Therapeutic DMSO Combinations Revolutionize MedicineHow DMSO being mixed with numerous common medications creates a myriad of remarkable therapeutic possibilitiesStory at a Glance: •DMSO is an “umbrella remedy” capable of treating a wide range of challenging ailments due to its combination of therapeutic properties (e.g., reducing inflammation, improving circulation, and reviving dying cells). •One of DMSO’s unique properties is its ability to enter through the skin and carry anything it dissolves with it as it rapidly travels throughout the body, greatly enhancing the potency and viability of many pharmaceutical drugs. •Because of this, numerous pharmaceutical preparations over the years have combined DMSO with a commonly used drug, and in many cases, demonstrated significant safety and efficacy of this combination to drug regulators. •Some of these DMSO combination therapies are able to treat challenging illnesses, such as significant musculoskeletal injuries, antibiotic resistant infections, persistent fungal and viral infections, chemotherapy resistant cancers, and chronic pain. •More creative combinations (which can be produced at home) have been frequently used to successfully treat tinnitus, a wide range of eye problems (including many “incurable” eye diseases, cancers, and uncomfortable scars (which frequently create chronic illnesses)—all of which will be extensively reviewed in this article. •Many of the most promising uses of DMSO result from combining it with another natural or conventional therapy, as in many cases, a combination can do what DMSO cannot do alone for someone. This article examines the principles for effectively combining DMSO with other therapies to maximize its potential in treating complex conditions. Over the last nine months, I’ve worked to bring the public’s attention to dimethyl sulfoxide (DMSO) a forgotten natural therapy which rapidly treats a wide range of conditions and that many studies have shown is very safe (provided it’s used correctly), and, most importantly (thanks to the 1994 DSHEA act which legalized all natural therapies) is now readily available. Since I believe DMSO has immense potential to offer the medical community and individual patients, I’ve diligently worked to compile evidence that best supports its rediscovery. As such, throughout this series, I’ve presented over a thousand studies that DMSO effectively treats:
While unbelievable, consider for a moment this 1980 report by 60 Minutes that corroborates much of that: Fortunately, much in the same way DMSO caught on in the 1960s, providing that evidence has allowed it to make a rapid resurgence (e.g., I’ve now received over 2,000 stories from readers who have often had remarkable improvements from using it). Combination TherapiesDMSO’s ability to treat a wide range of illnesses results from it having a variety of highly unusual properties that appear to address the root causes of disease. At the same time however, since DMSO has so many different therapeutic mechanisms (e.g., increasing parasympathetic activity, increase circulation, regenerating senescent cells, being highly anti-inflammatory, blocking pain conduction etc.), despite having now reviewed thousands of studies on it, there is still a great deal I do not understand about the substance. As such, one of the greatest challenges throughout this series has been to avoid claiming anything about the substance that's not supported by the existing scientific literature, particularly when it’s a question many want answers to.
Note: after seeing this quote, I queried a few AI systems, which concluded that between 50,000 to 100,000 studies have been published on the medical and chemical properties of DMSO. One of DMSO’s most noteworthy abilities is its ability to enhance the effects of other substances, which in many cases makes it possible to surmount major dilemmas traditionally seen with those therapies. Unfortunately, since there is an almost infinite number of substances one could combine with DMSO’s function as a “vehicle” remains one of the least studied aspects of the compound, and is specifically for that reason I had this subject be the last major part of the series. Likewise, over the years I have come up with so many different potentially promising therapeutic DMSO combinations, but I still have not been able to try most of them. This is particularly important, as while DMSO helps the majority of recipients (e.g., around 85-90% of readers reported relief from chronic pain) in many instances where DMSO alone is not sufficient to address an ailment (e.g., pain), a combination therapy will. Note: DMSO (alone or combined with other agents) can be administered in a variety of ways such as a liquid (sometimes applied with a cotton swab, brush, or gauze), a cream, gel, roll-on or spray; taken internally as an oral solution, infusion, or injection; nebulized or used as eye drops, ear drops, nasal drops, mouth rinses, enemas, and bladder irrigations. In many cases, multiple modalities are done concurrently (e.g., oral and topical DMSO is often quite helpful for systemic arthritis). Combining DMSOIn pharmacology, DMSO is often referred to as a “vehicle” that helps other drugs get into the body. Because of this, while DMSO only has one approved (intravesical) use (which has led to many thinking it must not be safe), a variety of drugs are on the market that use DMSO as a vehicle to bring them inside the body. This is because DMSO is a unique solvent that: •Will pass through biological membranes without damaging them (which is extremely unusual and believed to be due to its exchange and interchange with water in biological membranes). •Once it contacts the skin, it rapidly spreads throughout the body (e.g., within an hour of being applied to the skin, it can be found within the bones and teeth). • It is a highly potent solvent that can dissolve a wide range of substances. •If a substance is dissolved within DMSO, DMSO can typically bring it into the body. While a few other substances can also serve as vehicles, DMSO is the most potent in pharmacology (e.g., this study found that DMSO was more effective than propylene glycol at delivering topical steroids into the body). Note: after a report of copper chloride and DMSO coloring someone’s skin, a team attempted to replicate this effect with a variety of dyes but were unable to do so (nor could they alter autoimmune skin discoloration). •In addition to bringing substances into the body, DMSO also greatly increases circulation and by taking the place of water (as it is small, can form hydrogen bonds and is relatively polar) while being both fat and water soluble, changes the permeability of the cell membrane, allowing new things to enter the cell and waste products to leave cells. As a result, DMSO is able to both spread what it transports throughout the body and significantly enhance the body’s innate ability to circulate what has already been absorbed (including to previously inaccessible areas). As such, DMSO enables the topical administration of drugs that would normally require injection, and in many cases, can significantly increase their potency (e.g., because it penetrates deep regions of the body that pharmaceuticals typically have difficulty entering or because it bypasses the barrier that cells have to foreign substances). Note: there are likely other reasons why DMSO increases the potency of substances mixed with it, but the ones I’ve looked at are more speculative and did not have enough evidence supporting them. Decades ago, I had a friend who used DMSO to get high by mixing it with street drugs who shared that the high from it was much stronger than what one would experience from injecting the drug (which is traditionally the strongest high one can experience) and that their group quickly realized they could only do this with pharmaceutical grade drugs as street preparations had a variety of impurities which frequently made them get quite ill when taking them. About ten years after sharing this with me, my friend died from a drug overdose (which did not involve DMSO). In contrast, most of the people I know who’ve mixed DMSO with natural substances either had positive to neutral experiences at worst. In my eyes, there are a few key lessons from this story: 1. One of the major risks of DMSO is applying it to the skin if a toxic substance is already present. For example, in 1965, the German Magazine Der Spiegel (No. 19) shared that the original investigator of DMSO:
Likewise, within the thousands of comments I’ve received here, a reader shared a case they heard of where someone accidentally got a (fortunately non-fatal) overdose of nicotine because it was on the skin DMSO was applied to, causing it to be rapidly absorbed into their system. Because of this, we always emphasize the importance of cleaning the application area before applying DMSO. Remarkably, aside from these precautions, to the best of my knowledge, no one has reported (either to me personally, in the literature, or within the DMSO community) becoming seriously ill from applying DMSO to skin that had a contaminant or toxin on it. This suggests that users have been consistently diligent about cleaning beforehand, or that the actual risk is limited to highly toxic substances—i.e., most compounds typically present on the skin are not harmful enough to cause systemic toxicity when absorbed through DMSO. Note: one possible explanation for this unexpected outcome is that DMSO, as a bidirectional “channel opener,” may not only enhance the absorption of compounds into tissues but also facilitate their excretion—helping to mitigate any potential harm. 2. Many agents will become significantly more potent when mixed with DMSO. With natural substances, this is generally not an issue (as their potency and toxicity are typically much less than pharmaceuticals), but it is still a real risk to consider. Despite this, I have not run into reports (either in the literature or from readers) of a natural combination DMSO therapy creating serious issues (which was quite surprising). 3. Since very little quality control exists for them, one of the major problems with street drugs are all the things they are cut with (or impurities that accumulate during the manufacturing process). For this reason, even though many people over the years have used DMSO as a creative way to get high, I strongly advise against doing this (especially since there is also the risk of an overdose if too much is given at one time). 4.
This same impurity issue could apply to anything else too. For this
reason, whenever making DMSO mixes that others have had success with, it
is essential to obtain a pure mixture (e.g., many pharmaceutical and
supplement preparations contain multiple ingredients beyond the primary
pharmaceutical). As such, caution should be taken when taking potent pharmaceuticals at the same time as DMSO. Presently, I’ve reviewed a lot of published reports and reader stories where a pharmaceutical drug was mixed with DMSO and applied topically with no issues following, however to the best of my knowledge, none of those were with drugs that can easily cause overdoses. The one exception comes from Jim McCann (a longtime DMSO practitioner), who reported seeing cases of individuals becoming seriously ill when an IV was given that contained both DMSO and an (unspecified) anticoagulant or steroid. Given that topical preparations of heparin (which was the IV only anticoagulant in use at McCann’s time) and steroids mixed with DMSO have caused no issues in clinical trials, if his observations were correct (which they may not have been), I suspect they resulted from both being infused together in an IV. At the same time however, while drug potentiation is a potential safety concern, it is also invaluable in medicine. This is because frequently, it is quite difficult to get a drug to its target site in the body, requiring sustained high doses of it so that enough of the drug arrives at the target site (which can require exposing the body to a toxic dose). DMSO Drug InteractionsGiven
DMSO’s ability to potentiate pharmaceuticals, this raises an obvious
question—is it safe to take it alongside other drugs? The best answer I
can share is that: •If a pharmaceutical is fairly toxic (e.g., gadolinium for an MRI), it’s generally a good policy not to take it alongside DMSO. •Likewise
if you are taking other drugs, starting with a low dose of DMSO and
gradually working it up is advised (so you can monitor for side
effects). Presently, the specifics we know on this topic are as follows: •In a 1967 report of 500 cases,
investigators noted that a few of the patients concurrently on a
medication (2 on insulin, 2 on digitalis, 1 on nitroglycerine and 1 on
quinidine sulfate) had the effects of their drugs increase and needed to
be switched to a lower dose (whereas other drugs like the psychiatric
ones of the era were never potentiated). •DMSO has been observed to enhance the potency of certain opioids (e.g., morphine patches), NSAIDs, Novalgin, anticonvulsants
(e.g., gabapentin), sedatives (e.g., trazodone), corticosteroids, gold
salts, insulin, barbiturates, and antibiotics—which in many cases can be
extremely advantageous. •In
a sample of roughly 10,000 people receiving antibiotics and DMSO
