-income communities that have been fluoridated for years. Despite some claims to the
contrary, water fluoridation cannot prevent the oral health crises
that result from rampant poverty, inadequate nutrition, and lack of access to
dental care. There have been numerous reports of severe dental crises in
low-income neighborhoods of US cities that have been fluoridated for over 20
years (e.g., Boston, Cincinnati, New York City, and Pittsburgh). In addition,
research has repeatedly found fluoridation to be ineffective at preventing the
most serious oral health problem facing poor children, namely “baby bottle tooth decay,”
otherwise known as early childhood caries (Barnes 1992; Shiboski 2003).
16) Tooth decay does not go up when
fluoridation is stopped. Where fluoridation has been discontinued in
communities from Canada, the former East Germany, Cuba and Finland, dental
decay has not increased but has generally continued to decrease (Maupomé 2001;
Kunzel & Fischer, 1997, 2000; Kunzel 2000; Seppa 2000).
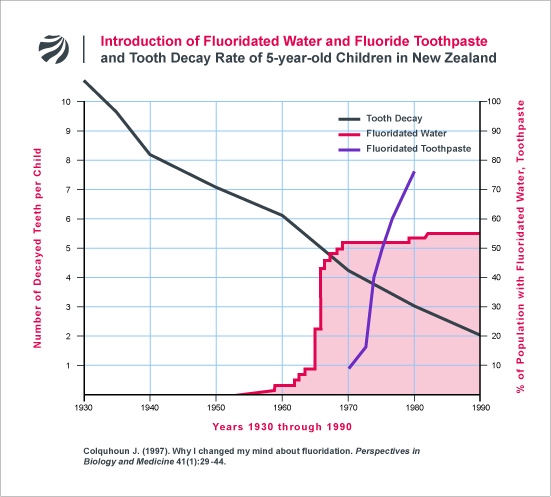
17) Tooth decay was coming down
before fluoridation started. Modern research shows that decay rates were coming down
before fluoridation was introduced in Australia and New Zealand and have
continued to decline even after its benefits would have been maximized.
(Colquhoun 1997; Diesendorf 1986). As the following figure indicates, many
other factors are responsible for the decline of tooth decay that has been
universally reported throughout the western world.
18) The studies that launched
fluoridation were methodologically flawed. The early trials conducted between
1945 and 1955 in North America that helped to launch fluoridation, have been
heavily criticized for their poor methodology and poor choice of control
communities (De Stefano 1954; Sutton 1959, 1960, 1996; Ziegelbecker 1970).
According to Dr. Hubert Arnold, a statistician from the University of
California at Davis, the early fluoridation trials “are especially rich in
fallacies, improper design, invalid use of statistical methods, omissions of
contrary data, and just plain muddleheadedness and hebetude.” Serious questions
have also been raised about Trendley Dean’s (the father of fluoridation) famous
21-city study from 1942 (Ziegelbecker 1981).
Children are being over-exposed to fluoride
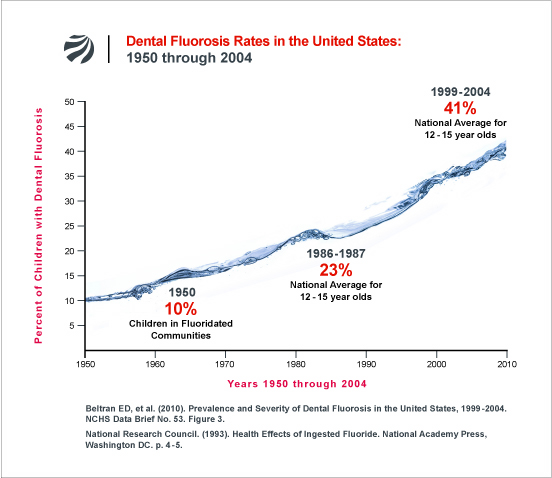
19) Children are being over-exposed
to fluoride. The
fluoridation program has massively failed to achieve one of its key objectives,
i.e., to lower dental decay rates while limiting the occurrence of dental fluorosis (a
discoloring of tooth enamel caused by too much fluoride. The goal of the early
promoters of fluoridation was to limit dental fluorosis (in its very mild form)
to10% of children (NRC 1993, pp. 6-7). In 2010, however, the
Centers for Disease Control and Prevention (CDC) reported that 41% of
American adolescents had dental fluorosis, with 8.6% having mild fluorosis and
3.6% having either moderate or severe dental fluorosis (Beltran-Aguilar 2010).
As the 41% prevalence figure is a national average and includes children living
in fluoridated and unfluoridated areas, the fluorosis rate in fluoridated
communities will obviously be higher. The British Government’s York Review
estimated that up to 48% of children in fluoridated areas worldwide have dental
fluorosis in all forms, with 12.5% having fluorosis of aesthetic
concern (McDonagh, 2000).
20) The highest doses of fluoride
are going to bottle-fed babies. Because of their sole reliance on liquids for their
food intake, infants
consuming formula made with fluoridated water have the highest exposure to
fluoride, by bodyweight, in the population. Because infant exposure to
fluoridated water has been repeatedly found to be a major risk factor for
developing dental fluorosis later in life (Marshall 2004; Hong 2006; Levy
2010), a number of dental
researchers have recommended that parents of newborns not use fluoridated
water when reconstituting formula (Ekstrand 1996; Pendrys 1998; Fomon 2000;
Brothwell 2003; Marshall 2004). Even the American Dental Association (ADA), the
most ardent institutional proponent of fluoridation, distributed a November 6,
2006 email alert to its members recommending that parents be advised that
formula should be made with “low or no-fluoride water.” Unfortunately, the ADA
has done little to get this information into the hands of parents. As a result,
many parents remain unaware of the fluorosis risk from infant exposure to
fluoridated water.
Evidence of harm to other tissues
21) Dental fluorosis may be an
indicator of wider systemic damage. There have been many suggestions as to the possible biochemical
mechanisms underlying the development of dental fluorosis (Matsuo 1998; Den
Besten 1999; Sharma 2008; Duan 2011; Tye 2011) and they are complicated for a
lay reader. While promoters of fluoridation are content to dismiss dental
fluorosis (in its milder forms) as merely a cosmetic effect, it is rash to
assume that fluoride is not impacting other developing tissues when it is
visibly damaging the teeth by some biochemical mechanism (Groth 1973; Colquhoun
1997). Moreover, ingested fluoride can only cause dental fluorosis during the
period before the permanent teeth have erupted (6-8 years), other tissues are
potentially susceptible to damage throughout life. For example, in areas of
naturally high levels of fluoride the first indicator of harm is dental
fluorosis in children. In the same communities many older people develop skeletal
fluorosis.
22) Fluoride may damage the brain. According to the National Research
Council (2006), “it is apparent that fluorides have the ability to interfere
with the functions of the brain.” In a review of
the literature commissioned by the US Environmental Protection Agency (EPA),
fluoride has been listed among about 100 chemicals for which there is
“substantial evidence of developmental neurotoxicity.” Animal experiments
show that fluoride accumulates in the brain and alters mental behavior in a
manner consistent with a neurotoxic agent (Mullenix 1995). In total, there have
now been over 100 animal
experiments showing that fluoride can damage the brain and
impact learning and behavior. According to fluoridation proponents, these
animal studies can be ignored because high doses were used. However, it is
important to note that rats generally require five times more fluoride to reach
the same plasma levels in humans (Sawan 2010). Further, one animal experiment
found effects at remarkably low doses (Varner 1998). In this study, rats fed
for one year with 1 ppm fluoride in their water (the same level used in
fluoridation programs), using either sodium fluoride or aluminum fluoride, had
morphological changes to their kidneys and brains, an increased uptake of
aluminum in the brain, and the formation of beta-amyloid deposits which are
associated with Alzheimer’s disease. Other animal studies have found effects on
the brain at water fluoride levels as low as 5 ppm (Liu 2010).
23) Fluoride may lower IQ. There have now been 33 studies from
China, Iran, India and Mexico that have reported an association between
fluoride exposure and reduced IQ. One of these studies (Lin 1991) indicates
that even just moderate levels of fluoride exposure (e.g., 0.9 ppm in the
water) can exacerbate the neurological defects of iodine deficiency. Other
studies have found IQ reductions at 1.9 ppm (Xiang 2003a,b); 0.3-3.0 ppm (Ding
2011); 1.8-3.9 ppm (Xu 1994); 2.0 ppm (Yao 1996, 1997); 2.1-3.2 ppm (An 1992);
2.38 ppm (Poureslami 2011); 2.45 ppm (Eswar 2011); 2.5 ppm (Seraj 2006); 2.85
ppm (Hong 2001); 2.97 ppm (Wang 2001, Yang 1994); 3.15 ppm (Lu 2000); 4.12 ppm
(Zhao 1996). In the Ding study, each 1 ppm increase of fluoride in urine
was associated with a loss of 0.59 IQ points. None of these studies indicate an
adequate margin of safety to protect all children drinking artificially
fluoridated water from this affect. According to the National Research Council
(2006), “the consistency of the results [in fluoride/IQ studies] appears
significant enough to warrant additional research on the effects of fluoride on
intelligence.” The NRC’s conclusion has recently been amplified by a team of
Harvard scientists whose fluoride/IQ meta-review concludes that fluoride’s
impact on the developing brain should be a “high research priority.” (Choi et
al., 2012). Except for one small IQ study from New Zealand (Spittle 1998) no
fluoridating country has yet investigated the matter.
24) Fluoride may cause non-IQ
neurotoxic effects. Reduced IQ is not the only neurotoxic effect that may result from
fluoride exposure. At least three human studies have reported an association
between fluoride exposure and impaired
visual-spatial organization (Calderon 2000; Li 2004; Rocha-Amador 2009); while
four other studies have found an association between prenatal fluoride exposure
and fetal brain damage
(Han 1989; Du 1992; Dong 1993; Yu 1996).
