What They Don’t Tell You About AnxietySince anxiety is frequently misdiagnosed the wrong treatment is often chosenStory at a Glance:
Many consider anxiety to be the disease of the modern age. It is thus one of the most significant disease markets in America (e.g., from 2001-2004, approximately 19.1% of American adults had an anxiety disorder and in 2007, 36.8 billion was spent on medical care for anxiety and mood disorders). Yet despite spending billions on anxiety, rather than be appropriately addressed (like many other industries that depend upon the perpetuation of the problem they “solve”), it has only increased.
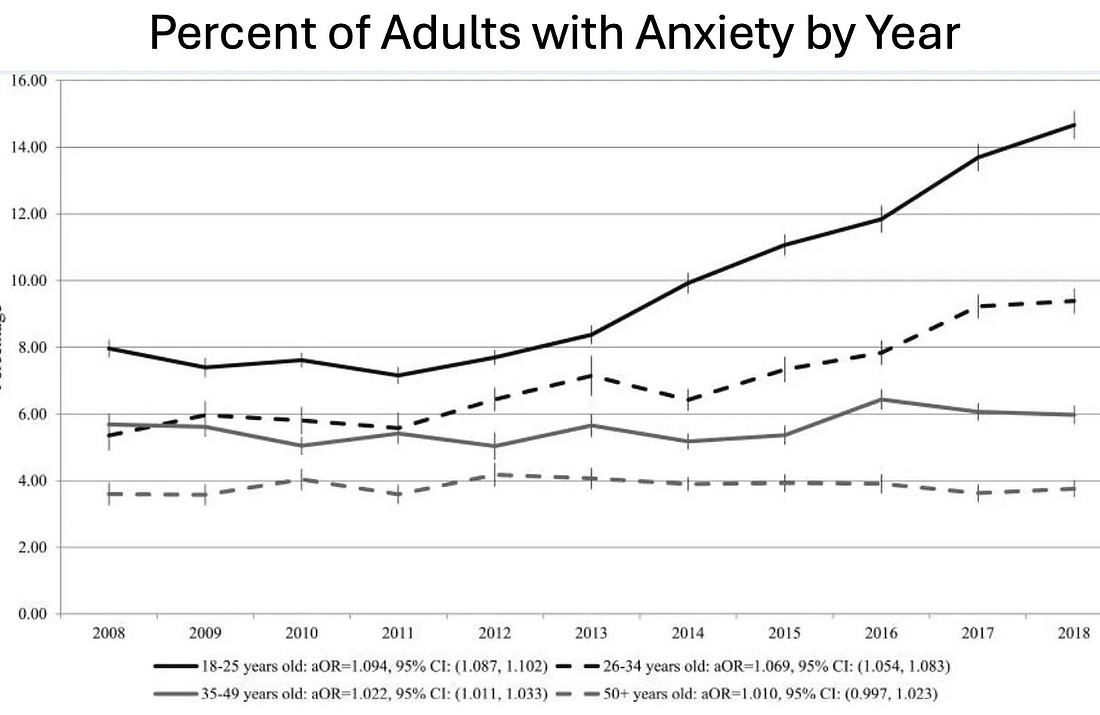
Worse still, a recent survey found slightly over half of young adults (18-26) now suffer from anxiety, 43% have panic attacks, a third take anxiety medications, 54% found they became worse in 2023, and 26% of them were diagnosed with a new mental health condition due to COVID-19.All of this suggests we may not be utilizing the best approach to deal with anxiety—particularly since the drugs used to treat it are some of the most problematic ones on the market. Insufficient Treatment TimeOne of the biggest challenges in psychiatric care is the lack of time spent with patients. This rushed approach leads to some serious issues such as:
Sadly, in today’s healthcare system, unless you work with a holistic cash-pay psychiatrist appointments are typically limited to just 15 minutes, leaving little room for meaningful interaction. Overlapping SyndromesA major challenge in medical diagnosis is that the same disease can create different symptoms in different patients, while completely different diseases can present with fairly similar symptoms. Because of this, it is typically much easier (and profitable) to give therapies that are directed at the symptomatic expressions of disease rather than taking the time to determine exactly what is causing the illness to trigger, and treating the root cause. As such, one of the most common reasons individuals seek out the (often costly) realm of non-insurance covered integrative medicine is due to the fact that the symptomatic management conventional care offers leads to unacceptable outcomes (e.g., many debilitating symptoms remaining, costly and harmful “treatments” needing to be done indefinitely, or the illness progressing). In an article on the depression industry, I highlighted a major problem with the condition—rather than there being one type of depression, numerous different things can cause it. This is often quite consequential, as while some types of depression respond well to SSRI antidepressants, others do not, and some become significantly worse with antidepressant therapy. As such, it is not appropriate to quickly diagnose someone with depression and then prescribe an antidepressant—but this is unfortunately what frequently happens, particularly in 10 minute primary care visits. In turn, the exact same is true for “anxiety” (which helps to explain why “anxiety” and “depression” remain the two most common psychiatric diagnoses). Types of AnxietySome of the most common types of anxiety include:
Understanding these different types of anxiety is crucial for accurate diagnosis and treatment. For example, in many cases, benzodiazepines or SSRIs are not appropriate for the condition (and frequently can make it worse or create a medication dependence), while the appropriate psychotherapy can be quite helpful. However, in practice, we find inappropriate medications are frequently given while psychotherapy (which is often far more beneficial for resolving anxiety) is never offered. This I believe to a large extent results from the prescribing physician not understanding that different types of anxiety require different treatments and it requiring far more resources to provide psychotherapy. Note: it can sometimes initially be difficult to determine what form of anxiety someone has either because they are concealing it or are in denial over the root cause of it or because they have multiple forms existing concurrently. As such, I believe it is important for patients to understand the types of anxiety so they can avoid being misdiagnosed and given the wrong treatment. Causes of AnxietyWith some types of anxiety (e.g., PTSD anxiety), the cause is fairly straightforward. However, it is far more ambiguous for many others and hence often missed by a rushed clinician. Important causes to be aware of include: Mental Causes of AnxietyAnxiety, particularly Generalized Anxiety Disorder (GAD), often stems from anticipating a negative future, being fearful of it, and then getting trapped into an overthinking response. Many things in our society encourage this:
Physiologic Causes of Anxiety.Frequently, while anxiety is treated as a psychiatric illness, there is actually a physical cause of it. These include:
When the physiologic causes of anxiety are addressed, rapid improvements are frequently seen. For instance, I’ve lost count of how many people I’ve met who had rapid and dramatic improvements in their anxiety once the dysfunctional half of their autonomic nervous system was addressed. Metabolic Causes of AnxietyWilliam Walsh analyzed the blood of 2,800 individuals with depression
and discovered there were five common metabolic types of depression
which each have characteristic symptoms. Walsh’s paradigm is quite
useful as: •It explains why patients will often have very positive or negative responses to medications (e.g., SSRIs can be helpful for undermethylators but cause severe reactions for overmethylators). Likewise, it helps predict if patients will have an adverse reaction to supplements or other medications •Anxiety often occurs concurrently with depression in these biotypes and hence can be treated (or fully resolved) by treating the biotype.