concurrently, 4 reported experiencing significant reactions from the
drugs that typically are very rare, suggesting a potentiation of
toxicity occurred, which I believe followed either a fluoroquinolone,
sulfonamide or macrolide, with the most severe following a
fluoroquinolone (while in contrast DMSO did not potentiate other toxic
antibiotics like dioxidine). Likewise, while DMSO typically improves chemotherapy,
there have been a few reports of rare but significant side effects
sometimes seen with chemotherapy drugs in individuals taking both
concurrently. •A few compounds have been shown to become more toxic with DMSO (e.g., mice and rats given quaternary ammonium salts showed increased toxicity when pentolinium tartrate and hexamethonium bitartrate were dissolved in DMSO, but not when given alone, and DMSO also increased the lethality of benzene), while in contrast other toxic substances (e.g., decamethonium iodide) became less toxic with DMSO. •Other non-pharmaceutical interactions can also occur. For example, DMSO neutralizes chlorine in drinking water (reducing it to chloride) providing an emergency way to “purify” chlorinated water. Carrying SizeMany
of the bacteria in your mouth are highly pathogenic. Nonetheless, (to
the best of my knowledge), no one has gotten sepsis from putting DMSO
into their mouth. This is because while DMSO (a very small molecule) is
extremely effective at transporting things inside the body, as things
get larger, DMSO can no longer transport them, and even the smallest
viruses are far larger than DMSO’s maximum carrying size. Much of this was originally learned after the discovers of DMSO realized a non-injectable way to administer insulin would be extremely helpful for diabetic patients, but regrettably discovered this didn’t work as insulin (a peptide) was too large to enter the body with DMSO. In contrast, most natural chemicals and pharmaceutical drugs are within DMSO’s size limit and hence can be absorbed. Note: DMSO’s ability to function as a vehicle increases with increasing DMSO concentrations, but in some cases, 90% DMSO is a more effective carrier than 100% DMSO. As
best as I could tell, the exact skin carrying limit of DMSO has not
been definitively studied, and most current sources agree it transports
substances less than 500 Daltons (Da), and may to a lesser degree
transport those between 500-1000 Daltons (whereas insulin is 5808 Da). I suspect the actual limit is higher, as I’ve seen many cases of larger drugs that are clearly being transported (e.g., ivermectin is 875 Da). Stanley Jacob found that DMSO significantly increased the penetration of heparin into dog urinary bladders.1,2,3 Likewise, many studies have found a DMSO-heparin gel was therapeutically active in patients. Heparin for context has a molecular weight of 2,000-30,000 Da (typically averaging 12,000-15,000 Da or 4,000-6,000 Da for low weight formulations), greatly exceeding the 500 Da threshold, suggesting either that the 500Da limit is wrong, that all of those studies and outsiders investigating them made an erroneous conclusion (e.g., benefits attributed to DMSO-Heparin were just due to DMSO), or that heparin being extremely electronegative increases DMSO’s ability to transport it. Note: a Dalton is equal to the mass of a Hydrogen atom, so a strand of human DNA is approximately 2,080,000,000,000 Da, whereas aspirin is 180.16 Da and prednisone is 358.43 Da. Lastly, that limit (which is not constrained by the skin) appears to be much higher inside the body. For example, there is some evidence suggesting DMSO can bring molecules larger than 70,000 Da through the blood-brain barrier (suggesting an even wider range of possibilities for DMSO IV mixtures). Unwanted AbsorptionAs DMSO is a powerful solvent, it can easily dissolve many substances with which it comes into contact. Because of this, a major concern with DMSO is whether it will interact with the materials you prepare and administer, as well as with medical materials already present in the body, once it is administered. Having extensively looked at this, the DMSO community has concluded the following: •With plastics, many of the most problematic components are all additives on their surface (e.g., phthalate plasticizers, flame retardants, etc.). Because of this, if you pre-treat them with concentrated DMSO and then wash them out, they will be removed and not have as much leached by subsequent DMSO applications. This in turn, can be useful when plastic has to be used (e.g., for a spray bottle) or to prevent general plastic exposure (e.g., by removing chemicals from a hood that needs to be worn for a prolonged period). •DMSO’s ability to leach is concentration dependent and within the DMSO community is thought to occur minimally for plastic at concentrations below 20%, so many potential issues can be avoided by ensuring DMSO intended for the body does not touch plastic surfaces at high concentrations. While I could not locate studies corroborating the 20% threshold, I did find one study that determined that less than 80% does not quickly leach plastic, while less than 55% does not leach it after long term storage. Because of this, 15% is often advised as a concentration to work with while preparing DMSO. •
When DMSO is administered into the body, it rapidly dilutes. Because of
this, if topical DMSO is applied over an artificial joint or taken
orally, it is unlikely to reach a significant concentration at the joint
(whereas it might if injected directly into the joint). While I am not
sure how to estimate the actual concentration topical DMSO creates at a
joint below, no doctor I know, nor anyone in the DMSO community, has run
into DMSO creating issues for metal joints (particularly since DMSO
does not react with metal surfaces). •While
metal is resistant to DMSO, many implants (including artificial joints)
have plastic components that could leach. As this is most likely to
matter for components of dental implants (or toothbrushes), lower DMSO
concentrations are advised for mouthwashes. • The one area where issues are observed is with plastic external surgical sutures, as applying highly concentrated DMSO to them can cause them to harden and break. Conversely, no issues have been noted with dissolving internal sutures (which being deeper will contact more diluted DMSO) although issues could also be occurring but simply remain unnoticed due to them being inside the body. •In the case of breast implants, it’s not clear if DMSO will react with the less reactive-silicone, but in many cases, individuals develop breast implant illnesses due to small amounts of the components of the implant leaking, which DMSO would be more likely to react with. Conversely, a rat study found that DMSO effectively reduces capsule formation (e.g., fibrotic tissue) around silicone breast implants (something which can often be quite difficult to treat). •When
working with or preparing DMSO, especially the initial higher
concentrations, it is advised not to use plastic containers or utensils
(instead use glass, metal, ceramic, porcelain, or natural brushes). In
cases where it will be injected, using pre-diluted DMSO is considered
ideal, and in the early days of DMSO, investigators ran into issues
by directly drawing pure DMSO and putting it into plastic syringes and
IV tubing, and when this cannot be avoided, the DMSO community advises
pre-rinsing the syringes with DMSO (as injected applications have a
higher risk of bringing too many toxins into the body than topical
ones). •As
there are many theoretical risks of DMSO reacting with cataract lens,
many potential concerns have been raised around DMSO eye drops and they
are often advised against out of caution. However, when doctors attempt
to investigate, they often cannot obtain clear answers. That said, most
of the materials used to make cataract lenses are somewhat DMSO
resistant, with the one exception, polymethylmethacrylate, having been
largely phased out a bit over 20 years ago (although it is still used in
poorer areas). Because of this, the DMSO community advises using low
DMSO concentrations for eye drops, and has found they both provide
dramatic improvement for a wide range of visual issues and have never
caused issues with cataract lenses. •If DMSO is left to settle for a while, leached plastic is often detectable because the DMSO becomes cloudy (which can sometimes be observed in packaged DMSO products). Likewise, in many cases it’s possible to observe if leaching has occurred (due to changes in plastic) but in many other cases, plastics with small areas which briefly contact DMSO will show no signs of leaching over many years. Additionally, individuals often enquire if DMSO can be used over tattoos (and in some cases, DMSO is used to dissolve tattoos). As so many different inks of varying toxicity are used, many (myself included) believe a potential risk exists that should be avoided, particularly with higher DMSO concentrations being applied to those areas. Note: synthetic cosmetics are much more problematic to mix with DMSO than natural ones. For this reason, users are often advised to use lower concentrations on their head (e.g., 10%). Finally, once applied to the skin, DMSO can have a limited ability to carry other substances it comes into contact with for a few hours. If you wish to wash it off (so nothing else can mix with it) most gels and liquid formulations are water soluble, whereas most creams and ointments are not and hence require soap to be washed off. DMSO Pharmaceutical Combination StudiesA variety of pharmaceutical drugs have been combined with DMSO over the years.
Note: I was unable to confirm whether three of these products contained DMSO. Additionally, a few are DMSO only, rather than a combination of DMSO and other substances. Finally, a longer list of DMSO containing products can be found here. With the majority of these products, they took an existing drug that had similar effects to DMSO (typically musculoskeletal or dermatologic) and enhanced them once DMSO was combined with it. In each package insert I’ve read through, DMSO was typically described as a safe and inert ingredient. This is noteworthy as: •DMSO is still erroneously viewed as being dangerous (as that was the FDA’s justification for their decision to spend decades stonewalling it). Due to this, in both Europe and the United States, DMSO is an approved active pharmaceutical ingredient; however, with the exception of RIMSO-50, the FDA has not approved DMSO alone as a pharmaceutical drug. •Many people still believe DMSO is an unproven and rarely used therapy, whereas in reality, it is many different pharmaceutical products. In short, while DMSO is an “unproven” “dangerous” and “unapproved” “fringe remedy,” once combined with another patentable drug, it magically becomes “safe and effective.” Additionally, a few more unusual DMSO pharmaceuticals exist: •Mekinist, a targeted cancer therapy which uses DMSO to stabilize it, enhances its solubility in water (and possibly to increase its penetration into tumors). •Prochymal, a stem cell product for preventing tissue rejection which uses 10% DMSO to preserve the stem cells. •Onyx,
a liquid which is injected into blood vessels to plug leaks or abnormal
vessels as it will solidify at problem areas. It uses DMSO to dissolve
Onyx’s polymer (so it can be liquid) as DMSO is a (fairly unique) safe
substance which can perform that role. A similar product, Tegress, was previously used to coat and thicken the urethra to reduce incontinence. •Viadur is a non-degradeable implant for prostate cancer containing Lupron (a fairly toxic hormone suppressing drug) dissolved in DMSO that is designed to slowly release Lupron into the body over the course of a year. DMSO is used here as Lupron is otherwise hard to dissolve (and unless dissolved cannot be pumped out by the implant), DMSO preserves Lupron’s stability for a prolonged period and because it is a non-toxic option. Note: adverse reactions to pharmaceuticals are tracked in FAERS. In FAERS, very few reactions have been reported from DMSO, and most of the severe ones came from these non-standard products (e.g., Onyx or stem cell preparations). I will now review the common DMSO therapeutic combinations, both to shed light on some ways they can enhance existing pharmaceutical therapies, but more importantly, to help you understand some of the general principles behind DMSO combination therapies. Note: almost all of the combinations that follow were for conditions where DMSO’s efficacy was extensively studied in the 1960s. As such, I believe that if DMSO research had continued, many other promising therapeutic combinations would have been considered. Heparin CombinationsHeparin is one of the oldest anticoagulants, and something I believe in part works by improving zeta potential, as due to its numerous sulfate (and carboxylate) groups, has the most negative charge density of any known biomolecule (making it a strong zeta potential restoring agent). Unfortunately, heparin cannot be absorbed orally, so it is typically reserved for the hospital setting where it can be injected, hence making DMSO quite valuable for its ability to bypass this need. The one study I am aware of that clearly compared DMSO alone to DMSO plus heparin found a significant benefit from the combination in rheumatoid arthritis.