25) Fluoride affects the pineal
gland. Studies
by Jennifer Luke (2001) show that fluoride accumulates in the human pineal gland to
very high levels. In her Ph.D. thesis, Luke has also shown in animal studies
that fluoride reduces melatonin production and leads to an earlier onset of
puberty (Luke 1997). Consistent with Luke’s findings, one of the earliest
fluoridation trials in the U.S. (Schlesinger 1956) reported that on average
young girls in the fluoridated community reached menstruation 5 months earlier
than girls in the non-fluoridated community. Inexplicably, no fluoridating
country has attempted to reproduce either Luke’s or Schlesinger’s findings or
examine the issue any further.
26) Fluoride affects thyroid
function. According
to the U.S. National Research Council (2006), “several lines of information
indicate an effect of fluoride exposure on thyroid function.”
In the Ukraine, Bachinskii (1985) found a lowering of thyroid function, among
otherwise healthy people, at 2.3 ppm fluoride in water. In the middle of the
20th century, fluoride was prescribed by a number of European doctors to reduce
the activity of the thyroid gland for those suffering from hyperthyroidism
(overactive thyroid) (Stecher 1960; Waldbott 1978). According to a clinical
study by Galletti and Joyet (1958), the thyroid function of hyperthyroid
patients was effectively reduced at just 2.3 to 4.5 mg/day of fluoride ion. To
put this finding in perspective, the Department of Health and Human Services
(DHHS, 1991) has estimated that total fluoride exposure in fluoridated
communities ranges from 1.6 to 6.6 mg/day. This is a remarkable fact,
particularly considering the rampant and increasing problem of hypothyroidism
(underactive thyroid) in the United States and other fluoridated countries.
Symptoms of hypothyroidism include depression, fatigue, weight gain, muscle and
joint pains, increased cholesterol levels, and heart disease. In 2010, the
second most prescribed drug of the year was Synthroid (sodium
levothyroxine) which is a hormone replacement drug used to treat an underactive
thyroid.
27) Fluoride causes arthritic
symptoms. Some of
the early symptoms of skeletal fluorosis (a fluoride-induced bone and
joint disease that impacts millions of people in India, China, and Africa),
mimic the symptoms of arthritis
(Singh 1963; Franke 1975; Teotia 1976; Carnow 1981; Czerwinski 1988; DHHS
1991). According to a review on fluoridation published in Chemical &
Engineering News, “Because some of the clinical symptoms mimic arthritis, the
first two clinical phases of skeletal fluorosis could be easily misdiagnosed”
(Hileman 1988). Few, if any, studies have been done to determine the extent of
this misdiagnosis, and whether the high prevalence of arthritis in America (1
in 3 Americans have some form of arthritis – CDC, 2002) and other fluoridated
countries is related to growing fluoride exposure, which is highly plausible.
Even when individuals in the U.S. suffer advanced forms of skeletal fluorosis
(from drinking large amounts of tea), it has taken years of
misdiagnoses before doctors finally correctly diagnosed the condition
as fluorosis.
28) Fluoride damages bone. An early fluoridation trial
(Newburgh-Kingston 1945-55) found a significant two-fold increase in cortical
bone defects among children in the fluoridated community (Schlesinger 1956).
The cortical bone is the outside layer of the bone and is important to protect
against fracture. While this result was not considered important at the time
with respect to bone fractures, it did prompt questions about a possible link
to osteosarcoma (Caffey, 1955; NAS, 1977). In 2001, Alarcon-Herrera and
co-workers reported a linear correlation between the severity of dental fluorosis
and the frequency of bone fractures in both children and adults in a high
fluoride area in Mexico.
29) Fluoride may increase hip
fractures in the elderly. When high doses of fluoride (average 26 mg per day) were used in
trials to treat patients with osteoporosis in an effort to harden their bones
and reduce fracture rates, it actually led to a higher number of fractures,
particularly hip
fractures (Inkovaara 1975; Gerster 1983; Dambacher 1986; O’Duffy 1986;
Hedlund 1989; Bayley 1990; Gutteridge 1990. 2002; Orcel 1990; Riggs 1990 and
Schnitzler 1990). Hip fracture is a very serious issue for the elderly, often
leading to a loss of independence or a shortened life. There have been over a dozen
studies published since 1990 that have investigated a possible relationship
between hip fractures and long term consumption of artificially fluoridated
water or water with high natural levels. The results have been mixed – some have found
an association and others have not. Some have even claimed a protective effect.
One very important study in China, which examined hip fractures in six Chinese
villages, found what appears to be a dose-related increase in hip fracture as
the concentration of fluoride rose from 1 ppm to 8 ppm (Li 2001) offering
little comfort to those who drink a lot of fluoridated water. Moreover, in the
only human epidemiological study to assess bone strength as a function of bone
fluoride concentration, researchers from the University of Toronto found that
(as with animal studies) the strength of bone declined with increasing fluoride
content (Chachra 2010). Finally, a recent study from Iowa
(Levy 2009), published data suggesting that low-level fluoride exposure may
have a detrimental effect on cortical bone density
in girls (an effect that has been repeatedly documented
in clinical trials and which has been posited as an important mechanism by which
fluoride may increase bone fracture rates).
30) People with impaired kidney
function are particularly vulnerable to bone damage. Because of their inability to
effectively excrete fluoride, people with kidney disease
are prone to accumulating high levels of fluoride in their bone and blood. As a
result of this high fluoride body burden, kidney patients have an elevated risk
for developing skeletal fluorosis. In one of the few U.S. studies investigating
the matter, crippling skeletal fluorosis was documented among patients with
severe kidney disease drinking water with just 1.7 ppm fluoride (Johnson 1979).
Since severe skeletal fluorosis in kidney patients has been detected in small
case studies, it is likely that larger, systematic studies would detect
skeletal fluorosis at even lower fluoride levels.
31) Fluoride may cause bone cancer
(osteosarcoma). A
U.S. government-funded animal study found a dose-dependent increase in bone
cancer (osteosarcoma)
in fluoride-treated, male rats (NTP 1990). Following the results of this study,
the National Cancer Institute (NCI) reviewed national cancer data in the U.S.
and found a significantly higher rate of osteosarcoma (a bone cancer) in young
men in fluoridated versus unfluoridated areas (Hoover et al 1991a). While the
NCI concluded (based on an analysis lacking statistical power) that
fluoridation was not the cause (Hoover et al 1991b), no explanation was
provided to explain the higher rates in the fluoridated areas. A smaller study
from New Jersey (Cohn 1992) found osteosarcoma rates to be up to 6 times higher
in young men living in fluoridated versus unfluoridated areas. Other
epidemiological studies of varying size and quality have failed to find this
relationship (a summary of these can be found in Bassin, 2001 and Connett &
Neurath, 2005). There are three reasons why a fluoride-osteosarcoma connection
is plausible: First, fluoride accumulates to a high level in bone. Second, fluoride
stimulates bone growth. And, third, fluoride can interfere with the genetic
apparatus of bone cells in several ways; it has been shown to be mutagenic,
cause chromosome damage, and interfere with the enzymes involved with DNA
repair in both cell and tissue studies (Tsutsui 1984; Caspary 1987; Kishi 1993;
Mihashi 1996; Zhang 2009). In addition to cell and tissue studies, a
correlation between fluoride exposure and chromosome damage in humans has also
been reported (Sheth 1994; Wu 1995; Meng 1997; Joseph 2000).
32) Proponents have failed to refute
the Bassin-Osteosarcoma study. In 2001, Elise Bassin, a dentist, successfully defended her
doctoral thesis at Harvard in which she found that young boys had a
five-to-seven fold increased risk of getting osteosarcoma by the age of 20 if
they drank fluoridated water during their mid-childhood growth spurt (age 6 to
8). The study was published in 2006 (Bassin 2006) but has been largely
discounted by fluoridating countries because her thesis adviser Professor Chester Douglass
(a promoter of fluoridation and a consultant for Colgate) promised a larger
study that he claimed would discount her thesis (Douglass and Joshipura, 2006).
Now, after 5 years of waiting the Douglass study has finally been published
(Kim 2011) but in no way does this study discount Bassin’s findings. The study,
which used far fewer controls than Bassin’s analysis, did not even attempt to
assess the age-specific window of risk that Bassin identified. Indeed, by the
authors’ own admission, the study had no capacity to assess the risk of
osteosarcoma among children and adolescents (the precise population of
concern). For a critique of the Douglass study, click here.
33) Fluoride may cause reproductive
problems. Fluoride
administered to animals at high doses wreaks havoc on the male reproductive
system – it damages sperm and increases the rate of infertility in
a number of different species (Kour 1980; Chinoy 1989; Chinoy 1991; Susheela
1991; Chinoy 1994; Kumar 1994; Narayana 1994a,b; Zhao 1995; Elbetieha 2000;
Ghosh 2002; Zakrzewska 2002). In addition, an epidemiological study from the US
found increased rates of infertility among couples living in areas with 3 ppm
or more fluoride in the water (Freni 1994), two studies have found increased
fertility among men living in high-fluoride areas of China and India (Liu 1988;
Neelam 1987); four studies have found reduced level of circulating testosterone
in males living in high fluoride areas (Hao 2010; Chen P 1997; Susheela 1996;
Barot 1998), and a study of fluoride-exposed workers reported a “subclinical reproductive
effect” (Ortiz-Perez 2003). While animal studies by FDA researchers have failed to find
evidence of reproductive toxicity in fluoride-exposed rats (Sprando 1996, 1997,
1998), the National Research Council (2006) has recommended that, “the
relationship between fluoride and fertility requires additional study.”
34) Some individuals are highly
sensitive to low levels of fluoride as shown by case studies
and double blind studies. In one study, which lasted 13 years, Feltman and
Kosel (1961) showed that about 1% of patients given 1 mg of fluoride each day
developed negative reactions. Many individuals have reported suffering from
symptoms such as fatigue, headaches, rashes and stomach and gastro intestinal
tract problems, which disappear when they avoid fluoride in their water and
diet. (Shea 1967; Waldbott 1978; Moolenburgh 1987) Frequently the symptoms
reappear when they are unwittingly exposed to fluoride again (Spittle, 2008).
No fluoridating government has conducted scientific studies to take this issue
beyond these anecdotal reports. Without the willingness of governments to
investigate these reports scientifically, should we as a society be forcing
these people to ingest fluoride?
35) Other subsets of population are
more vulnerable to fluoride’s toxicity. In addition to people suffering from impaired kidney
function discussed in reason #30 other subsets of the population are more
vulnerable to fluoride’s toxic effects. According to the Agency for Toxic
Substances and Disease Registry (ATSDR 1993) these include: infants, the
elderly, and those with diabetes mellitus. Also
vulnerable are those who suffer from malnutrition (e.g.,
calcium, magnesium, vitamin C, vitamin D and iodine deficiencies and
protein-poor diets) and those who have diabetes
insipidus. See: Greenberg 1974; Klein 1975; Massler & Schour 1952;
Marier & Rose 1977; Lin 1991; Chen 1997; Seow 1994; Teotia 1998.
No Margin of Safety
36) There is no margin of safety for
several health effects. No one can deny that high natural levels of fluoride damage health.
Millions of people in India and China have had their health compromised by fluoride.
The real question is whether there is an adequate margin of safety between the
doses shown to cause harm in published studies and the total dose people
receive consuming uncontrolled amounts of fluoridated water and non-water
sources of fluoride. This margin of safety has to take into account the wide
range of individual sensitivity expected in a large population (a safety factor
of 10 is usually applied to the lowest level causing harm). Another safety
factor is also needed to take into account the wide range of doses to which
people are exposed. There is clearly no margin of safety for dental fluorosis
(CDC, 2010) and based on the following studies nowhere near an adequate margin
of safety for lowered IQ (Xiang 2003a,b; Ding 2011; Choi 2012); lowered thyroid
function (Galletti & Joyet 1958; Bachinskii 1985; Lin 1991); bone fractures
in children (Alarcon-Herrera 2001) or hip fractures in the elderly (Kurttio
1999; Li 2001). All of these harmful effects are discussed in the NRC (2006)
review.
Environmental Justice
37) Low-income families penalized by
fluoridation. Those
most likely to suffer from poor nutrition, and thus more likely to be more
vulnerable to fluoride’s toxic effects, are the poor, who unfortunately, are
the very people being targeted
by new fluoridation programs. While at heightened risk, poor families are least
able to afford avoiding fluoride once it is added to the water supply. No
financial support is being offered to these families to help them get
alternative water supplies or to help pay the costs of treating unsightly cases
of dental fluorosis.
38) Black and Hispanic children are
more vulnerable to fluoride’s toxicity. According to the CDC’s national survey of dental
fluorosis, black and Mexican-American children have significantly higher rates
of dental fluorosis than white children (Beltran-Aguilar 2005, Table 23). The
recognition that minority children appear to be more vulnerable to toxic
effects of fluoride, combined with the fact that low-income families are less
able to avoid drinking fluoridated water, has prompted prominent leaders in the
environmental-justice movement to oppose mandatory fluoridation in Georgia. In
a statement issued in May 2011, Andrew Young, a colleague of Martin Luther
King, Jr., and former Mayor of Atlanta and former US Ambassador to the United
Nations, stated:
“I
am most deeply concerned for poor families who have babies: if they cannot
afford unfluoridated water for their babies’ milk formula, do their babies not
count? Of course they do. This is an issue of fairness, civil rights, and
compassion. We must find better ways to prevent cavities, such as helping those
most at risk for cavities obtain access to the services of a dentist…My father
was a dentist. I formerly was a strong believer in the benefits of water
fluoridation for preventing cavities. But many things that we began to do 50 or
more years ago we now no longer do, because we have learned further information
that changes our practices and policies. So it is with fluoridation.”
39) Minorities are not being warned
about their vulnerabilities to fluoride. The CDC is not warning black and Mexican-American
children that they have higher rates of dental fluorosis than Caucasian
children (see #38). This extra
vulnerability may extend to other toxic effects of fluoride. Black
Americans have higher rates of lactose intolerance, kidney problems and
diabetes, all of which may exacerbate fluoride’s toxicity.
40) Tooth decay reflects low-income
not low-fluoride intake. Since dental decay is most concentrated in poor communities, we should
be spending our efforts trying to increase the access to dental care for
low-income families. The highest rates of tooth decay today can be found in
low-income areas that have been fluoridated for many years. The real “Oral
Health Crisis” that exists today in the United States, is not a lack of
fluoride but poverty and lack of dental insurance. The Surgeon General has
estimated that 80% of dentists in the US do not treat children on Medicaid.
The largely untested chemicals used in fluoridation
programs
41) The chemicals used to fluoridate
water are not pharmaceutical grade. Instead, they largely come from the wet scrubbing
systems of the phosphate
fertilizer industry. These chemicals (90% of which are sodium
fluorosilicate and fluorosilicic acid), are classified hazardous wastes
contaminated with various impurities. Recent testing by the National Sanitation
Foundation suggest that the levels of arsenic in these silicon fluorides are
relatively high (up to 1.6 ppb after dilution into public water) and of
potential concern (NSF 2000 and Wang 2000). Arsenic is a known human carcinogen
for which there is no safe level. This one contaminant alone could be
increasing cancer rates – and unnecessarily so.
42) The silicon fluorides have not
been tested comprehensively. The chemical usually tested in animal studies is
pharmaceutical grade sodium fluoride, not industrial grade fluorosilicic acid.
Proponents claim that once the silicon fluorides have been diluted at the
public water works they are completely dissociated to free fluoride ions and
hydrated silica and thus there is no need to examine the toxicology of these
compounds. However, while a study from the University of Michigan (Finney et
al., 2006) showed complete dissociation at neutral pH, in acidic conditions (pH
3) there was a stable complex containing five fluoride ions. Thus the
possibility arises that such a complex may be regenerated in the stomach where
the pH lies between 1 and 2.
43) The silicon fluorides may
increase lead uptake into children’s blood. Studies by Masters and Coplan (1999,
2000, 2007), and to a lesser extent Macek (2006), show an association between
the use of fluorosilicic acid (and its sodium salt) to fluoridate water and an
increased uptake of lead into children’s blood. Because of lead’s acknowledged
ability to damage the developing brain, this is a very serious finding.
Nevertheless, it is being largely ignored by fluoridating countries. This
association received some strong biochemical support from an animal study by
Sawan et al. (2010) who found that exposure of rats to a combination of
fluorosilicic acid and lead in their drinking water increased the uptake of lead
into blood some threefold over exposure to lead alone.
44) Fluoride may leach lead from
pipes, brass fittings and soldered joints. In tightly controlled laboratory experiments,
Maas et al (2007) have shown that fluoridating agents in combination with chlorinating
agents such as chloroamine increase the leaching of lead from brass fittings
used in plumbing. While proponents may argue about the neurotoxic effects of
low levels of fluoride there is no argument that lead at very low levels lowers
IQ in children.
Continued promotion of fluoridation is unscientific
45) Key health studies have not been
done. In the
January 2008 issue of Scientific American, Professor John Doull, the chairman
of the important 2006 National
Research Council review, Fluoride in Drinking Water: A Review of EPA’s
Standards, is quoted as saying:
What
the committee found is that we’ve gone with the status quo regarding fluoride
for many years—for too long really—and now we need to take a fresh look . . .
In the scientific community people tend to think this is settled. I mean, when
the U.S. surgeon general comes out and says this is one of the top 10 greatest
achievements of the 20th century, that’s a hard hurdle to get over. But when we
looked at the studies that have been done, we found that many of these
questions are unsettled and we have much less information than we should,
considering how long this [fluoridation] has been going on.
The
absence of studies is being used by promoters as meaning the absence of harm.
This is an irresponsible position.
46) Endorsements do not represent
scientific evidence. Many
of those promoting fluoridation rely heavily on a list of endorsements.
However, the U.S. PHS first endorsed fluoridation in 1950, before one single
trial had been completed and before any significant health studies had been
published (see chapters 9 and 10 in The
Case Against Fluoride for the significance of this PHS endorsement for
the future promotion of fluoridation). Many other endorsements swiftly followed
with little evidence of any scientific rational for doing so. The continued use
of these endorsements has more to do with political science than medical
science.
47) Review panels hand-picked to
deliver a pro-fluoridation result. Every so often, particularly when their fluoridation
program is under threat, governments of fluoridating countries hand-pick panels
to deliver reports that provide the necessary re-endorsement of the
practice. In their recent book Fluoride Wars (2009), which is otherwise
slanted toward fluoridation, Alan Freeze and Jay Lehr concede this point when
they write:
There
is one anti-fluoridationist charge that does have some truth to it.
Anti-fluoride forces have always claimed that the many government-sponsored
review panels set up over the years to assess the costs and benefits of
fluoridation were stacked in favor of fluoridation. A review of the membership
of the various panels confirms this charge. The expert committees that put
together reports by the American Association for the Advancement of Science in
1941, 1944 and 1954; the National Academy of Sciences in 1951, 1971, 1977 and
1993; the World Health Organization in 1958 and 1970; and the U.S. Public
Health Service in 1991 are rife with the names of well-known medical and dental
researchers who actively campaigned on behalf of fluoridation or whose research
was held in high regard in the pro-fluoridation movement. Membership was
interlocking and incestuous.
The
most recent examples of these self-fulfilling prophecies have come from the
Irish Fluoridation Forum (2002); the National Health and Medical Research
Council (NHMRC, 2007) and Health Canada (2008, 2010). The latter used a panel
of six experts to review the health literature. Four of the six were
pro-fluoridation dentists and the other two had no demonstrated expertise on
fluoride. A notable exception to this trend was the appointment by the U.S.
National Research Council of the first balanced panel of experts ever selected
to look at fluoride’s toxicity in the U.S. This panel of twelve reviewed the US
EPA’s safe drinking water standards for fluoride. After three and half years
the panel concluded in a 507- page report that the safe drinking water standard
was not protective of health and a new maximum contaminant level goal (MCLG)
should be determined (NRC, 2006). If normal toxicological procedures and
appropriate margins of safety were applied to their findings this report should
spell an end to water fluoridation. Unfortunately in January of 2011 the US EPA
Office of Water made it clear that they would not determine a value for the
MCLG that would jeopardize the water fluoridation program (EPA press release,
Jan 7, 2011. Once again politics was allowed to trump science.