Note: another DMSO investigator also found that ultrasound enhances the potency of DMSO by directing it into target tissue and used this approach to treat a variety of foot issues. A third investigator used this approach to treat roughly a dozen spinal disc issues (e.g, a deteriorated disc causing radiculopathy) by applying topical DMSO and then using ultrasound to direct it to the affected disc. Finally, a rat study found that topical DMSO mixed with gold particles and then directed with ultrasound towards muscular injuries in rats reduced muscle damage and signs of oxidative stress. In Germany, roughly fifty years ago, Dolobene, a gel, was developed which combined: In the 1980s, Dolobene was one the leading topical medications for sports injuries arthritis, but I could not discern if that is still the case (however it is still widely available). Numerous studies from that period, in turn, corroborated its value both for those conditions and complications of varicose veins (another condition which has a strong response to DMSO): •A study of 78 patients (mostly athletes) with overstrained tendons received Dolobene for 2-3 weeks three times a day, with over 50% having a significant improvement of symptoms and those improvements including a 94% improvement in pain, a 55% improvement of swelling, 95% improvement of redness and 92% improvement of warmth. •A study gave Dolobene gel to 30 athletes with soft tissue injuries of the upper and lower extremities twice daily for 4 weeks. There were 4 athletes with contusion of the shoulder, 8 with distortion and contusion of the knee joint, 8 with muscle, tendon and ligament lesions, and 10 with distortion of the ankle joint. Following DMSO, 10 had an excellent response (improvement), 5 had an excellent to good response, 10 had a good response and 5 had a moderate response. Specifically, pain, inflammation, swelling, reabsorption of hematomas, tenderness and recovery time were assessed. •A study gave Dolobene gel and ultrasound to 15 subjects who had received a blunt-tissue trauma (without fracture) to the lower extremity within the last 24 hours. Compared to 15 placebos, the treatment resulted in a faster relief of pain, reduction of edema, and recovery of mobility. •A study gave 44 patients with spontaneous and postoperative phlebitis, periphlebitis, phlebitis following shrinking, chronic edema, hematoma, and traumatic injuries (many of which were due to varicose veins). A variety of factors were evaluated (e.g., leg pain and heaviness, pain intensity, swelling or indurations), with 75% of patients having a noteworthy improvement in over half of the parameters evaluated. •Another study of 41 patients who had undergone varicose vein surgery, undergone varicose vein obliteration, or who had acute thrombophlebitis gave the participants Dolobene Gel for up to 31 days. Of the 34 who could be evaluated (as six were taking other therapies and one died from prostate cancer), all experienced a good or very good results:
Note: each of these symptoms was mild, moderate or severe for the patients, with 77% having severe symptoms. A study of 38 patients with superficial thrombophlebitis found that after a day, 59.5% reported improvement or were already free of symptoms, by day 4 most symptoms had resolved (e.g., 91.9% of resting pain, all severe pressure pain, 71.7% of redness) and later further improvements were seen (e.g., on day 6, 92.1% were free of all pressure pain, and by 7, 84.2% of all cord like inflammation around the inflamed vein). Lastly, a 1984 study found it effectively treated pretibial hematomas, while a later 1999 study found Dolobene plus acupuncture was an effective treatment for joint sprains. Since Dolobene has been an effective medication, a variety of similar DMSO products with similar musculoskeletal indications (most of which overlap with what DMSO does alone) have been used for a long period in Europe. These include: •Sinedol and Roll-Bene (heparin and dexpanthenol). Lastly, while many forms of pure DMSO are sold in pharmacies around the world (e.g., Dimeksid in Russia and sterile injectable preparations in Europe), in America, DMSO’s only clinically approved indication is putting it directly into the bladder (intravesically) to treat interstitial cystitis (painful inflammation of the bladder). While this works, it does not in every IC case. According to Stanley Jacob:
Note: in one of the studies Jacob cited, IC patients who did not respond to a single agent (DMSO, silver nitrate, or chloropactin) responded to the heparin-containing combination, while in the other study, patients given that combination had not previously been treated for IC. NSAID CombinationsNSAIDs are one of the most widely utilized medications for pain and injury, despite often having limited efficacy and significant systemic toxicity (e.g., they cause gastric bleeding, heart attacks, and kidney damage—which collectively kill tens of thousands of Americans each year). One attempt to reduce their toxicity has been to apply a topical NSAID (e.g., diclofenac in Voltaren gel) to an irritated area so the systemic absorption and hence systemic toxicity can be reduced (which has been corroborated by numerous studies1,2,3,4). While Voltaren is the most popular option, a few approaches have also been utilized which combine DMSO with a NSAID (e.g., one form of Dolobene
includes ibuprofen, a variety of NSAIDs are sometimes mixed with DMSO
by compounding pharmacies for human or animal use), as this greatly
increases its absorption, allowing it to affect the injured area. In the United States, the only FDA-approved topical DMSO combination is Pennsaid (45% DMSO with diclofenac). In a 2004 randomized controlled trial used for its 2009 approval, this combination was found to have minimal systemic toxicity (the primary issue was topical skin irritation—which was greater in those receiving the combination), and that DMSO alone (the placebo) on average improved symptoms by 28.5% whereas DMSO plus diclofenac improved symptoms by 39.925%. Following this, a subsequent trial for the approval of a DMSO higher dosage had similar results.
Note: given the industry tendency to exaggerate the benefits of their therapy, it is likely that the actual benefit from DMSO alone was greater than these trials implied. Additionally: •A meta-analysis corroborated the previous and included a 2004 and 2005
controlled trial which like the other 2004 study found DMSO alone
created an improvement, but a greater improvement was seen with DMSO +
diclofenac. •When
topical DMSO-diclofenac was compared to oral diclofenac, it was found
to be as effective in reducing pain, but much less likely to cause
systemic side effects (e.g., GI complaints or abnormal laboratory
values). Another trial found the same and that combining the two did not increase the toxicity seen from oral diclofenac. •A study of 25 users found DMSO-diclonfenac was more pleasant to put on than Voltaren (diclofenac plus a different vehicle). These studies hence demonstrate both the safety and efficacy of this combination, making it quite unfortunate most physicians are not aware it exists within the conventional medical system as they instead routinely prescribe far more toxic NSAIDs. Note: DMSO alone as a 90% gel (sold as DOMOSO) is FDA approved for acute swelling due to trauma in dogs and horses. Pennsaid was approved in 2009, had a new Pennsaid formulation approved in 2014, and developed a foam-based ibuprofen DMSO formulation) but that company disappeared through a series of mergers and acquisitions.1,2,3 After the patent for Pennsaid ran out, another company also began producing it.1,2,3 Additionally, a Greek company produces the same combination (Inflaforte®). Note: much in the way Pennsaid bypasses the gut (hence preventing gastric bleeding) one reader shared that dissolving aspirin powder in DMSO and applying it topically addressed their pain while allowing them to avoid the stomach irritation oral aspirin causes. Steroid CombinationsCorticosteroids (steroids) have a wide range of significant side effects which increase with increasing doses and prolonged systemic use. However, early on, it was observed that DMSO increased their potency. For example: •Investigators found that 0.025% fluocinolone in DMSO was more efficacious than 0.025% fluocinolone alone for a wide range of conditions and that an equivalent efficacy was seen with 0.2% fluocinolone, suggesting DMSO makes the steroid ten times as potent and thus requires a much lower dose. •Mixing DMSO with a steroid made it between 10 to 1000 times more potent in stabilizing lysozymes Because of these early results, the pioneers of DMSO suspected that combining the two could make it possible to use much lower steroid doses and bypass their toxicity. Unfortunately, systemic applications remain unexplored, and no FDA-approved DMSO steroid combinations exist. However, I have read numerous reports online where taking DMSO allowed them to greatly reduce their steroid dose (e.g., for vasculitis). Note: while no human combinations exist, some compounding pharmacies will compound them. In contrast, a few combination veterinary products exist. Synotic® is 60% DMSO and 0.01% fluocinolone and FDA approved for ear inflammation in dogs, while Otiprin N, a dexamethasone combination has a similar approval in Europe and Flucort Domoso is marketed in Australia. Likewise, a 99% DMSO 0.05% dexamethasone combination for a wide range of musculoskeletal and dermatologic conditions and another dexamethasone combination for a variety of skin conditions are approved in Germany—some of which have other drugs too (e.g., chloramphenicol, benzyl benzoate, and lidocaine). Most of the trials which have been conducted for DMSO steroid combinations were used for dermatologic or musculoskeletal conditions. The studies are as follows: Safety and Distribution•When a variety of dyes were put onto the skin, researchers found
they thoroughly stained the stratum corneum (a surface layer of the
skin) but rarely went deeper, and that similar penetration was seen with
hydrocortisone, methylene blue, and the antiseptic hexachlorophene (with it staying there for up to 16 days and having increased antibacterial activity). •A 1967 study found 90% DMSO caused a fourfold increase in the absorption and excretion of topical corticosteroids or testosterone while a 1968 study
of 224 patients found 70% DMSO gel mixed with triamcinolone acetonide
produced a comparable result to wearing a cumbersome
(triamcinolone-containing) occlusive dressing. Additionally, a 1967 study
showed corticosteroids or estrogen mixed with DMSO has a comparable
systemic effect to equivalent doses injected subcutaneously. •A dermatologist who treated 613 patients successfully with 50% topical DMSO combined with the steroid triamcinolone acetonide reported that out of 363 who were evaluated, no systemic reactions occurred except for one patient who felt “jittery,” after use over a large area). Skin Conditions•A 1967 study found that topical DMSO and 0.025% fluocinolone treated the following conditions:
Note: a 1966 case study used this same combination to treat a woman’s widespread lichen sclerosis and alopecia (which had eliminated all of her hair). •A 1976 clinical trial
found DMSO and topical corticosteroids were very effective in treating
plaque-type psoriasis that was resistant to steroid treatment (with a
complete disease resolution occurring in 3-4 weeks). Additionally, the
steroids synergistically counteracted the irritation sometimes seen with
higher concentrations of DMSO. •A 2009 study found DMSO, combined with topical corticosteroids, was very effective in resistant plaque-type psoriasis and could completely clear it in 3–4 weeks. •DMSO and 0.025% fluocinolone significantly reduced the reactivity of cosmetic pulsed ruby lasers created on the skin. •After demonstrating with a tracing isotope (Xe133) that DMSO transported substances through the body, in 1975 a team of dermatologists over 3 years discovered that a DMSO combination spray (containing 20% DMSO, 5% diphenylbutazone, 0.2% sodium-rutin sulfate, and 0.5% prednisolone) was an effective treatment for a variety of venous disorders of the extremity and that all three in combination were more effective than any one alone with DMSO.
Rheumatoid Arthritis•A 1968 study found that DMSO combined with hydrocortisone or procaine was more effective than DMSO alone (which was still effective) and within 1 week of treatment improvement was seen in 5 out of 8 rheumatoid patients, 17 of 20 patients with inflamed nerve roots and 8 out of 10 with disc pain. •A 1979 study treated 343 arthritic patients (320 with RA and 23 with deforming arthritis), with either DMSO or a DMSO combination. In the DMSO only group, 64% had significant improvement, and when heparin, sodium salicylate, or hydrocortisone was added, this increased DMSO’s efficacy (e.g., there was a quicker decrease in pain, along with an improvement in joint function). •Another 1967 study of Rheumatoid arthritis found mixed results with using DMSO or a DMSO steroid preparation (about half responded to each therapy), but a significant amount of information was missing from this study. •Another study found that DMSO mixed with hydrocortisone was much more effective than a (no longer sold) NSAID antidepressant combination for rheumatoid arthritis. •A 1967 study found that DMSO could treat acute RA exacerbations triggered by corticosteroid withdrawals (providing relief in 5-10 minutes for as long as 6 hours) and that it reduced the needed steroid dose for patients with extensive RA (with a 77.7% success rate being seen in the 36 treated cases). Additionally: •A 1978 study treated pharyngeal lymphoid hyperplasia (pharyngitis) in horses with a throat spray containing 150ml dimethyl sulfoxide,+ 350 ml nitrofurazone solution, + 1000 mg prednisolone. •DMSO with dexamethasone was found to rapidly transform cancerous cervical cancer cells into normal ones and healed the surrounding cancerous tissues, with 6 out of 6 patients receiving this protocol being treated (including one with metastatic cancer). 5-Fluorouracil5-FU is a chemotherapy drug that has long been used for a variety of cancers and certain skin conditions. Actikerall is a 5-FU and salicylic acid combination approved in Europe and Australia for the treatment of actinic keratosis (skin growths). It contains DMSO, but that component is typically not mentioned or referred to as an “inert” ingredient. Verrucare and Verrumal also contain these three ingredients and are instead used for the treatment of warts. 5-FU with DMSO has been shown to: •Treat skin cancers as this 1967 study found DMSO significantly increased 5-FU’s potency and made a 5% concentration able to locally treat keratoacanthoma, superficial basal cell and early stage squamous cell carcinoma without causing any adverse effects. •Treat seborrheic keratosis and to treat common warts. •Drops of DMSO combined with 5-FU (in 70% ethanol) was found to be an effective Treat nail psoriasis (in a 20 patient series), with the best results seen for pitted nails, leukonychia, and oil spots, whereas marginal results were obtained for onychodystrophy and crumbly nails along with paronychia (inflammation of skin around the nail) resolving. 5-Iodo-2'- Deoxyuridine5-IDU was a nucleotide analog that had potent antiviral activity against herpes and shingles. Unfortunately, it has difficulty penetrating the skin, so its use is largely restricted to herpes in the eye. However, early on, DMSO researchers realized DMSO surmounted this challenge and conducted numerous clinical trials showing it was an effective treatment for herpes and shingles, resulting in the products Zostrum (90% DMSO 1% IDU for shingles) and Virunguent (1.8% DMSO 0.2% IDU for herpes) coming to market in Europe or New Zealand in the 1980s. Note: while DMSO generally increases the potency of IDU (and many other drugs) in one study (for herpes in the eye), it was found to be less effective than saline (possibly due to DMSO transporting it too quickly). Unfortunately, as the decades passed, it was forgotten, and this excellent therapy was overlooked. For this reason, I have summarized all the data on it in this article. Briefly it is as follows: •A 1965 study of 7 patients with severe cutaneous Herpes simplex infection all of whom had significant improvement. •A 1966
blinded trial of 21 patients with recurrent herpes where IDU alone did
nothing DMSO alone halved the duration of a flareup and DMSO-IDU cut its
length to a third and prevented recurrences. •A 1967 study found DMSO plus 5-IDU was more effective for treating early severe herpes simplex lesions than DMSO alone. •In 1972, a physician reported success using 100% DMSO and 5% IDU to treat severe herpes simplex in 5 patients. Likewise, in 1967 5-IDU plus DMSO was reported to be more effective than DMSO for herpes. •A 1990 RCT gave 80% DMSO mixed with 15% IDU to 301 with a recurrence of genital herpes, and found it reduced the mean duration of pain by 1.3 days and the healing time to loss of crust by 1.7 days. When only classic herpes lesions (vesicle, ulcer, or crust formation) were evaluated, a greater effect was seen (the duration of pain was reduced by 2.6 days and the healing time to normal skin by 2.3 days). •Two 1970 RCTs showed that both 5% and 40% IDU in DMSO were effective (with 40% IDU being more effective) over 4 days of repeated applications in reducing shingles, pain, and how long it took the lesions to heal.