More and more independent scientists oppose
fluoridation
48) Many scientists oppose
fluoridation. Proponents
of fluoridation have maintained for many years— despite the fact that the
earliest opponents of fluoridation were biochemists—that the only people
opposed to fluoridation are not bona fide scientists. Today, as more and more
scientists, doctors, dentists and other professionals, read the primary
literature for themselves, rather than relying on self-serving statements from
the ADA and the CDC, they are realizing that they and the general public have
not been diligently informed by their professional bodies on this subject. As
of January 2012, over 4,000 professionals have signed a statement
calling for an end to water fluoridation worldwide. This statement and a list
of signatories can be found on the website of the Fluoride Action
Network. A glimpse of the caliber of those opposing fluoridation can be
gleaned by watching the 28-minute video “Professional
Perspectives on Water fluoridation” which can be viewed online at the same
FAN site.
Proponents’ dubious tactics
49) Proponents usually refuse to
defend fluoridation in open debate. While pro-fluoridation officials continue to promote
fluoridation with undiminished fervor, they usually refuse to defend
the practice in open public debate – even when challenged to do so by
organizations such as the Association for Science in the Public Interest, the
American College of Toxicology, or the U.S. EPA (Bryson 2004). According to Dr.
Michael Easley, a prominent lobbyist for fluoridation in the US, “Debates give
the illusion that a scientific controversy exists when no credible people
support the fluorophobics’ view” (Easley, 1999). In light of proponents’
refusal to debate this issue, Dr. Edward Groth, a Senior Scientist at Consumers
Union, observed that, “the political profluoridation stance has evolved into a
dogmatic, authoritarian, essentially antiscientific posture, one that
discourages open debate of scientific issues” (Martin 1991).
50) Proponents use very dubious
tactics to promote fluoridation. Many scientists, doctors and dentists who have spoken out
publicly on this issue have been subjected to censorship and
intimidation (Martin 1991). Dr. Phyllis
Mullenix was fired from her position as Chair of Toxicology at Forsythe
Dental Center for publishing her findings on fluoride and the brain (Mullenix
1995); and Dr.
William Marcus was fired from the EPA for questioning the government’s
handling of the NTP’s fluoride-cancer study (Bryson 2004). Many dentists and
even doctors tell opponents in private that they are opposed to this practice
but dare not speak out in public because of peer pressure and the fear of
recriminations. Tactics like this would not be necessary if those promoting
fluoridation were on secure scientific and ethical grounds.
Conclusion
When
it comes to controversies surrounding toxic chemicals, vested interests
traditionally do their very best to discount animal studies and quibble with
epidemiological findings. In the past, political pressures have led government
agencies to drag their feet on regulating asbestos, benzene, DDT, PCBs,
tetraethyl lead, tobacco and dioxins. With fluoridation we have had a
sixty-year delay. Unfortunately, because government officials and dental
leaders have put so much of their credibility on the line defending
fluoridation, and because of the huge liabilities waiting in the wings if they
admit that fluoridation has caused an increase in hip fracture, arthritis, bone
cancer, brain disorders or thyroid problems, it will be very difficult for them
to speak honestly and openly about the issue. But they must, not only to
protect millions of people from unnecessary harm, but to protect the notion
that, at its core, public health policy must be based on sound science, not
political expediency. They have a tool with which to do this: it’s called the
Precautionary Principle. Simply put, this says: if in doubt leave it out. This
is what most
European countries have done and their children’s teeth have not suffered,
while their public’s trust has been strengthened.
Just
how much doubt is needed on just one of the health concerns identified above,
to override a benefit, which when quantified in the largest survey ever
conducted in the US, amounts to less than one tooth surface (out of 128) in a
child’s mouth?
While
fluoridation may not be the greatest environmental health threat, it is one of
the easiest to end. It is as easy as turning off a spigot in the public water
works. But to turn off that spigot takes political will and to get that we need
masses more people informed and organized. Please get these 50 reasons to all
your friends and encourage them to get fluoride out of their community and to
help ban this practice worldwide.
Postscript
Further
arguments against fluoridation, can be viewed at http://www.fluoridealert.org and
in the book The Case Against Fluoridation (Chelsea Green, 2010). Arguments for
fluoridation can be found at http://www.ada.org
Publication history of the 50 Reasons
The
50 Reasons were first compiled by Paul Connett and presented in person to the
Irish Fluoridation Forum in October 2000. The document was refined in 2004 and
published in Medical Veritas. In
the introduction to the 2004 version it was explained that after over four
years the Irish authorities had not been able to muster a response to the 50
Reasons, despite agreeing to do so in 2000. Eventually, an anonymous,
incomplete and superficial response was posted on the Irish Department of
Health and Children’s website (see this response and addendum
at:http://www.dohc.ie/other_health_issues/dental_research/. Paul Connett’s
comprehensive response to this response can be accessed
at http://www.fluoridealert.org/50reasons.ireland.pdf. We learned on
August 7, 2011 that this governmental response was prepared by an external
contractor at a cost to the Irish taxpayers’ of over 30,000 Euros.
Since
2004, there have been many major scientific developments including the
publication of the U.S. National Research Council report (NRC, 2006); the
publication of Bassin’s study on Osteosarcoma (Bassin 2006), and many more
studies of fluoride’s interaction with the brain, that necessitated a major
update of the 50 Reasons in August 2011. This update was made with the generous
assistance of James Beck, MD, PhD, Michael Connett, JD, Hardy Limeback,
DDS, PhD, David McRae and Spedding Micklem, D.Phil. Additional
developments in 2012, including FAN’s translation of over
20 Chinese studies on fluoride toxicity and publication of the Harvard
team’s meta-review of fluoride and IQ (Choi 2012), warranted a further update
in August 2012, with the extremely helpful assistance of my son, Michael
Connett.
References
Agency
for Toxic Substances and Disease Registry (ATSDR) (1993). Toxicological Profile for Fluorides,
Hydrogen Fluoride, and Fluorine (F). U.S. Department of Health &
Human Services, Public Health Service. ATSDR/TP-91/17.
Alarcon-Herrera
MT, et al. (2001). Well Water Fluoride, Dental fluorosis, Bone Fractures in the
Guadiana Valley of Mexico. Fluoride.
34(2): 139-149.
Allain
P, et al. (1996). Enhancement of aluminum digestive absorption by fluoride in
rats. Research Communications in Molecular
Pathology and Pharmacology. 91: 225-31.
An
J, et al. (1992). The effects of high fluoride on the level of intelligence of
primary and secondary students. Chinese
Journal of Control of Endemic Diseases 7(2):93-94.
Armfield
JM and Spencer AJ (2004). Consumption of Nonpublic Water: Implications for
Children’s Caries Experience,” Community
Dentistry and Oral Epidemiology. 32(4): 283–96
Arnold
HA. (1980). Letter to Dr. Ernest Newbrun. May 28,
1980. http://www.fluoridealert.org/uc-davis.htm
Awadia
AK, et al. (2002). Caries experience and caries predictors – a study of
Tanzanian children consuming drinking water with different fluoride
concentrations. Clinical Oral
Investigations. (2002) 6:98-103.
Bachinskii
PP, et al. (1985) Action of the body fluorine of healthy persons and
thyroidopathy patients on the function of hypophyseal-thyroid the system. Probl Endokrinol (Mosk) 31: 25-9.
Barbier
O. (2010) Molecular mechanisms of fluoride toxicity. Chemico-Biological Interactions. 188: 319–333.
Barnes
GP, et al. (1992). Ethnicity, location, age, and fluoridation factors in baby
bottle tooth decay and caries prevalence of Head Start children. Public Health Reports. 107:
167-73.
Barot
VV. (1998). Occurrence of endemic fluorosis in human population of North Gujarat,
India: human health risk. Bulletin
of Environmental Contamination and Toxicology. 61: 303-10.
Bassin
EB. (2001). “Association Between Fluoride in Drinking Water During Growth and
Development and the Incidence of Osteosarcoma for Children and Adolescents,”
DMSc thesis, Harvard School of Dental Medicine, Boston, Massachusetts.
Bassin
EB et al. (2006). Age-specific Fluoride Exposure in Drinking Water and
Osteosarcoma (United States). Cancer
Causes and Control. 17 (4): 421–28.
Bayley
TA, et al. (1990). Fluoride-induced fractures: relation to osteogenic
effect. Journal of Bone and Mineral
Research.5(Suppl 1):S217-22.
Beltrán-Aguilar
ED et al. (2010). Prevalence and severity of dental fluorosis in the
United States, 1999-2004. NCHS
DataBrief No. 53. U.S. DHHS, CDC, National Center for Health
Statistics.
Beltrán-Aguilar
ED et al. (2005). Surveillance for dental caries, dental sealants, tooth
retention, endentulism, and enamel fluorosis—United States, 1988- 1994 and
1999-2002. CDC, MMWR,
Surveillance Summaries, August 26, vol. 54, No SS-3, pp. 1-44. See Table 23.
Bentley
EM, et al. (1999). Fluoride ingestion from toothpaste by young children.
British Dental Journal. 186:
460-2.
Bhatnagar
M, et al. (2002). Neurotoxicity of fluoride: neurodegeneration in hippocampus
of female mice. Indian Journalof
Experimental Biology. 40: 546-54.
Bigay
J, et al. (1987). Fluoride complexes of aluminium or beryllium act on
G-proteins as reversibly bound analogues of the gamma phosphate of GTP. EMBO Journal. 6:2907-2913.
Bigay
J, et al. (1985). Fluoroaluminates activate transducin-GDP by mimicking the
gamma-phosphate of GTP in its binding site. FEBS Letters. 191:181-185.
Brothwell
D, Limeback H. (2003). Breastfeeding is protective against dental fluorosis in
a nonfluoridated rural area of Ontario, Canada. Journal of Human Lactation 19: 386-90.
Brunelle
JA, Carlos JP. (1990). Recent trends in dental caries in U.S. children and the
effect of water fluoridation. Journalof
Dental Research. 69(Special edition): 723-727.