•A 1974 RCT of 118 patients found 100% DMSO and 5% IDU applied every 4 hours for 4 days significantly shortened the vesicular phase, healing time, and duration of pain, while significantly improving post-herpetic neuralgia. •A 1979 study found that 40% DMSO plus IDU created a small but significant improvement in the healing of shingles. •A 1981 trial gave 46 shingles patients either DMSO or DMSO mixed with 5% IDU. Compared to DMSO alone, DMSO plus IDU significantly reduced the time it took pain to improve, and significantly fewer new vesicles developed. •A 1992 RCT of 171 patients with non-severe shingles (which had been present for less than 4 days) found that compared to acyclovir, 40% DMSO topical mixed with IDU was a superior treatment for how quickly all vesicles dried, how long moderate-intense pain, hyperaesthesia and itching lasted, and how long reducing medications were required, how frequently new vesicles appeared, and in preventing post-herpetic neuralgia. •Additionally, a 1983 study found that DMSO effectively brought acyclovir (ACV) into the skin, caused a moderate reduction in herpes lesions, and dramatically reduced them when combined with acyclovir.
•Likewise, a 2006 case report discussed using IV DMSO mixed with acyclovir to treat a horse with myeloencephalopathy (dangerous brain and spinal cord inflammation) from equine herpesvirus-1. Note: DMSO also helps herpes fever blisters, and DMSO with IDU has been reported to be effective in treating HSV whitlow (herpes on the fingers). Infection Combination TreatmentsIn addition to exhibiting significant antiviral activity (e.g., against herpes and shingles), which is enhanced by antiviral therapy, DMSO also displays antiviral, parasitic, and fungal activity, which is significantly enhanced when combined with an antimicrobial agent. From reviewing the body of literature on this topic (which I compiled here), the following uses stand out for these applications: • Potent topical medications, such as 5-IDU, which normally cannot penetrate the skin, can do so with DMSO and exert their antimicrobial activity (e.g., this is the case for the antifungal griseofulvin). •Infections deep within the skin that are typically challenging to eliminate can be eliminated if the topical antimicrobial agent is mixed with DMSO. •DMSO causes antimicrobial resistant organisms to lose their resistance, thereby making it possible to eliminate these superbugs (which has been best most conclusively shown with tuberculosis—an infection whose widespread antibiotic resistance has become a global health problem). In parallel, it often lowers the lethal antibiotic concentration required to eliminate an infection, thereby reducing both cost and toxicity. •DMSO makes it possible to reach infections deep within the body that would normally require high and prolonged antibiotic doses (which has been the most conclusively shown for osteomyelitis). This is particularly useful for dental infections as they can be deep enough it is difficult to reach them with standard antimicrobial therapies. •While
this has rarely been explored, certain medications which typically need
to be chronically taken in an IV fashion (which is a pain) such as some
of the antibiotics used for Lyme disease could instead be given as
topical preparations (and likely bypass creating as much damage to the
microbiome as oral antibiotics). Bacterial InfectionsDMSO’s ability to potentiate antibiotics is well recognized throughout the scientific literature. For example, a 1966 study found that 5% DMSO increased bacterial antibiotic sensitivity, both in antibiotic sensitive strains and in many antibiotic resistant strains. For example, all 4 strains of colistin-resistant pseudomonas became sensitive, while resistant E. coli did not become penicillin sensitive Some antibiotics target things inside bacteria, while others target the wall that surrounds them. From the data that exists, DMSO appears to increase the potency of antibiotics that target the inside of cells (presumably because it transports it into the cells), whereas it does not improve those that target the outside of cells like penicillin. Specifically, a 2002 study of bacteria from lung infections found DMSO potentiated kanamycin, amikacin, streptomycin, and chloramphenicol, but did not potentiate a variety of cell wall targeting antibiotics. Note: the one study potentially refuting this hypothesis was a study which found that DMSO with ectericide and oxacillin (a cell wall targeting antibiotic) was able to significantly accelerate the healing of a dry socket (an unhealed wound following a dental extraction). DMSO has specifically been shown to potentiate: •Streptomycin in resistant E. coli (lowering the inhibitory dose [MIC] from over 5000 µg/ml to 7.5 µg/ml) and in treating gingival (gum) infections.1,2 •Gentamicin, ciprofloxacin, or norfloxacin in pseudomonas aeruginosa, doubling the potency (and having a much greater potentiation for resistant strains). •DMSO significantly improves inflammation in teeth pulp (pulpitis), and this response rate was improved with the addition of oxyphenylbutazone (a drug for gout) or chloramphenicol, going from 75% to 85% (which was also corroborated by another study). •Iodopiron eliminates pseudomonas (resistant bacteria frequently found in burn patients), which was demonstrated by electron microscope observations). •Antimicrobial photodynamic therapy in third-degree burn wounds a day after they had been infected with Staph aureus, resulting in a 98% elimination of the bacteria (whereas without DMSO there was only a marginal dose-dependent reduction of the bacteria). •Isopropanol (an antiseptic alcohol), making it 10-100 times as potent (and sometimes even more, particularly with higher DMSO doses) against many common microbes. Cell studies have also repeatedly shown that DMSO makes resistant tuberculosis susceptible to the common antibiotics. For example: •A 1995 study found DMSO combined with a tuberculosis antibiotic (which was washed away prior to applying other antibiotics) made multidrug-resistant tuberculosis (both in test tubes and within macrophages) much more susceptible to other tuberculosis antibiotics (isoniazid, rifampicin, and streptomycin). Specifically, non-lethal doses of ethambutol and 2-5% DMSO caused a 4-64 fold increase in the sensitivity to other antibiotics (4-16X for rifampicin, 16-33X for streptomycin, and 4-16X for isoniazid), while isoniazid and 2.5% DMSO caused an eight fold increase in susceptibility to other tuberculosis medications. •A 1976 study took cultures from tuberculosis patients and found that 5% DMSO made 19 of the 61 isoniazid resistant strains become susceptible to isoniazid and 19 of the 19 rifampin resistant strains susceptible to rifampin. •Pretreating tuberculosis bacteria in 5% DMSO made them 200 times more sensitive to streptomycin. •A 1974 study of guinea pigs infected with isoniazid resistant tuberculosis found that while all guinea pigs treated only with isoniazid died within 80 days (with tuberculosis throughout their tissues), if a single oral dose of DMSO was given 2 weeks prior to isoniazid, they all survived (and a year later were still alive). Likewise, a 2008 study on hamsters found that DMSO enhanced isoniazid’s ability to treat tuberculosis. Note: DMSO has also been shown to prevent rifampin from degrading for at least 8 months, which suggests it will not disrupt the antibiotic’s potency if administered concurrently. DMSO being combined with antibiotics has made it possible to treat a variety of fairly severe infections: •A 1969 study of 32 patients with destructive pulmonary tuberculosis and endobronchial tuberculosis found nebulized streptomycin and penicillin mixed in 10% or 25% DMSO significantly improved their infection. •A 1991 study found nebulized DMSO mixed with rifampin over 1-2 months was an effective treatment for 148 pulmonary tuberculosis and 18 obstructive bronchitis patients that it could be used alone or to enhance the efficacy of conventional therapies and that DMSO significantly reduced the chronic liver toxicity of rifampin. •A 1982 study tested 27 antibiotic resistant isolates of mycobacterium avium-intracellulare and found that 2.5% DMSO made each antibiotic (rifampin, streptomycin, ethambutol, and isoniazid) affect 26-30% more cultures, in turn leading to every culture becoming susceptible to at least one antibiotic. •A 1994 study of 287 children with either infectious abscesses or regionally inflamed lymph nodes (a tuberculosis vaccine complication) found that applying a DMSO rifampin mixture to those lesions halved their recovery time, reduced the number of isoniazid injections they needed and eliminated the need for other antibiotic therapies. •A 1975 study used a mouth and throat DMSO spray containing y-ketophenylbutazone (an NSAID), moroxydine (an antiviral), hydrocortisone (a steroid), lidocaine, n-propylcarbinol, and 1-butanol (which has antibacterial properties). It was given to 30 fairly-ill infants (most of whom were 1-6 months old) with respiratory diseases (concurrently receiving ampicillin) until they recovered. It caused a rapid clinical improvement and greatly reduced their hospital stay. Note: a reader reported their English bulldog had a very stubborn case of pneumonia, eight weeks of three different antibiotics over an eight week period it did not improve, but after a week of DMSO being used as well, it was fully cured. •In 2020, a Libyan hospital reported giving 16.67% DMSO and 2.78% ceftriaxone (diluted in saline) via a chest tube or endotracheal cannula to 31 lung abscesses, all of which had a complete recovery and no recurrence. •A 1982 study of 42 severely ill patients who had septic complications of post-resuscitation disease, IV DMSO was an effective therapy, even in cases where sepsis came from antibiotic resistant bacteria. Likewise, a 1984 study reported that DMSO was quite useful for critically ill patients with a variety of septic infections and one author cited a case of a septic patient with a severe bladder infection who did not respond to antibiotics but recovered once he began taking one teaspoon of DMSO three times a day. • A 1974 study used DMSO and antibiotics to treat peritonitis (inflammation of the abdominal lining). A 2011 dog study found that DMSO greatly enhanced the ability of antibiotics to treat peritonitis and improve survival rates. A 1975 study also used this combination to treat abdominal cavity abscesses. A 1981 study
then found that injecting DMSO mixed with kanamycin into the peritoneum
concentrated it there, increasing its concentration 3-8 times and
delaying its diffusion into the rest of the body, so that it was
retained 10-13 hours longer (particularly in animals with peritonitis). DMSO combination therapies can also be beneficial for treating persistent infections in the head. For example, in 1967 an Ear, Nose and Throat (ENT) doctor reported that DMSO alone would significantly reduce ENT infections for 2-4 hours (including severe or antibiotic resistant ones), but once combined with DMSO, dramatic improvements would occur (e.g., the eardrum of an otitis media patient would begin shrinking in 10-15 minutes and he had rapid responses to traumatic hematomas of the ear drum and nasal septum).
•A 1968 trial of 25 patients (by this author) showed rhinoscleroma (a rare chronic bacterial infection of the upper respiratory tract) had an excellent response to DMSO plus antibiotics and prednisolone. •A 1992 study found administering 10% DMSO to the sinuses, followed by local oxygenation, caused 49 out of 52 children with acute sinusitis to have a complete recovery. In contrast, many controls receiving standard treatments did not. Note: as the previous studies show (along with many others which have been conducted) DMSO often produces dramatic improvement for a variety of issues in the ears, sinuses, nose and throat (e.g., flus, tinnitus, hearing loss, otitis media, otitis externa, nasal polyps sinusitis, pollen allergies). While DMSO alone can help alleviate these conditions (e.g., tinnitus), they often respond more effectively to combination DMSO drops. •A 2011 study found that DMSO mixed with therapeutic enzymes could treat infertility in men with chronic bacterial prostatitis. Note: a DMSO doctor I’ve corresponded with successfully cured 44 out of 45 cases of microbiologically confirmed chronic bacterial prostatitis (that were likely antibiotic resistant) using DMSO combined with antibiotics that were applied directly into the bladder. •A 2014 study of 48 hospitalized patients with purulent wounds found DMSO greatly enhanced the ability of antiseptics, particularly isopropyl alcohol to eliminate biofilms in them and made the wounds take 6 days less to fully heal. Another 2014 study of wounds also found that DMSO disrupted biofilms and reduced bacterial adhesion to them. A 2013 study also found that it reduced S. Aureus adhesion. Finally, a 2017 study isolated 20 strains of staph (including S. Aureus) and found DMSO significantly reduced their biofilm formation and adhesive activity. •Numerous studies have also shown that DMSO when mixed with antimicrobial compounds (e.g., azathioprine, ethonium), helps gum infections.1,2 Additionally, a herbal extract and the NSAIDs diclofenac and indomethacin have also been used in combination with DMSO to treat peridontitis.1,2,3 •A 2010 Russian animal study found that a gel with 10% glucosamine hydrochloride, 5% DMSO, nettle juice, and kalanchoe juice reduces inflammation and promotes tissue regeneration, suggesting its potential for treating periodontitis. •A 1987 study used DMSO combined with a nuclease to treat meningitis or meningoencephalitis caused by an acute viral respiratory infection. •A 1984 study found that DMSO plus antibiotics prevent open wounds in the hands from developing purulent infections •Lastly, in plants (peach trees) combining 2% DMSO with oxytetracycline was found to significantly increase their resistance to bacterial spotting without injuring the plants, with most of the DMSO leaving the peach trees within a week. Note: DMSO, especially at high concentrations inhibits bacterial growth, so for this reason, if a DMSO mixture is intended for an application where the potential for introducing infection exists (e.g., in a punctured ear drum, fistulas, wounds, infected bladders, infected sinuses) DMSO mixtures that are made by users (rather than sterile preparations that are purchased) should either have a high DMSO concentration or be prepared shortly before use and not stored for a prolonged period. Additionally, clean DMSO, if not exposed to UV light (which is why it’s often sold in amber bottles) will last for a long time (e.g., ancient bottles of DMSO have been reported to work). Fungal InfectionsDMSO has shown promise in treating challenging fungal infections, and there are numerous cases of severe fungal infections which did not respond to conventional therapies (e.g, hence requiring an amputation) that responded to the antifungals being dissolved in DMSO (e.g., see this 1969 case report and others I complied in this article). Note: one DMSO antifungal formulation (Fungizyl AC or Fungizyl AL) was sold in the United States but has since been discontinued. Another (Onychofissan) made by GlaxoSmithKline was designed for nail fungal infections. In parallel, DMSO was shown to significantly increase the dissemination of antifungals. For example: •One study found DMSO increased the amount of ketoconazole that entered the brain, which is useful in fungal infections of the central nervous system, as there are fairly few antifungals that can pass through the blood-brain barrier. •A 1991 guinea pig study found that applying ultrasound to topical amphotericin B (a powerful antifungal) increased its penetration into the skin, but a larger effect was seen when DMSO was applied to the skin prior to amphotericin B being applied (without ultrasound). •Griseofulvin is an antifungal that is primarily taken orally because it has poor absorption through the skin, but once mixed with DMSO, it can be applied topically. Studies highlighting the synergy of DMSO and antifungals include: •A 1965 study
found that 90% DMSO with 2% thiabendazole (an antiparasitic with
antifungal activity) over two weeks had an excellent response in all 16
patients, with 13 having a complete elimination of the fungus. •While neither was effective alone, in two 1966 cases, DMSO when combined with thiabendazole was found to treat tinea nigra palmaris. •A 1968 German study demonstrated that increasing concentrations of DMSO have a greater inhibitory effect on fungal colonies from a variety of species (as they become progressively smaller).
Then, once DMSO was combined with griseofulvin, the inhibition was significantly greater than that seen from DMSO or griseofulvin alone.
•A 1971 study
found DMSO mixed with griseofulvin transported active griseofulvin
through the unbroken skin of guinea pigs and appeared to treat ringworm
infections. Following this, 11 cats with (often severe) ringworm
infections were given either DMSO (which did nothing), oral griseofulvin
(which cured them in 21-42 days) or when the two were combined, cured
them in 5-10 days (typically under a week). •A 1979 animal study found DMSO combined with Griseofulvin was an effective treatment for ringworm, as did a 1974 case report where this combination treated a human ringworm infection. •A 1966 study found that combining 0.5g of bromosulfonylurea and 0.5g of iodochlorohydroxyquinoline with DMSO treated chronic paronychia (inflammation around a nail) caused by Candida, other fungi, pyogenic cocci, and E. coli. Since very small doses were required (1 drop per nail bed, administered multiple times daily), there was also a minimal toxicity risk. In a 1972 trial of 38 patients, a topical solution containing 2% triamcinolone acetonide, 0.05% benzalkonium chloride, 2% salicylic acid, and dimethyl sulfoxide was found to be an effective treatment for bacterial and fungal nail infections. •A 1997 study gave 30% topical DMSO ointment mixed with 1% itraconazole (an anti-fungal) to 9 horses with fungal infections of their corneas (one of whom had 2 affected eyes) every 4 hours, with 8 of the 10 eyes recovering, with treatment lasting between 16 to 53 days (on average 34.6).