Bryson
C. (2004). The Fluoride Deception.
Seven Stories Press, New York.
Burgstahler
AW, et al. (1997). Fluoride in California wines and raisins. Fluoride. 30: 142-146.
Caffey
J. On Fibrous Defects in Cortical Walls: Their Radiological Appearance,
Structure, Prevalence, Natural Course, and Diagnostic Significance in Advances in Pediatrics, ed. S. Z. Levin,
(New York: Interscience, 1955).
Calderon
J et al. (2000). Influence of fluoride exposure on reaction time and
visuospatial organization in children. Epidemiology11(4):S153.
Carlsson
A. (1978). Current problems relating to the pharmacology and toxicology of
fluorides. Journal of the Swedish
Medical Association. 14: 1388-1392.
Carnow
BW, Conibear SA. (1981). Industrial fluorosis. Fluoride. 14: 172-181.
Caspary
WJ, et al (1987). Mutagenic activity of fluorides in mouse lymphoma
cells. Mutation Research. 187:165-80.
Centers
for Disease Control and Prevention (CDC). (2002). Prevalence of Self-Reported
Arthritis or Chronic Joint Symptoms Among Adults — United States, 2001. Mortality and Morbidity Weekly Report. 51:
948-950.
Centers
for Disease Control and Prevention (CDC). (2001). Recommendations for Using
Fluoride to Prevent and Control Dental Caries in the United States. Morbidity and Mortality Weekly Report. 50(RR14):
1-42.
Centers
for Disease Control and Prevention (CDC). (1999). Achievements in Public
Health, 1900-1999: Fluoridation of Drinking Water to Prevent Dental
Caries. Mortality and Morbidity
Weekly Report. 48: 933-940.
Chachra
et al. (2010) The long-term effects of water fluoridation on the human
skeleton. Journal of Dental
Research. 89(11): 1219-1223.
Chen
J, et al. (2003). Selective decreases of nicotinic acetylcholine receptors in
PC12 cells exposed to fluoride. Toxicology. 183:
235-42.
Chen
J, et al. (2002). [Studies on DNA damage and apoptosis in rat brain induced by
fluoride] Zhonghua Yu Fang Yi Xue Za
Zhi. 36 222-224.
Chen
YC, et al. (1997). Nutrition survey in dental fluorosis-afflicted areas. Fluoride. 30(2):77-80.
Chen
P, et al. (1997). Effects of hyperfluoride on reproduction-endocrine system of
male adults. Endemic Diseases
Bulletin 12(2):57-58.
Choi
AL, et al. (2012). Developmental fluoride neurotoxicity: a systematic review
and meta-analysis. Environmental Health
Perspectives doi:10.1289/ehp.1104912
Chinoy
NJ, Narayana MV. (1994). In vitro fluoride toxicity in human spermatozoa. Reproductive Toxicology. 8:155-9.
Chinoy
NJ, et al. (1991). Microdose vasal injection of sodium fluoride in the
rat. Reproductive Toxicology. 5:
505-12.
Chinoy
NJ, Sequeira E. (1989). Effects of fluoride on the histoarchitecture of
reproductive organs of the male mouse.Reproductive
Toxicology. 3: 261-7.
P.
D. Cohn (1992). An Epidemiologic
Report on Drinking Water and Fluoridation, New Jersey Department of Health,
Environmental Health Service, November 8, 1992. Note: The original title of
this report was A Brief Report on
the Association of Drinking Water Fluoridation and the Incidence of
Osteosarcoma Among Young Males. The word “osteosarcoma” was deleted
from the title soon after the report was released.
Colquhoun
J. (1997). Why I changed my mind about Fluoridation. Perspectives in Biology and Medicine 41: 29-44.
Connett
PH, Beck J and Micklem S. The Case
Against Fluoride: How Hazardous Waste Ended Up in Our Drinking Water and the
Powerful Politics and Bad Science That Keep it There. Chelsea Green, White
River Junction, VT, 2010.
Connett,P
(2004) 50 Reasons to Oppose Fluoridation (updated April 12, 2004). Reprinted in
Medical Veritas. 1:70–80.
Medical Veritas. 1:70–80.
Connett
M. (2004). Fluoride & Bone Damage: Published Data. Submission to National
Research Council (NRC).
Connett,
P. (2000). Fluoride: A Statement of Concern. Waste Not #459. January 2000.
Waste Not, 82 Judson Street, Canton, NY 13617.
Connett
P, Neurath C and Connett M. (2005). Revisiting the Fluoride-Osteosarcoma
Connection in the Context of Elise Bassin’s Findings: Part II.” Submission to
the National Research Council of the National Academies review panel on the
Toxicologic Risk of Fluoride in Drinking Water, March 21, 2005 (revised April
8, 2005).
Czerwinski
E, et al. (1988). Bone and joint pathology in fluoride-exposed workers. Archives of Environmental Health. 43:340-343.
Dambacher
MA, et al. (1986). Long-term fluoride therapy of postmenopausal
osteoporosis. Bone 7:
199-205.
De
Liefde B. (1998). The decline of caries in New Zealand over the past 40
Years. New Zealand Dental
Journal. 94: 109-113.
Department
of Health & Human Services. (U.S. DHHS) (1991). Review of Fluoride:
Benefits and Risks. Report of the Ad
Hoc Committee on Fluoride, Committee to Coordinate Environmental
Health and Related Programs. Department of Health and Human Services, USA.
DenBesten,
P (1999). Biological mechanism of dental fluorosis relevant to the use of
fluoride supplements. Community
Dentistry and Oral Epidemiology. 27: 41-7.
De
Stefano TM. (1954). The fluoridation research studies and the general
practitioner. Bulletin of Hudson
County Dental Society.February.
Diesendorf
M.(1986). The mystery of declining tooth decay. Nature. 322: 125-129.
Ding
Y et al. (2010. The relationships between low levels of urine fluoride on
children’s intelligence, dental fluorosis in endemic fluorosis areas in
Hulunbuir, Inner Mongolia, China. Journal
of Hazardous Materials. doi:10.1016/j.jhazmat.2010.12.097.
Ditkoff
BA, Lo Gerfo P. (2000). The Thyroid
Guide. Harper-Collins. New York.
Dong
Z, et al. (1993). Determination of the contents of amino-acid and monoamine
neurotransmitters in fetal brains from a fluorosis-endemic area. Journal of Guiyang Medical College
18(4):241-45.
Douglass
CW and Joshipura K. (2006) “Caution Needed in Fluoride and Osteosarcoma Study”
(letter), Cancer Causes &
Control. 17 (4): 481–82.
Du
L. 1992. The effect of fluorine on the developing human brain. Chinese Journal of Pathology 21(4):218-20
(republished in Fluoride41:327-30).
Duan
X. et al. (2011). Excess Fluoride Interferes with Chloride-channel-dependent
Endocytosis in Ameloblasts. J Dent
Res.90(2):175-180.
Easley,
M. (1999). Community fluoridation in America: the unprincipled opposition.
Dental Watch. http://www.dentalwatch.org/fl/opposition.pdf (accessed
March 21, 2010).
Ekambaram
P, Paul V. (2001). Calcium preventing locomotor behavioral and dental
toxicities of fluoride by decreasing serum fluoride level in rats. Environmental Toxicology and
Pharmacology. 9: 141-146.
Ekstrand
J, et al. (1981). No evidence of transfer of fluoride from plasma to breast
milk. British Medical Journal (Clin
Res Ed). 83: 761-2.
Ekstrand
J, et al. (1994). Fluoride pharmacokinetics in infancy. Pediatric Research. 35:157–163.
Ekstrand
J. (1996). Fluoride Intake. In: Fejerskov O, Ekstrand J, Burt B, Eds. Fluoride in Dentistry, 2nd Edition. Munksgaard,
Denmark. Pages 40-52.
Elbetieha
A, et al. (2000). Fertility effects of sodium fluoride in male mice. Fluoride. 33: 128-134.
Emsley
J, et al (1981). An unexpectedly strong hydrogen bond: ab initio calculations
and spectroscopic studies of amidefluoride systems. Journal of the American Chemical Society. 103: 24-28.
Eswar
P, et al. (2011). Intelligent quotients of 12-14 year old school children in a
high and low fluoride village in India. Fluoride 44:168-72.
Fagin,
D. (2008). Second Thoughts on Fluoride. Scientific American 298 (1)(January): 74–81.
Fein
NJ, Cerklewski FL. (2001). Fluoride content of foods made with mechanically
separated chicken. Journal of
Agricultural Food Chemistry. 49: 4284-6.
Feltman
R, Kosel G. (1961). Prenatal and postnatal ingestion of fluorides – Fourteen
years of investigation – Final report. Journal
of Dental Medicine. 16: 190-99.
Finney
WF et al. (2006) Reexamination of Hexafluorosilicate Hydrolysis by Fluoride NMR
and pH Measurement. Environmental
Science & Technology 40 (8): 2572–77.
Fluoridation
Forum (2002). Forum on Fluoridation (Dublin, Ireland: Stationery Office, 2002).
Fomon
SJ, et al. (2000). Fluoride intake and prevalence of dental fluorosis: trends
in fluoride intake with special attention to infants.Journal of Public Health Dentistry. 60: 131-9.
Franke
J, et al. (1975). Industrial fluorosis. Fluoride. 8: 61-83.
Freni
SC. (1994). Exposure to high fluoride concentrations in drinking water is
associated with decreased birth rates. Journal
of Toxicology and Environmental Health. 42: 109-121.
Freeze
RA and Lehr JA. The Fluoride Wars:
How a Modest Public Health Measure Became America’s Longest-Running Political
Melodrama. (Hoboken, NJ: John Wiley, 2009).
Freni
SC, Gaylor DW. (1992). International trends in the incidence of bone cancer are
not related to drinking water fluoridation.Cancer. 70:
611-8.
Galletti
P, Joyet G. (1958). Effect of fluorine on thyroidal iodine metabolism in
hyperthyroidism. Journal of Clinical
Endocrinology 18: 1102-1110.