•A 1966 study found DMSO increased the potency of two commonly used fungicides for lawn grass by 30%. Note: a variety of agricultural applications exist for DMSO (as it allows the agrochemicals to enter plants and to more effectively eliminate pests). Other Infections•Two different 1966 studies (this study and this 25 person RCT) found that DMSO plus an anti-parasitic (e.g., 2% topical thiabendazole in 90% DMSO) was an effective treatment for hookworm infections in the skin. This was followed by a 1972 case report in a woman who was given DMSO on one affected knee and DMSO plus thiabendazole on the other in a blinded fashion. The knee that received the combination rapidly recovered from hookworm, while the DMSO only knee got worse and then recovered once it also received the combination. •In patients with echinococcosis (a tapeworm), large cysts can form in the liver. A 2014 study found that when surgically removing them, applying a mixture of DMSO, glycerol, and albendazole to the cavity prevented the spread or recurrence of the infection. • A 1967 study treated 9 cats with feline panleukopenia, a virus that has a high mortality rate (e.g., over 90% in kittens) and is therefore one of the primary cat vaccines. Those cats were treated with 4ml injections of 90% DMSO alongside vitamins, antibiotics, and IV fluids. There was a rapid improvement in the cats, with two-thirds surviving (60% of those less than six months old and 75% of those over six months). In contrast, after 12 subsequent cats were treated with only the standard of care, all died. Chemotherapy CombinationsIn the same manner that DMSO enhances the ability of antimicrobials to reach pathogens, it also does the same for chemotherapy while simultaneously reducing its toxicity (e.g., lower doses can be used, particularly for hard to reach tumors like brain cancers). Furthermore, DMSO appears to concentrate in cancers (e.g., one study found a 1.5-fold concentration of it in brain tumors, which was clearly demonstrated with the DMSO-hematoxylin mixture). Many studies, in turn, have shown that DMSO increases the potency of cancer drugs. For example: •A 1975 study of 65 patients with incurable cancers (most of which had received conventional therapies) found a low dose of cyclophosphamide mixed in DMSO with GABA, GABOB, and acetylglutamine cured 57 of them. •A 1975 rat study found that oral DMSO increased the potency of cyclophosphamide and increased the survival times in advanced cancers by potentiating many common chemotherapy drugs. •A 1987 study of patients with cervical cancer found that applying metronidazole dissolved in DMSO to the cervix increased the tumor’s regression following radiation therapy. •Two 1988 studies1,2 found DMSO generally increased the potency of five different common chemotherapies; however, the potentiation varied depending on the cancer, dose of each, and chemotherapy drug used, and in a few cases it instead reduced the potency. •A 1992 study of rats with bladder cancer found that DMSO caused 7.1-12.1 dose dependent increase in doxorubicin in the bladder and lymph nodes, greatly reducing the amount of chemotherapy needed to treat the cancer (e.g., mixing it in 5% reduced the amount needed by 44%). •A 2021 study of 52 patients with surgically removed bladder cancer found that adding DMSO to a chemotherapy regimen reduced their relapse rate by approximately 50%. •A 1983 study found DMSO neutralized an impermeable barrier cancer cells had around them and made cytoskeleton targeting drugs more potent (e.g., making 1/30th to 1/1000th of their usual dose be needed). •A 2022 study found that 1% DMSO significantly altered the cytoskeleton of melanoma cells (e.g., how they attached to their extracellular surroundings) but not normal cells, and that when DMSO was combined with CaS (which releases ions that can trigger programmed cell death), there was no noticeable effect on the skeleton of normal cells, but there was heavy disruption to the cytoskeleton of cancerous cells. Many other studies have also been conducted on DMSO’s effect with common chemotherapy agents (e.g., cisplatin), most of which found it increased their potency and often reduced their toxicity (all of which can be read here). Additionally four studies between 1995 to 2009 found DMSO roughly doubled the efficacy of photodynamic therapy for basal and squamous cell cancers.1,2,3,4 Note: while most sources say DMSO works well with chemotherapy, one more modern research stated that concurrent administration can increase the toxicity of chemotherapy drugs and lower doses needed to be used to avoid side effects (which may be due to newer chemotherapy drugs existing now that did not exist at the time most of the DMSO research was conducted). Additionally, for conventional chemotherapy agents, nurses who prepare and administer them (e.g., via vapor inhalation) have found been found to at an elevated risks for a variety of diseases (including cancers) so it is crucial to be extremely cautious when administering it with chemotherapy drugs (particularly when applying it topically). Lastly, many have started exploring the ivermectin and fenbendazole protocols, which we have found sometimes produce dramatic results but are typically insufficient to treat cancers, and for which certain individuals have difficulty (e.g., due to visual toxicity from the higher doses of ivermectin that are frequently suggested). One doctor shared with me that topical DMSO-ivermectin treated a metastatic colon cancer, appeared to have a good response in 5 prostate, 1 breast, and 1 ovarian cancer that had not metastasized, and may have helped a brain cancer (but for those 8 cases, conclusive data is still being awaited). Additionally, 30 or so other patients were recommended the protocol, but no followup was possible with them (due to his practice being both in person and a Telehealth, and those 30 being Telehealth rather than in person patients), so it is not known if they did the protocol or it worked for them. I find this report noteworthy, as it reports a much higher success rate than I have typically seen with ivermectin, suggesting that DMSO effectively potentiates the therapy while simultaneously using doses that avoid ivermectin’s visual toxicity. Note: guidance for preparing a DMSO ivermectin paste can be found later in the article. In parallel, one reader shared that DMSO and ivermectin cured their skin cancer, while another cured a squamous cell carcinoma with ivermectin, fenbendazole, and DMSO. Likewise, a reader shared that adding DMSO to their IVM/FenBen protocol caused their cancer markers to rapidly drop and their tumor to shrink, while another shared it allowed them to reduce the dose of the drugs to doses they could tolerate, and a third shared that DMSO and ivermectin cured their cancer. Note: part of the potentiation of ivermectin is likely due to it bypassing the liver (which due to the first pass effect metabolizes about half of the ivermectin you ingest) because much greater concentrations can be achieved by applying it to the target area (rather than having to achieve that concentration throughout the body with a much higher dose), it allowing ivermectin to penetrate into the tumor, and DMSO's broad anticancer properties, many of which align with or enhance ivermectin's mechanisms (e.g., they both inhibiting proliferation via overlapping pathways induce apoptosis, enhance immune targeting of cancers, and reduce resistance to chemotherapy). Other CombinationsMany other applications of DMSO have been studied, and as recently as 2019, a few pharmaceutical patents have been filed for DMSO delivery systems (which are instructive to read for anyone wanting a more detailed understanding of the subject). One was for enhancing the tissue penetration of steroids, another for a DMSO tetracycline antibiotic foam combination used to treat acne and one for the parenteral injection of peptide drugs. Note: DMSO is difficult to sterilize with conventional methods (as it will react), so the accepted method of sterilization is to run it through 0.22 μm filters with DMSO compatible housings. In cases where DMSO is mixed with a polymer (which can’t pass through the filter), each component is purified separately and then compounded together. A few of these assorted DMSO combinations include: •DMSO combined with Perftoran (a tissue oxygenating agent), when injected into the joint space was found to treat bone marrow swelling of the femoral head. •Finally, 1998 and 2000 cow studies found that if experimentally induced aseptic arthritis and then treated each day with DMSO, if on days 2 and 7, the joint was injected with healthy synovial fluid from the same cow, recovery was enhanced. •A study found that 1% hexopyrronium bromide (an antiperspirant) in 90% DMSO was of value in the treatment of dyshidrosis (blistering eczema) and hyperhidrosis (excessive sweating). A sheep study found DMSO was superior to carbocetin (an oxytocin analog) at opening the cervix (which is needed for artificial insemination to succeed), and that when both were given together, a better effect was seen than with DMSO alone. Note: many more assorted pharmaceutical combinations exist that I did not cover here. Enhancing DMSO CombinationsInspired by the extensive body of research demonstrating the value of combination DMSO therapies, many have independently experimented with them to identify the most beneficial options. Unfortunately, there are so many options that it can be quite difficult to know where to start. For
instance, in most cases, rather than pure DMSO being used, it is
diluted in something. While water (ideally purified water) is typically
the most popular choice (and what I’ve broached so far), DMSO users tend
to overlook the fact that many other options also exist, which can
frequently enhance the potency of a DMSO treatment. For example, magnesium is one of the most important elements for the body, and simultaneously one of the ones in which we are most deficient. Since magnesium causes muscles to relax, assists in mitochondrial energy production and tissue regeneration, and already partially absorbs through the skin (e.g., topical magnesium oil is often used for pain from tight muscles), it has been a popular substance to dilute DMSO in (provided the correct dilutions are used). In
turn, when added to DMSO, magnesium amplifies many of DMSO’s injury
healing and pain reducing qualities. As such, DMSO magnesium
combinations (topically or orally) are frequently used for inflammation,
pain, scars (including small ones on the face), injuries (particularly
sports injuries), hair loss along with many other conditions (e.g.,
baker’s cysts or tendonitis), with many reporting rapid improvements and
relief not seen with DMSO alone. Healing the EyesIn the early days of DMSO research, Merck discovered that high doses of DMSO could alter the refractive index of dogs (which essentially made them require glasses). Needing a reason to outlaw DMSO, the FDA amplified this and before long convinced many that DMSO could make you could go blind and that DMSO trials could only be approved under the strictest of situations where participants eyes were continuously monitored (which made the trials financially prohibitive to conduct). Subsequent research showed this effect was temporary, did not affect any other animal besides rabbits (e.g., monkeys were unaffected) and it was never seen in human studies. Nonetheless, this mythology persisted, even when an exhaustive human toxicology study using massive doses failed to detect any effect. This was quite ironic as one of the first “side effects” observed from DMSO (e.g., when taken topically for musculoskeletal issues) was a significant improvement in vision. This led to a series of studies (detailed here) that showed DMSO did even more when applied directly to the eyes and treated a variety of challenging or incurable eye diseases (e.g., macular degeneration, cataracts, glaucoma, inflammation throughout the eye, episcleritis, corneal edema, retinitis pigmentosa, corneal burns) along with case reports of even more dramatic improvement (e.g., years of lost sight being restored). Since
that time, the DMSO community (and certain German ophthalmologists)
have extensively explored using DMSO for eye conditions and essentially
found that most eye diseases can be treated or improved with certain