Gerster
JC, et al. (1983). Bilateral fractures of femoral neck in patients with
moderate renal failure receiving fluoride for spinal osteoporosis. British Medical Journal (Clin Res
Ed). 287(6394):723-5.
Ghosh
D, et al. (2002). Testicular toxicity in sodium fluoride treated rats:
association with oxidative stress. Reproductive
Toxicolology.16: 385.
Gray,
AS. (1987). Fluoridation: time for a new base line? Journal of the Canadian Dental Association. 53: 763-5.
Greenberg
LW, et al. (1974). Nephrogenic diabetes insipidus with fluorosis. Pediatrics.
54(3):320-2.
Grobleri
SR, et al. (2001). Dental fluorosis and caries experience in relation to three
different drinking water fluoride levels in South Africa. International Journal of Paediatric
Dentistry. 11(5):372-9.
Guan
ZZ, et al (1998). Influence of chronic fluorosis on membrane lipids in rat
brain. Neurotoxicology and
Teratology.20: 537-542.
Gutteridge
DH, et al. (2002). A randomized trial of sodium fluoride (60 mg) +/- estrogen
in postmenopausal osteoporotic vertebral fractures: increased vertebral
fractures and peripheral bone loss with sodium fluoride; concurrent estrogen
prevents peripheral loss, but not vertebral fractures. Osteoporosis International. 13(2):158-70.
Gutteridge
DH, et al. (1990). Spontaneous hip fractures in fluoride-treated patients:
potential causative factors. Journal
of Bone and Mineral Research. 5 Suppl 1:S205-15.
Han
H, Cheng Z, Liu W. 1989. Effects of fluorine on the human fetus. Chinese Journal of Control of Endemic
Diseases 4:136-138 (republished in Fluoride 41:321-6).
Hanmer
R. (1983). Letter from Rebecca Hanmer, deputy assistant administrator for
water, U.S. Environmental Protection Agency, to Leslie A. Russell, D.M.D, March
30, 1983.
Hao
P, et al. (2010). Effect of fluoride on human hypothalamus-hypophysis-testis
axis hormones. Journal of Hygiene
Research 39(1):53-55.
Hazan
S. (2004). Letter from Stan Hazan, General Manager, NSF Drinking Water
Additives Certification Program, to Ken Calvert, Chairman, Subcommittee on
Energy and the Environment, Committee on Science, US House of
Representatives.July 7.
Health
Canada (2008). Findings and
Recommendations of the Fluoride Expert Panel (January 2007). April
2008.
Health
Canada (2010). Guidelines for
Canadian Drinking Water Quality: Guideline Technical Document – Fluoride.
Health Canada Dated Dec 2010, published June 21, 2011.
Hedlund
LR, Gallagher JC. (1989). Increased incidence of hip fracture in osteoporotic
women treated with sodium fluoride. Journal
of Bone and Mineral Research. 4: 223-5.
Heilman
JR et al. (1999). Assessing Fluoride Levels of Carbonated Soft Drinks. Journal of the American Dental
Association. 130 (11): 1593–99.
Heller
KE, et al (1997). Dental caries and dental fluorosis at varying water fluoride
concentrations. Journal of Public
Health Dentistry.57: 136-143.
Hileman
B. (1989). New studies cast doubt on fluoridation benefits. Chemical and Engineering News. May
8.
Hileman
B. (1988). Fluoridation of water: Questions about health risks and benefits
remain after more than 40 years. Chemical
and Engineering News. August 1: 26-42.
Hirzy
JW. (1999). Why the EPA’s Headquarters Union of Scientists Opposes
Fluoridation. Press release from National Treasury Employees Union. May 1.
Hong
F, et al. (2001). Research on the effects of fluoride on child intellectual
development under different environments. Chinese Primary Health Care 15(3):56-57 (republished in Fluoride 2008; 41(2):156–60).
Hong
L, et al. (2006). Timing of fluoride intake in relation to development of
fluorosis on maxillary central
incisors. Community Dentistry and Oral Epidemiology 34:299-309.
incisors. Community Dentistry and Oral Epidemiology 34:299-309.
Hoover
RN, et al. (1991a). Time trends for bone and joint cancers and osteosarcomas in
the Surveillance, Epidemiology and End Results (SEER) Program. National Cancer
Institute In: Review of Fluoride: Benefits and Risks Report of the Ad Hoc
Committee on Fluoride of the Committee to Coordinate Environmental Health and
Related Programs US Public Health Service. Appendix E.
Hoover
RN, et al. (1991b). Time trends for bone and joint cancers and osteosarcomas in
the Surveillance, Epidemiology and End Results (SEER) Program. National Cancer
Institute In: Review of Fluoride: Benefits and Risks Report of the Ad Hoc
Committee on Fluoride of the Committee to Coordinate Environmental Health and
Related Programs US Public Health Service. Appendix F.
Inkovaara
J, et al. (1975). Prophylactic fluoride treatment and aged bones. British Medical Journal. 3: 73-4.
Institute
of Medicine. (1997). Dietary
Reference Intakes for Calcium, Phosphorus, Magnesium, Vitamin D, and Fluoride.
Standing Committee on the Scientific Evaluation of Dietary Reference Intakes,
Food and Nutrition Board. National Academy Press.
Johnson
WJ, et al. (1979). Fluoridation and bone disease in renal patients. In:
Johansen E, Taves DR, Olsen TO, Eds.Continuing Evaluation of the Use of
Fluorides. AAAS Selected Symposium. Westview Press, Boulder, Colorado. pp.
275-293.
Joseph
S, Gadhia PK. (2000). Sister chromatid exchange frequency and chromosome
aberrations in residents of fluoride endemic regions of South Gujarat. Fluoride. 33: 154-158.
Juncos
LI, Donadio JV. (1972). Renal failure and fluorosis. Journal of the American Medical Association 222: 783-5.
Kelly
JV. (2000). Letter to Senator Robert Smith, Chairman of Environment and Public
Works Committee, U.S. Senate, August 14, 2000.
Kilborn
LG, et al. (1950). Fluorosis with report of an advanced case. Canadian Medical Association Journal. 62:
135-141.
Kim
FM et al. (2011). An Assessment of Bone Fluoride and Osteosarcoma. J. Dent.Res. July 28, 2011
(published online).
Kiritsy
MC, et al. (1996). Assessing fluoride concentrations of juices and
juice-flavored drinks. Journal of
the American Dental Association. 127: 895-902.
Kishi
K, Ishida T. (1993). Clastogenic activity of sodium fluoride in great ape
cells. Mutation Research. 301:183-8.
Klein
H. (1975). Dental fluorosis associated with hereditary diabetes insipidus. Oral
Surg Oral Med Oral Pathol. 40(6):736-41.
Komárek
AE (2005). A Bayesian Analysis of Multivariate Doubly-Interval-Censored Dental
Data,” Biostatistics. 6
(1):145–55.
Kour
K, Singh J. (1980). Histological finding of mice testes following fluoride
ingestion. Fluoride. 13:
160-162.
Kumar
A, Susheela AK. (1994). Ultrastructural studies of spermiogenesis in rabbit
exposed to chronic fluoride toxicity. International
Journal of Fertility and Menopausal Studies. 39:164-71.
Kumar
JV, Green EL. (1998). Recommendations for fluoride use in children. NY State Dental Journal. 64: 40-7.
Kunzel
W, Fischer T. (2000). Caries prevalence after cessation of water fluoridation
in La Salud, Cuba. Caries Research.34:
20- 5.
Kunzel
W, et al. (2000). Decline in caries prevalence after the cessation of water
fluoridation in former East Germany. Community
Dentistry and Oral Epidemiology. 28: 382-389.
Kunzel
W, Fischer T. (1997). Rise and fall of caries prevalence in German towns with
different F concentrations in drinking water.Caries Research. 31: 166-73.
Kurttio
PN, et al. (1999). Exposure to natural fluoride in well water and hip fracture:
A cohort analysis in Finland. American
Journal of Epidemiology. 150(8): 817-824.
Lalumandier
JA, et al. (1995). The prevalence and risk factors of fluorosis among patients
in a pediatric dental practice.Pediatric
Dentistry. 17: 19-25.
Levy
SM, Guha-Chowdhury N. (1999). Total fluoride intake and implications for
dietary fluoride supplementation. Journal
of Public Health Dentistry. 59: 211-23.
Levy
SM et al. (2009). Associations of fluoride intake with children’s bone measures
at age 11. Community Dent
OralEpidemiol.37(5):416-26.
Levy
SM, et al. (2010). Associations Between Fluorosis of Permanent Incisors and
Fluoride Intake From Infant Formula, Other Dietary Sources and Dentifrice
During Early Childhood. JADA 141:1190-1201.
Li
J, Yao L, Shao QL, Wu CY. 2004. Effects of high fluoride level on neonatal
neurobehavioural development. Chinese
Journal of Endemiology 23:464-465 (republished in Fluoride 41:165-70).
Li
L. (2003). The biochemistry and physiology of metallic fluoride: action,
mechanism, and implications. Critical
Reviews of Oral Biology and Medicine. 14: 100-14.
Li
XS. (1995). Effect of fluoride exposure on intelligence in children. Fluoride 28: 189-192.
Li
Y, et al. (2001). Effect of long-term exposure to fluoride in drinking water on
risks of bone fractures. Journal of
Bone and Mineral Research 16: 932-9.
Lin
Fa-Fu; et al (1991). The relationship of a low-iodine and high-fluoride
environment to subclinical cretinism in Xinjiang. Endemic Disease Bulletin 6(2):62-67 (republished in Iodine Deficiency Disorder Newsletter Vol.
7(3):24-25).
Liu
H, et al. (1988). Analysis of the effect of fluoride on male infertility in
regions with reported high level of fluoride (endemic fluorosis). Journal of the Medical Institute of Suzhou 8(4):297-99.
Locker
D. (1999). Benefits and Risks of Water Fluoridation. An Update of the 1996
Federal-Provincial Sub-committee Report. Prepared for Ontario Ministry of
Health and Long Term Care.
Long
YG, et al. (2002). Chronic fluoride toxicity decreases the number of nicotinic
acetylcholine receptors in rat brain. Neurotoxicology
and Teratology. 24: 751-7.
Lu
XH, et al. (2000). Study of the mechanism of neurone apoptosis in rats from the
chronic fluorosis. Chinese Journal
of Epidemiology. 19: 96-98.
Lu
Y, et al (2000). Effect of high-fluoride water on intelligence of
children. Fluoride 33:74-78.
Luke
J. (2001). Fluoride deposition in the aged human pineal gland. Caries Research 35: 125-128.
Luke
J. (1997). The Effect of Fluoride on the Physiology of the Pineal Gland. Ph.D.
Thesis. University of Surrey, Guildord.
Maas
RP et al. (2007). Effects of Fluoridation and Disinfection Agent Combinations
on Lead Leaching from Leaded-Brass Parts.Neurotoxicology. 28
(5): 1023–31.
Macek
M, et al. (2006). Blood lead concentrations in children and method of water
fluoridation in the United States, 1988-1994. Environmental Health Perspectives 114:130-134.
Mahaffey
KR, Stone CL. (1976). Effect of High Fluorine (F) Intake on Tissue Lead (Pb)
Concentrations. Federation Proceedings.
35: 256.
Mahoney
MC, et al. (1991). Bone cancer incidence rates in New York State: time
trends and fluoridated drinking water. American
Journal of Public Health. 81: 475-9.
Mann
J, et al. (1990). Fluorosis and dental caries in 6-8-year-old children in a 5
ppm fluoride area. Community
Dentistry and Oral Epidemiology. 18: 77-9.
Mann
J, et al. (1987). Fluorosis and caries prevalence in a community drinking
above-optimal fluoridated water.Community
Dentistry and Oral Epidemiology. 15: 293-5.
Marcus
W. (1990). Memorandum from Dr. William Marcus, to Alan B. Hais, Acting Director
Criteria & Standards Division ODW, US EPA. May 1, 1990.
Marier
J and Rose D. (1977). Environmental
Fluoride. National Research Council of Canada. Associate Committee on
Scientific Criteria for Environmental Quality. NRCC No. 16081, Ottawa, Canada.
Marshall
TA, et al. (2004). Associations between Intakes of Fluoride from Beverages
during Infancy and Dental Fluorosis of Primary Teeth. Journal of the American College of Nutrition 23:108-16.Martin
B. (1991). Scientific Knowledge in
Controversy: The Social Dynamics of the Fluoridation Debate. SUNY
Press,Albany NY.
Martin
B. (1991). Scientific Knowledge in
Controversy: The Social Dynamics of the Fluoridation Debate. SUNY Press,
Albany NY.
Massler
M, Schour I. (1952). Relation of endemic dental fluorosis to
malnutrition. Journal of the
American Dental Association. 44: 156-165.
Masters
R, et al. (2000). Association of silicofluoride treated water with elevated
blood lead. Neurotoxicology. 21:
1091-1099.
Masters
RD, Coplan M. (1999). Water treatment with silicofluorides and lead
toxicity. International Journal of
Environmental Studies.56: 435-449.
Matsuo
S, et al. (1998). Mechanism of toxic action of fluoride in dental fluorosis:
whether trimeric G proteins participate in the disturbance of intracellular
transport of secretory ameloblast exposed to fluoride. Archives of Toxicology. 72: 798-
806.
Maupome
G, et al. (2001). Patterns of dental caries following the cessation of water fluoridation. Community Dentistry and Oral
Epidemiology. 29: 37-47.
McClure
F. (1970). Water fluoridation, the
search and the victory. US Department of Health, Education, and
Welfare, Washington DC.
McDonagh
M, et al. (2000). A Systematic
Review of Public Water Fluoridation. NHS Center for Reviews and
Dissemination, University of York, September 2000.
Meng
Z, Zhang B. (1997). Chromosomal aberrations and micronuclei in lymphocytes of
workers at a phosphate fertilizer factory.Mutation
Research. 393: 283-288.
Mihashi,
M. and Tsutsui,T.(1996). Clastogenic activity of sodium fluoride to rat
vertebral body-derived cells in culture.Mutation
Research 368: 7-13.
Moolenburgh
H. (1987). Fluoride: The Freedom
Fight. Mainstream Publishing, Edinburgh.
Morgan
L, et al. (1998). Investigation of the possible associations between fluorosis,
fluoride exposure, and childhood behavior problems. Pediatric Dentistry. 20: 244-252. Mullenix P, et al. (1995).
Neurotoxicity of sodium fluoride in rats. Neurotoxicology and Teratology. 17: 169-177.
Mullenix
P, et al. (1995). Neurotoxicity of sodium fluoride in rats. Neurotoxicology and Teratology. 17:
169-177.
Narayana
MV, et al. (1994). Reversible effects of sodium fluoride ingestion on
spermatozoa of the rat. International Journal
of Fertility and Menopausal Studies. 39: 337-46.
Narayana
MV, Chinoy NJ. (1994). Effect of fluoride on rat testicular
steroidogenesis. Fluoride. 27:
7-12.
NHMRC
(2007). National Health and Medical Research Council, A Systematic Review of the Efficacy and Safety of Fluoridation,reference no. EH41, Australian Government,
December 27, 2007.
National
Research Council (1977). Drinking
Water and Health, National Academy of Sciences, Washington DC: National
Academy Press, 1977, 388–89. National Research Council. (1993). Health Effects of Ingested Fluoride. National
Academy Press, Washington DC. National Sanitation Foundation International
(NSF). (2000)
National
Research Council. (1993). Health
Effects of Ingested Fluoride. National Academy Press, Washington DC.
National Sanitation Foundation International (NSF). (2000)
National
Toxicology Program [NTP] (1990). Toxicology
and Carcinogenesis Studies of Sodium Fluoride in F344/N Rats and B6C3f1
Mice. Technical report Series No. 393. NIH Publ. No 91-2848. National
Institute of Environmental Health Sciences, Research Triangle Park, N.C. The
results of this study are summarized in the Department of Health and Human
Services report (DHHS,1991).
NRC
(2006). National Research Council of the National Academies, Fluoride in Drinking Water: A Scientific
Review of EPA’s Standards. Washington, DC: National Academies Press.
Neelam,
K, et al. (1987). Incidence of prevalence of infertility among married male
members of endemic fluorosis district of Andhra Pradesh. In: Abstract Proc Conf Int Soc for Fluoride Res.
Nyon, Switzerland.
O’Duffy
JD, et al. (1986). Mechanism of acute lower extremity pain syndrome in
fluoride-treated osteoporotic patients.American
Journal of Medicine. 80: 561-6.
Olsson
B. (1979). Dental findings in high-fluoride areas in Ethiopia. Community Dentistry and Oral
Epidemiology. 7: 51-6.
Orcel
P, et al. (1990). Stress fractures of the lower limbs in osteoporotic patients
treated with fluoride. Journal of
Bone and Mineral Research. 5(Suppl 1): S191-4.
Ortiz-Perez
D, et al. (2003). Fluoride-induced disruption of reproductive hormones in
men. Environmental Research 93:20-30.
Paul
V, et al. (1998). Effects of sodium fluoride on locomotor behavior and a few
biochemical parameters in rats. Environmental
Toxicology and Pharmacology. 6: 187–191.
Pendrys
DG, Katz RV. (1998). Risk factors for enamel fluorosis in optimally fluoridated
children born after the US manufacturers’ decision to reduce the fluoride
concentration of infant formula. American
Journal of Epidemiology 148:967-74.
Pinkham,
JR, ed. (1999). Pediatric Dentistry
Infancy Through Adolescence. 3rd Edition. WB Saunders Co,
Philadelphia.
Poureslami
HR, et al. (2011). Intelligence quotient of 7 to 9 year-old children from an
area with high fluoride in drinking water. Journal of Dentistry and Oral Hygiene 3(4):61-64.
Public
Health Service (PHS). (1993). Toward improving the oral health of Americans: an
overview of oral health status, resources, and care delivery. Public Health Reports. 108: 657-72.
Retief
DH, et al. (1979). Relationships among fluoride concentration in enamel, degree
of fluorosis and caries incidence in a community residing in a high fluoride
area. Journal of Oral
Pathology. 8: 224-36.
Riggs
BL, et al. (1990). Effect of Fluoride treatment on the Fracture Rates in Postmenopausal
Women with Osteoporosis. New England
Journal of Medicine 322: 802-809.
Rocha-Amador
D et al. (2009). Use of the Rey-Osterrieth Complex Figure Test for
neurotoxicity evaluation of mixtures in children.Neurotoxicology 30(6):1149-54.
Rozier
RG. (1999). The prevalence and severity of enamel fluorosis in North American
children. Journal of Public Health
Dentistry.59: 239-46.
Sawan
RMM et al. (2010) Fluoride Increases Lead Concentrations in Whole Blood and in
Calcified Tissues from Lead-Exposed Rats.Toxicology. 271
1–2: 21–26.
Schlesinger
ER et al. (1956) Newburgh-Kingston Caries-Fluorine Study. XIII. Pediatric
Findings After Ten Years,” Journal
of the American Dental Association. 52 (3):296–306.
Schnitzler
CM, et al. (1990). Bone fragility of the peripheral skeleton during fluoride
therapy for osteoporosis. Clinical
Orthopaedics.(261): 268-75.
Seholle
RH. (1984). Preserving the perfect tooth (editorial). Journal of the American Dental Association. 108: 448.
Seow
WK, Thomsett MJ. (1994). Dental fluorosis as a complication of hereditary
diabetes insipidus: studies of six affected patients. Pediatr Dent.
16(2):128-32.
Seppa
L, et al. (2000). Caries trends 1992-98 in two low-fluoride Finnish towns
formerly with and without fluoride. Caries
Research.34: 462-8.
Seraj
B, et al. (2006). [Effect of high fluoride concentration in drinking water on
children’s intelligence]. [Study in Persian] Journal of Dental Medicine 19(2):80-86.
Shao
Q, et al. (2000). Influence of free radical inducer on the level of oxidative
stress in brain of rats with fluorosis.Zhonghua
Yu Fang Yi Xue Za Zhi. 34(6):330-2.