DMSO eye drop formulations. These include: In parallel, many have also found that circulation, oxygenation, and in the eyes greatly improve and the eyes “rehydrate,” and their muscle tension dissipates. DMSO hence has allowed many to reduce eye strain (e.g., from screens) , restore gradually declining vision and reduce their need for glasses. Because of this, many with early eye issues that have not yet become a disease now take DMSO to preserve the health and longevity of their eyes. Note: when DMSO eye drops are used, it is generally advised to avoid using them within 2 hours of eye medications to avoid potentiating the medications. Local Anesthetic CombinationsOne of the most promising DMSO combinations arises with local anesthetics. Local anesthetics (unless injected into the bloodstream) typically only affect (numb) the area where they are injected. However, once combined with the transporting agent DMSO, both their potency and range in the body broaden (e.g., procaine has been shown to rapidly penetrate through the skin when mixed with DMSO). For example, a 1967 study found that when DMSO was mixed with tetracaine (a potent local anesthetic), using at least 5% tetracaine resulted in 4-6 hours of prolonged anesthesia, with faster onsets occurring as higher percentages of DMSO were used as the vehicle. Additionally, 20% procaine (rather than tetracaine) was not sufficient to produce pinprick anesthesia, the anesthetic effect was only near the surface, and tetracaine was not observed to enter systemic circulation. Later, another study by the same author found that local anesthetics (e.g., tetracaine and procaine) could produce prolonged (and reversible) nerve blocks and pain control in animals, lasting up to five days without adverse effects. DMSO has also been shown to potentiate local anesthetics put on the eyes, and when combined with tetracaine, to topically anesthetize the ear drum (thereby bypassing the need for a painful puncture to anesthetize it). Anesthetizing ScarsOne German school of medicine, neural therapy, recognized that scars (e.g., from a C-section, injury, joint replacement, or vaccination) can often create “interference” fields, which continually disrupt the autonomic nervous system and give rise to a wide range of chronic and sometimes debilitating syndromes (e.g., complex regional pain syndrome). In turn, they discovered that if a scar was injected with a local anesthetic, once the anesthetic wore off, the scar would “reset,” stop setting off the nervous system, and resolve a variety of complex issues. As this frequently produced phenomenal results, it became a mainstay in the German integrative community, and gradually was refined to identify which scars were problematic (e.g., by focusing on areas with numbness or “disrupted energy flows”) so less injections needed to be done. I frequently utilize this modality, and it is one of the many ways I can quickly produce “miracle” cures for complex illnesses, as it is seldom recognized by the medical community how problematic scars (particularly surgical ones can be) or how many other issues (e.g., gastrointestinal ones or psychiatric symptoms) will resolve once a toxic scar is treated. Since DMSO to some extent, treats toxic scars too (and restores normal functionality to the scar tissue, such as sensation, sweat production, and hair growth) and can bring anesthetics into the body and spread through the tissue, the German DMSO community gradually started mixing it with their preferred local anesthetic. They quickly discovered that this combination not only treats many scars but also enhances other DMSO’s curative properties. In cases where DMSO can’t treat a specific issue (it frequently helps), the combination does. Note: frequently, after DMSO treats a scar, individuals report an unimaginable sense of lightness within them or a softening of deep, hardening throughout their body that they had become accustomed to. Many individuals in turn, have reported remarkable success using a topical or injected DMSO mixture to treat a wide range of conditions, including: •Tissue adhesions (with DMSO combination injections followed by manual therapy). Note: most of my experience with neural therapies comes from direct injections of scars. The DMSO community reports they find topical applications allow them to eliminate about half of the otherwise painful injections they need to do. Likewise, many in the DMSO community advocate for simply treating every scar on your body with this mixture as they often observe profound improvements from the correct scar being treated (which is often one that individuals do not even recognize they have). Unfortunately, very little formal research has been conducted on this approach, and the only study I could locate was a 1988 investigation
of adolescent patients that found DMSO plus procaine to be effective in
treating chronic parenchymatous parotitis (inflammation of the salivary
glands). Lastly, a relatively safe mucus clearing drug (which is sold over the counter in Europe but not approved in America) also happens to have a secondary function as a local anesthetic. The DMSO community in turn, has discovered when it is combined with DMSO, it can treat a wide range of significant pain conditions. Unlocking DMSO's Potential: Practical Applications and ProtocolsThe preceding sections highlight the vast potential of therapeutic DMSO combinations and their practical applications. Remarkably, some of the most effective pharmaceutical DMSO combinations discovered are also the simplest, making them accessible for use at home. In the final part of this article, I explore the best sources for obtaining high-quality DMSO (as the surge in interest has led to the emergence of questionable sources and sellers). I also cover dosing guidelines, common protocols for DMSO applications and preparing therapeutic combinations, and how these principles can be tailored to address challenging conditions, including:
Additionally, I will highlight my favorite DMSO combination, which enabled an extraordinary ability: being able to see in the dark... Continue reading this post for free in the Substack app
|
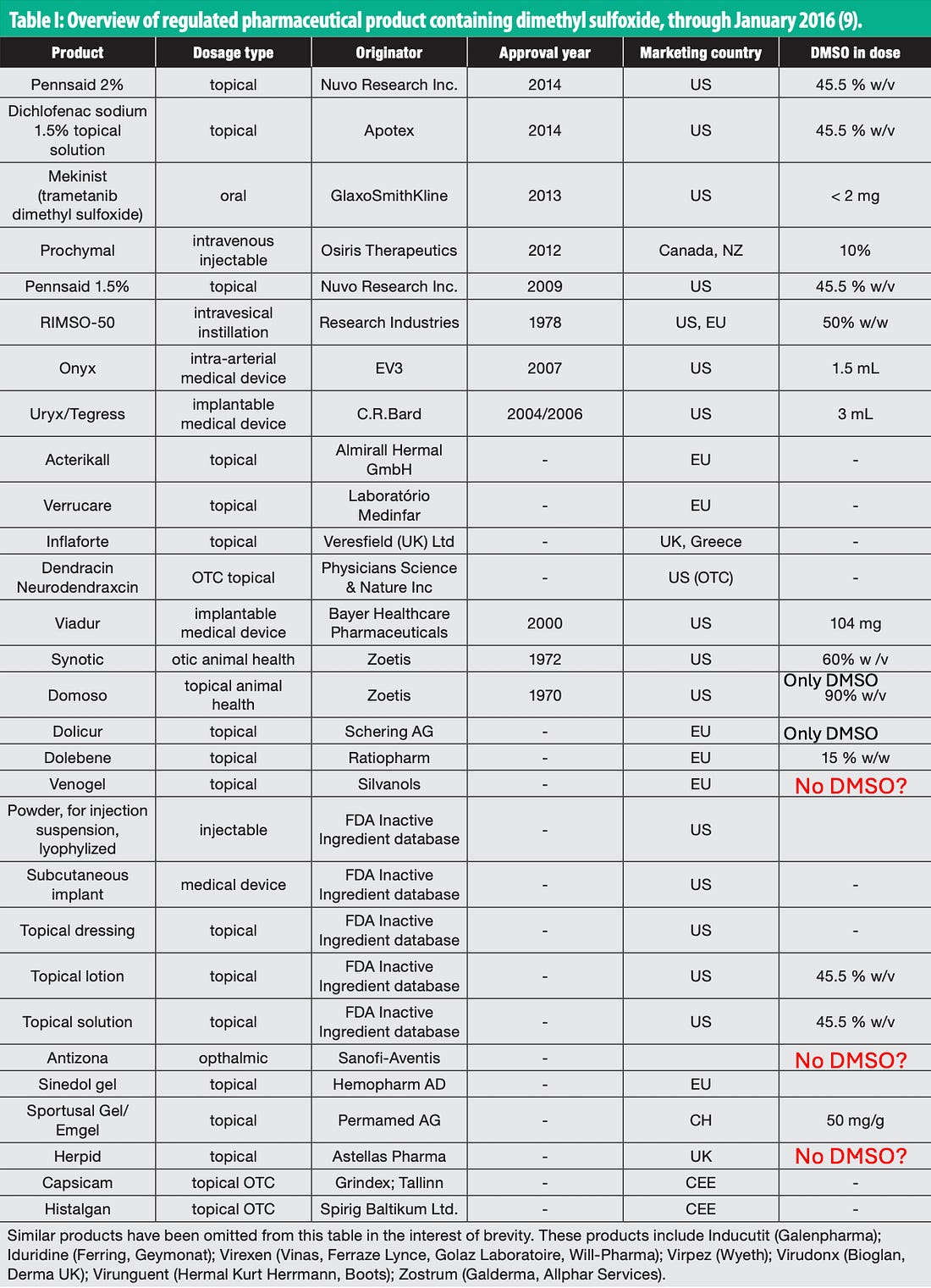
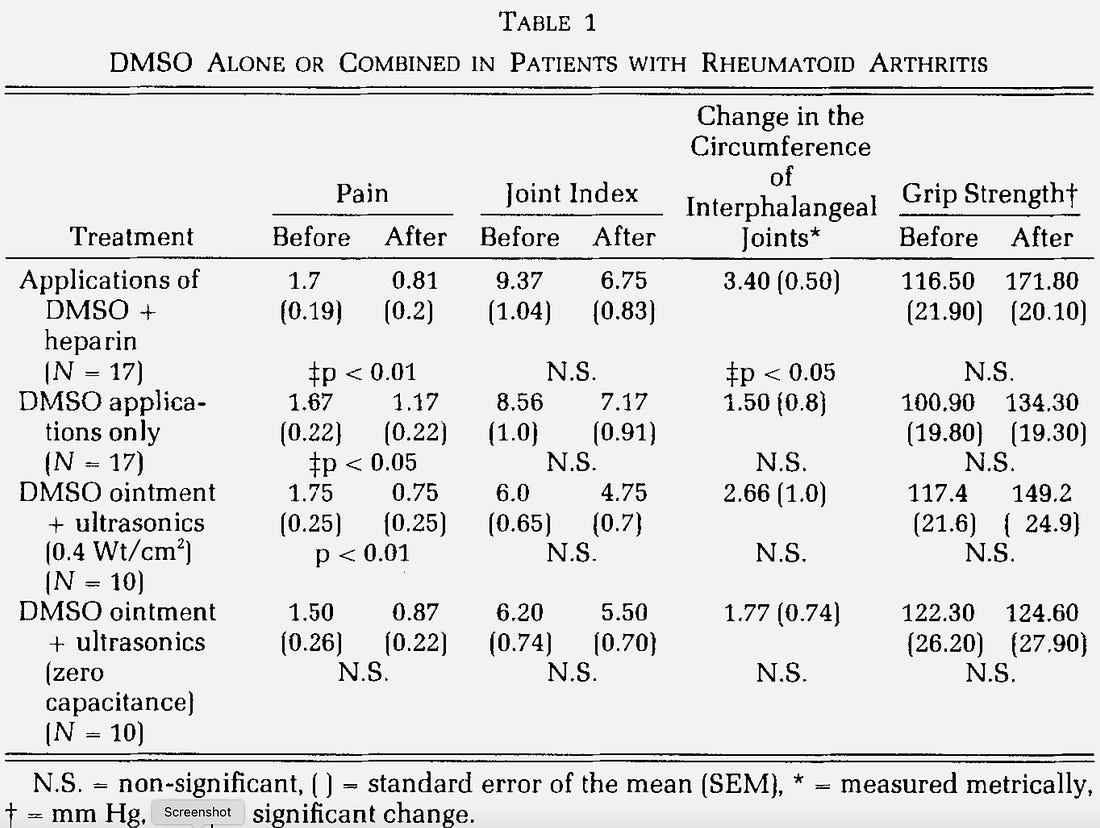
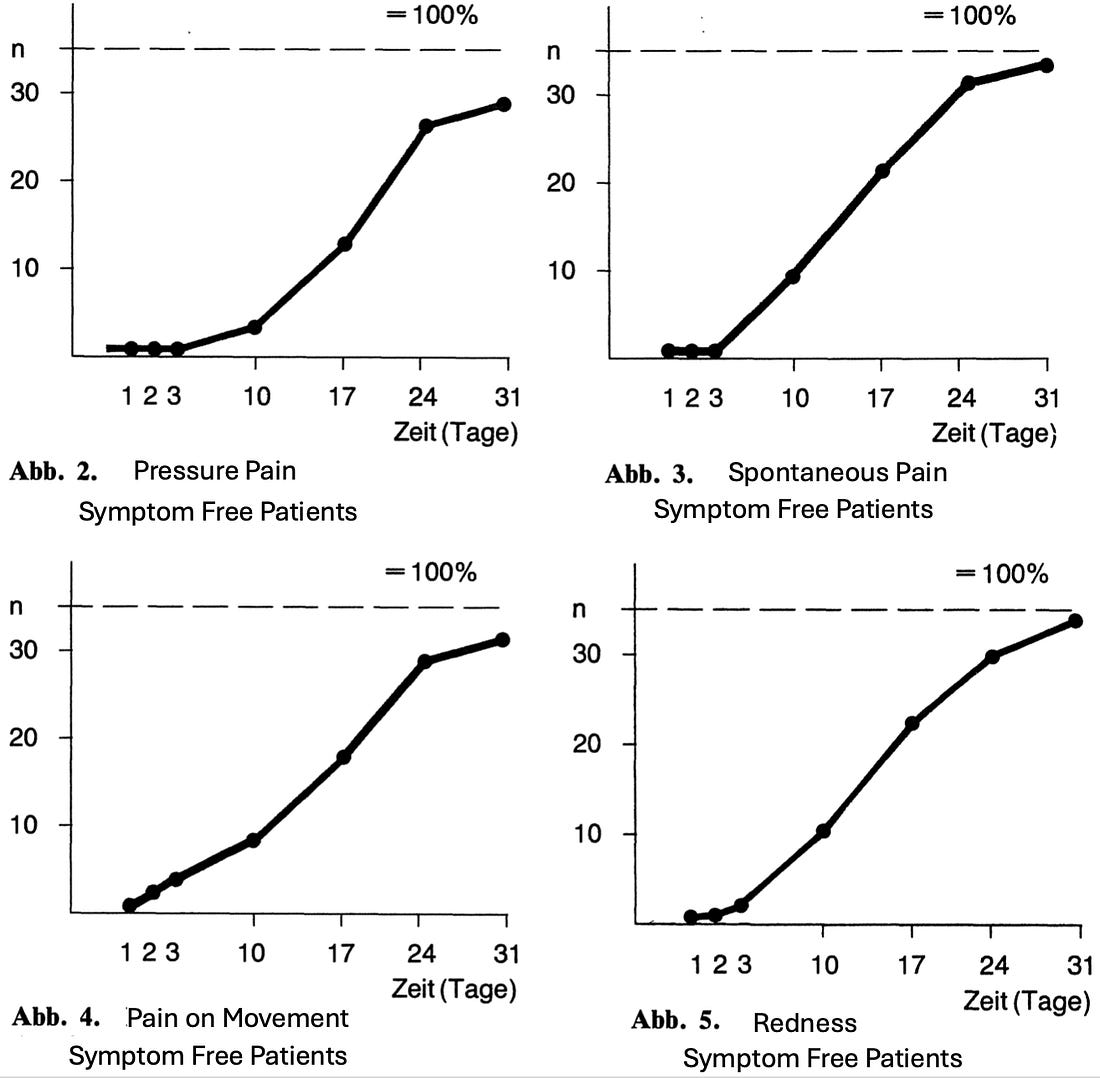
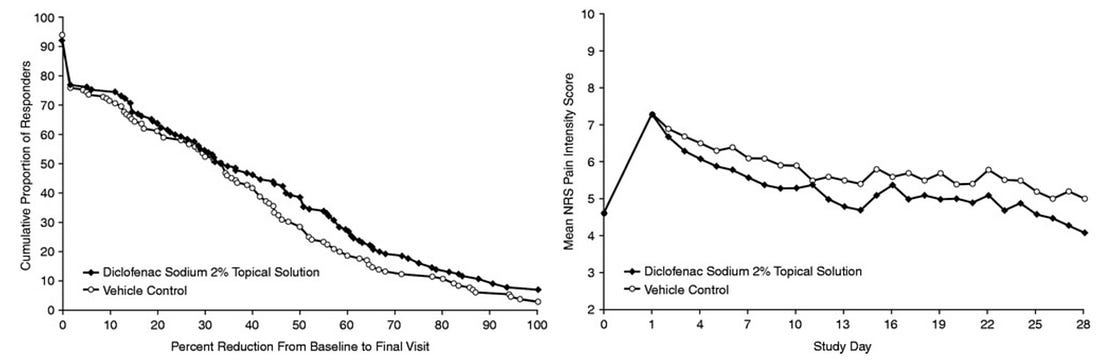
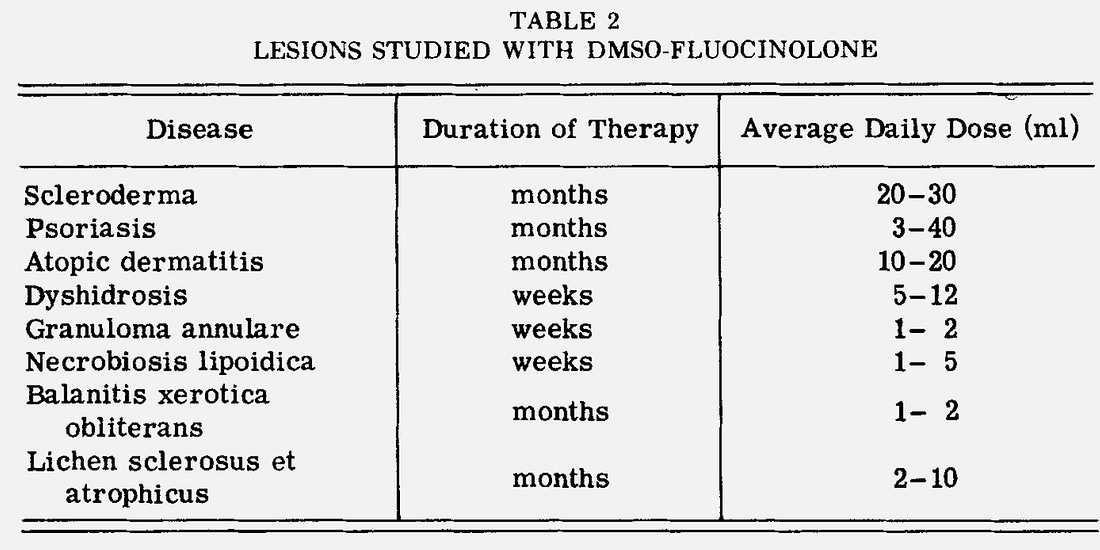
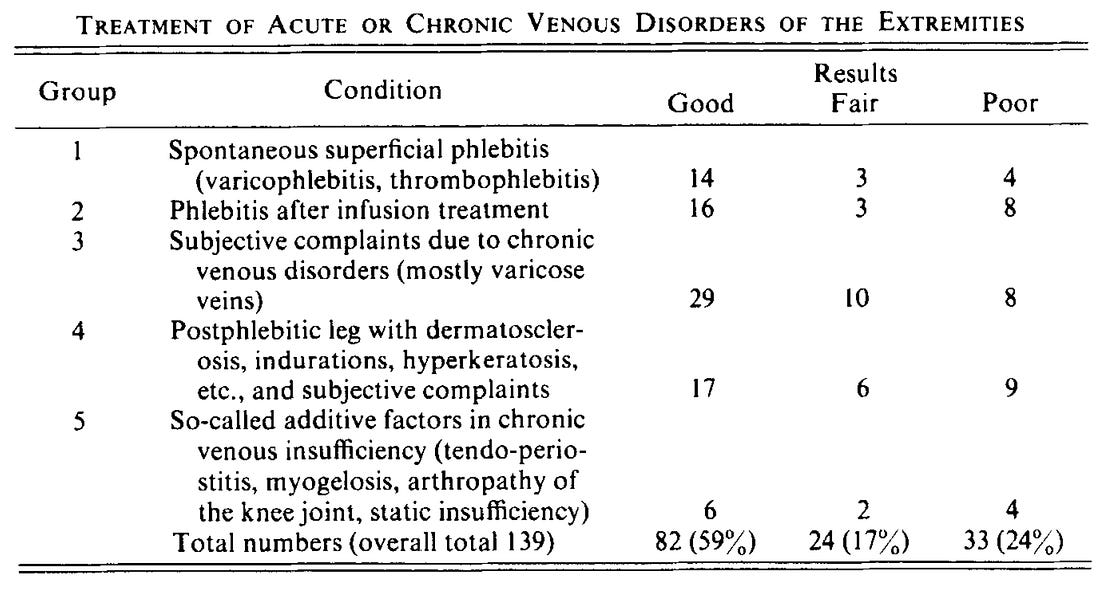
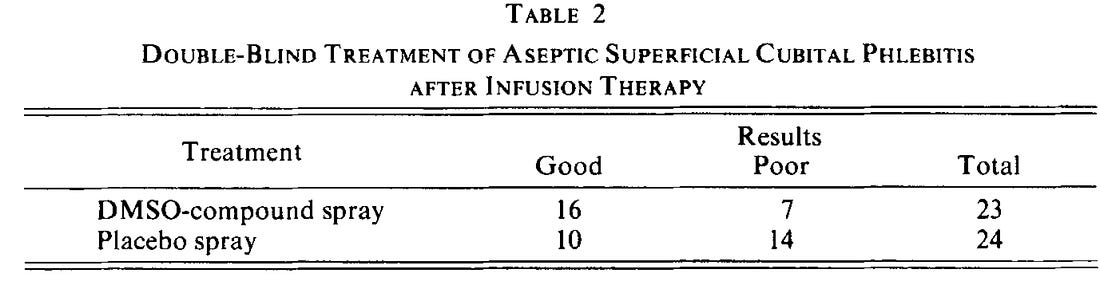
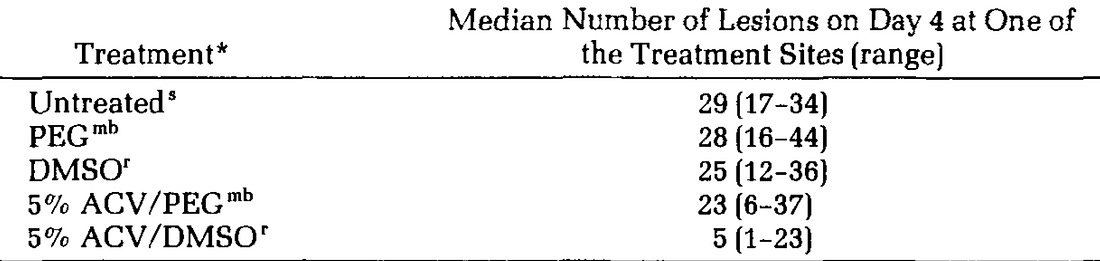
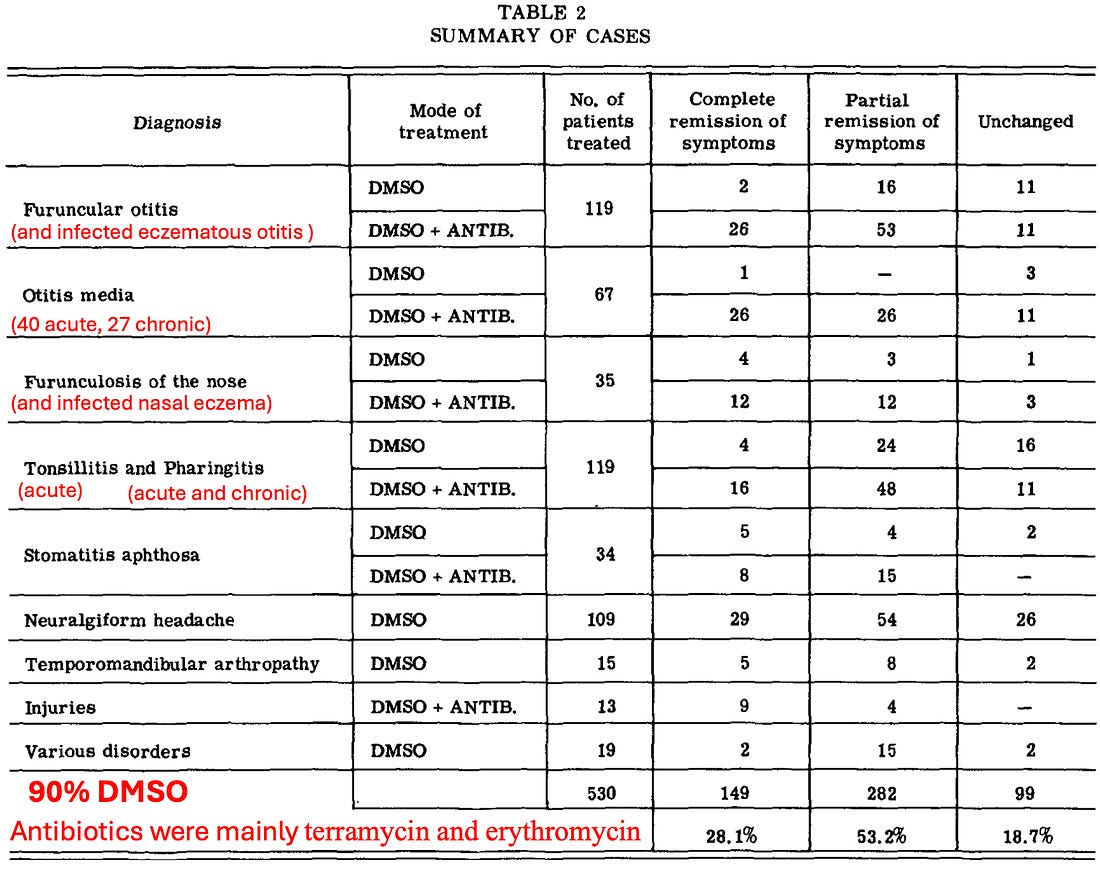
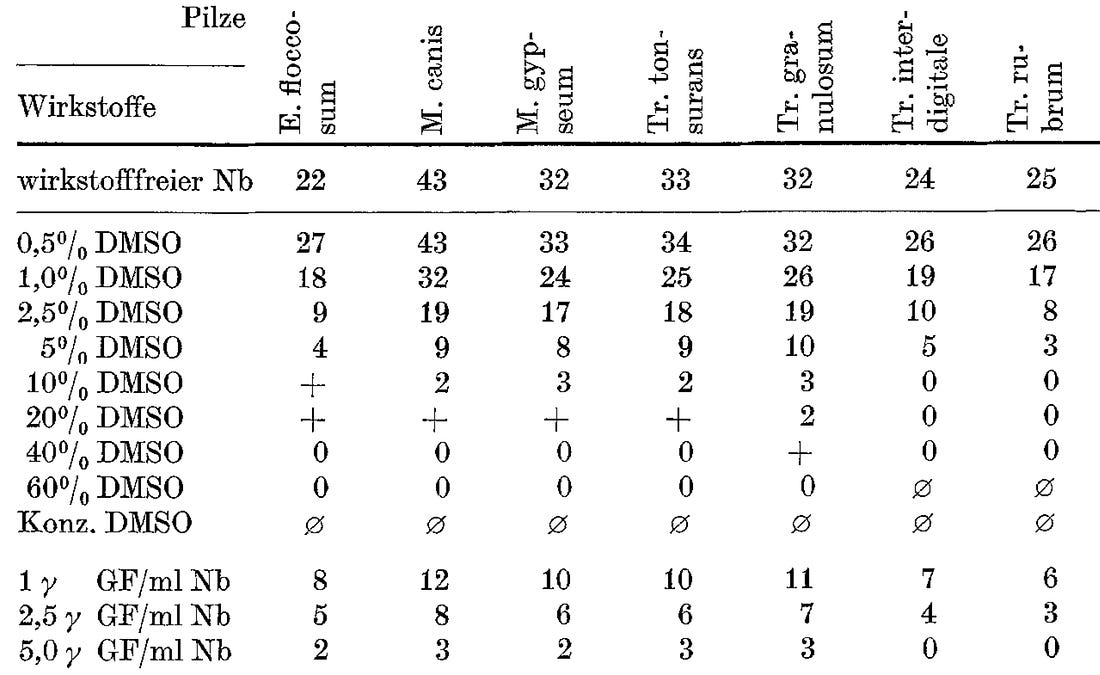
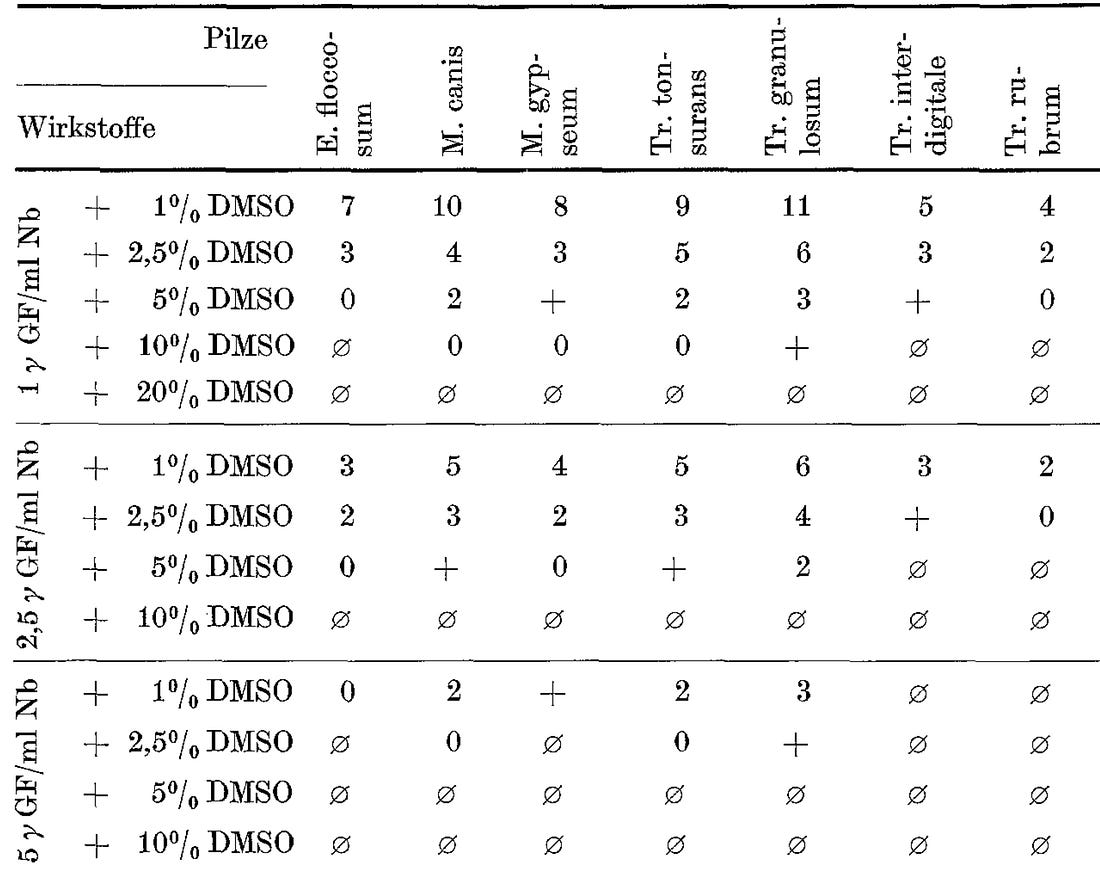

No comments:
Post a Comment