Sharma
R et al. (2008). Fluoride Induces Endoplasmic Reticulum Stress and Inhibits
Protein Synthesis and Secretion. Environ
Health Perspect. 116:1142–1146.
Shashi
A. (2003). Histopathological investigation of fluoride-induced neurotoxicity in
rabbits. Fluoride. 36:
95-105.
Shea
JJ, et al. (1967). Allergy to fluoride. Annals of Allergy. 25:388-91.
Sheth
FJ, et al. (1994). Sister chromatid exchanges: A study in fluorotic individuals
of North Gujurat. Fluoride. 27:
215-219.
Shiboski
CH, et al. (2003). The association of early childhood caries and race/ethnicity
among California preschool children. Journal
of Public Health Dentistry. 63:38-46.
Shivarajashankara
YM , et al. (2002). Brain lipid peroxidation and antioxidant systems of young
rats in chronic fluoride intoxication.Fluoride. 35:
197-203.
Shivarajashankara
YM , et al. (2002). Histological changes in the brain of young
fluoride-intoxicated rats. Fluoride. 35:12-21.
Singh
A, Jolly SS. (1970). Fluorides and Human Health. World Health Organization. pp
239-240.
Singh
A, et al. (1963). Endemic fluorosis: epidemiological, clinical and biochemical
study of chronic fluoride intoxication in Punjab.Medicine. 42: 229-246.
Spencer
AJ et al. (1996).Water Fluoridation in Australia. Community Dental Health. 13 (suppl. 2):27–37.
Spittle
B. Fluoride Fatigue: Is Fluoride in Your Drinking Water—and from Other Sources—
Making You Sick? (Dunedin, New Zealand: Paua Press, 2008).
Spittle
B, et al. (1998). Intelligence and fluoride exposure in New Zealand Children
(abstract). Fluoride 31:S13
Sprando
RL, et al. (1998). Testing the potential of sodium fluoride to affect
spermatogenesis: a morphometric study. Food and Chemical Toxicology. 36:
1117-24.
Sprando
RL, et al. (1997). Testing the potential of sodium fluoride to affect
spermatogenesis in the rat. Food and
Chemical Toxicology. 35: 881-90.
Sprando
RL, et al. (1996). Effect of intratesticular injection of sodium fluoride on
spermatogenesis. Food and
ChemicalToxicology. 34: 377-84.
Stannard
JG, et al. (1991). Fluoride Levels and Fluoride Contamination of Fruit
Juices. Journal of Clinical
Pediatric Dentistry. 16: 38-40.
Stecher
P, et al. (1960). The Merck Index of
Chemicals and Drugs. Merck & Co., Inc, Rathway NJ. p. 952
Strunecka
A, Patocka J. (1999). Pharmacological and toxicological effects of
aluminofluoride complexes. Fluoride 32:230-242.
Sun
ZR, et al. (2000). Effects of high fluoride drinking water on the cerebral
functions of mice. Chinese Journal
of Epidemiology. 19: 262-263.
Susheela
AK. (1993). Prevalence of endemic fluorosis with gastrointestinal
manifestations in people living in some North-Indian villages. Fluoride. 26: 97-104.
Susheela
AK and Jethanandani P (1996). Circulating testosterone levels in Skeletal
Fluorosis patients. Clinical
Toxicology.34 (2): 1-7.
Susheela
AK, Kumar A. (1991). A study of the effect of high concentrations of fluoride
on the reproductive organs of malerabbits, using light and scanning electron
microscopy. Journal of Reproductive
Fertility. 92: 353-60.
Sutton
P. (1996). The Greatest Fraud:
Fluoridation. Lorne, Australia: Kurunda Pty, Ltd.
Sutton
P. (1960). Fluoridation: Errors and
Omissions in Experimental Trials. Melbourne University Press. Second
Edition.
Sutton,
P. (1959). Fluoridation: Errors and
Omissions in Experimental Trials. Melbourne University Press. First
Edition.
Teotia
M, et al. (1998). Endemic chronic fluoride toxicity and dietary calcium
deficiency interaction syndromes of metabolic bone disease and deformities in
India: year 2000. Indian Journal of
Pediatrics. 65: 371-81.
Teotia
SPS, et al. (1976). Symposium on the non-skeletal phase of chronic fluorosis:
The Joints. Fluoride. 9:
19-24.
Tsutsui
T, Suzuki N, Ohmori M, Maizumi H. (1984). Cytotoxicity, chromosome aberrations
and unscheduled DNA synthesis in cultured human diploid fibroblasts induced by
sodium fluoride. Mutation
Research. 139:193-8.
Tye
CE et al. (2011). Fluoride Does not Inhibit Enamel Protease Activity. J Dent Res. 90(4): 489-494.
U.S.
EPA (2011). EPA and HHS Announce New Scientific Assessments and Actions on
Fluoride / Agencies working together to maintain benefits of preventing tooth
decay while preventing excessive exposure. Joint press release with DHHS, Jan
7, 2011.
Varner
JA et al. (1998). Chronic Administration of Aluminum-Fluoride or
Sodium-Fluoride to Rats in Drinking Water:Alterations in Neuronal and
Cerebrovascular Integrity. Brain
Research. 78 (1–2): 284–98.
Waldbott
GL, et al. (1978). Fluoridation: The
Great Dilemma. Coronado Press, Inc., Lawrence, Kansas.
Waldbott
GL. (1965). A Struggle with
Titans. Carlton Press, NY.
Wang
C, et al. (2000). Treatment Chemicals contribute to Arsenic Levels. Opflow. (Journal of the American Water
Works Association. October 2000.
Wang
Y, et al. (1997). Changes of coenzyme Q content in brain tissues of rats with
fluorosis. Zhonghua Yu Fang Yi Xue
Za Zhi. 31: 330-3.
Wang
X, et al. (2001). Effects of high iodine and high fluorine on children’s
intelligence and thyroid function. Chinese
Journal of Endemiology 20(4):288-90.
Warren
JJ et al. (2009). Considerations on Optimal Fluoride Intake Using Dental
Fluorosis and Dental Caries Outcomes – A Longitudinal Study. Journal of Public Health Dentistry. 69
(2): 111–15.
WHO
(Online). WHO Oral Health Country/Area Profile Programme. Department of
Noncommunicable Diseases Surveillance/Oral Health. WHO Collaborating Centre,
Malmö University, Sweden.
Williams
JE, et al. (1990). Community water fluoride levels, preschool dietary patterns,
and the occurrence of fluoride enamel opacities. Journal of Public Health Dentistry. 50: 276-81.
Wu
DQ, Wu Y. (1995). Micronucleus and sister chromatid exchange frequency in
endemic fluorosis. Fluoride. 28:
125-127.
Xiang
Q, et al. (2003a). Effect of fluoride in drinking water on children’s
intelligence. Fluoride. 36:
84-94.
Xiang
Q. (2003b). Blood lead of children in Wamiao-Xinhuai intelligence study. Fluoride. 36: 138.
Xu
Y, et al. (1994). The effect of fluorine on the level of intelligence in
children. Endemic Diseases Bulletin 9(2):83-84.
Yang
Y, et al. (1994). The effects of high levels of fluoride and iodine on
intellectual ability and the metabolism of fluoride and iodine. Chinese Journal of Epidemiology 15(4):296-98
(republished in Fluoride 2008;
41:336-339).
Yao
Y, et al. (1997). Comparative assessment of the physical and mental development
of children in endemic fluorosis area with water improvement and without water
improvement. Literature and
Information on Preventive Medicine 3(1):42-43.
Yao
Y, et al. (1996). Analysis on TSH and intelligence level of children with
dental Fluorosis in a high fluoride area. Literature and Information on Preventive Medicine 2(1):26-27.
Yu
Y et al. (1996) Neurotransmitter and receptor changes in the brains of fetuses
from areas of endemic fluorosis. ChineseJ
Endemiology 15: 257-259 (republished in Fluoride 41(2):134-8).
Zakrzewska
H, et al. (2002). In vitro influence of sodium fluoride on ram semen quality
and enzyme activities. Fluoride.35:
153-160.
Zhang,
R., et al. (2009). A stable and sensitive testing system for potential
carcinogens based on DNA damage-induced gene expression in human HepG2
cell. Toxicology in Vitro. 23:158-165.
Zhang
Z, et al. (2001). [Effects of selenium on the damage of learning-memory ability
of mice induced by fluoride]. Wei
Sheng Yan Jiu.30: 144-6.
Zhang
Z, et al. (1999). [Effect of fluoride exposure on synaptic structure of brain
areas related to learning-memory in mice] [Article in Chinese]. Wei Sheng Yan Jiu. 28:210-2.
Zhao
ZL, et al. (1995). The influence of fluoride on the content of testosterone and
cholesterol in rat. Fluoride. 28:
128-130.
Ziegelbecker
R. (1970). A critical review on the fluorine caries problem. Fluoride. 3: 71-79.
Ziegelbecker
R. (1981). Fluoridated Water and Teeth. Fluoride. 14 (3): 123–28.
Zhai
JX, et al. (2003). Studies on fluoride concentration and cholinesterase
activity in rat hippocampus. Zhonghua
Lao Dong Wei Sheng Zhi Ye Bing Za Zhi. 21: 102-4.
Zhao
XL, Wu JH. (1998). Actions of sodium fluoride on acetylcholinesterase
activities in rats. Biomedical and
Environmental Sciences. 11: 1-6
Zhao
LB, et al (1996). Effect of high-fluoride water supply on children’s
intelligence. Fluoride. 29:
190-192.
current petitions
Together
we can change policy. Sign our petitions to help us change health standards:
fan newsletter
Sign
up for our free newsletter and get monthly updates about how fluoride is
affecting all of us.
quick facts
- More people drink fluoridated water in the United States than the rest of the world combined.
- Wine and grape juice made in the U.S. have high levels of fluoride pesticide.
- In Europe, fluoride was once prescribed as a drug to reduce thyroid activity.
- Fluoridation disproportionately harms black children.
· Related Videos:



{kind=link}
· Related Articles:
· Related Studies:
· Related Miscellaneous Content:
No comments:
Post a Comment