Note: the five biotypes of depression are discussed further here. Lifestyle Causes of AnxietyWhen there is too much stagnation in the body (particularly in the head), individuals have a tendency to overthink things. This I believe, explains why: Physical Activity: A meta-analysis found that exercise is 1.5 times more effective than medication or therapy in reducing mild-to-moderate anxiety and depression. Note: we believe daily walking is an ideal exercise for mental health, physical health and longevity. Stagnation and Illnesses: Conditions like COVID-19, vaccine injuries, or cancer can create stagnation, leading to anxiety and depression. Tight Clothing: Tight or synthetic clothes can restrict blood and lymphatic flow, contributing to anxiety. Restricted breathing and the positive charges from synthetic fibers can worsen the issue (which then adversely affects the electrical dispersion with fluids like blood and creates significant fluid stagnation). Improving Stagnation: Many approaches that improve stagnation in the body improve anxiety (e.g., sexual intercourse, hot bathing, and electrical grounding have been found to decrease anxiety). Screen Time: Excessive computer use and blue light can overstimulate the brain, contributing to anxiety. Grounding Traditions: Practices from Chinese medicine suggest that anxiety arises from too much energy in the head, emphasizing the need for grounding (e.g. by walking barefoot on natural surfaces). Collectively, I believe many health issues arise from modern technology, nutritional depletion, circadian disruptions, and fluid stagnation within our bodies, and that beyond this affecting physical health, it also affects emotional and mental health. Because of this, the psychiatric treatments that are utilized to treat anxiety often only have marginal efficacy, as one can often try very hard to stop overthinking things, but nonetheless still do so (if their anxiety has a physiologic cause). Anxiety and BenzodiazepineWhy are Benzodiazepines the medical industrial complex primary treatment for anxiety? Beyond the obvious profit incentives, the high usage results from prescribing doctors simply having too little time with their patients. Unfortunately, there are many issues with this approach. These include: •Benzodiazepines (and SSRIs) tend to work much better for anxious patients who have first received psychotherapy (typically cognitive behavioral therapy—which has repeatedly been shown to be a highly effective treatment for anxiety). Unfortunately, since therapy is resource intensive, this often is not done. In an ideal world, all patients with anxiety would first receive psychotherapy appropriate for their type of anxiety, then if that does not get them well, start them on an appropriate medication (which provided psychotherapy has already been done for, they are likely to have a far more rapid response to that if the medication is given without prior psychotherapy), and then gradually reduce the medication to the minimal dose the patient needs (or completely withdraw it). •Patients are not warned by their doctors as to how addictive the benzodiazepines can be or how hard they are to quit (and had they known many patients would never start them). Likewise, many do not know that using benzodiazepines for as little as 3-6 weeks can create a physical dependence that can give way to a permanent addiction. •Patients are not warned that certain benzodiazepines have a much higher risk of addiction. This is particularly those with a short half-life, especially Xanax, due to the fact it concurrently creates a euphoria when it is taken (and a depression once it wears off). Note: individuals commonly mistake the euphoric effect of a drug with its therapeutic effect. As such, when taking psychiatric medications, the goal of a patient should be to “feel fine” not to “feel good.” Unfortunately, the issues with Xanax are still not sufficiently recognized by the medical field and it remains one of the most commonly prescribed benzodiazepines.
Note: Xanax is also incredibly difficult to withdraw from, to the point it often must first be substituted with another benzodiazepine. •Because benzodiazepine users frequently develop tolerances to these drugs, prescribers frequently use higher benzodiazepine doses than are appropriate and then further increase them as the patient develops a tolerance to the drugs. Conversely, the people I know who have the best results with benzodiazepines use very low doses (e.g., they start with one-half or one-quarter of the recommended dose, monitor the patient’s response to it, and only raise it a bit if needed). •Because patients often are very sensitive to benzodiazepine withdrawals, small changes in the doses can often create significant problems. This frequently arises when generic formulations of the drugs are made (as significant quality control issues exist with many generics produced overseas, and the pharmacologic action of generic benzodiazepines can be surprisingly inconsistent). As such, my colleagues periodically will have patients who were changed to a different brand of an existing prescription that developed significant complications as two brands were not equivalent. In short, benzodiazepines can be very helpful if they are used for a type of anxiety that responds to their action, and they are appropriately used for a short period of time. Unfortunately, they instead tend to be given for a broad swathe of anxieties and then continued indefinitely (particularly in the elderly), at which point their harms greatly outweigh any benefit they can provide (as benzodiazepines have many highly consequential side effects). In many ways, benzodiazepines could be analogized to the “nuclear option” for anxiety. Unfortunately, providers are far too quick to use them rather than first attempting to consider the far safer options available due to their limited time with patients. ConclusionThe situation we see with anxiety and benzodiazepines reflects a sad reality in society. Whenever a group is tasked with solving a problem but is paid for “improving” rather than fixing it, the group cannot be relied upon to solve the problem as their economic and political incentives reward the perpetuation of the problem rather than its resolution. In healthcare, this has resulted in a myriad of chronic illnesses becoming more common as the years go by (and their harmful “treatments” consuming an ever growing share of the national budget). Worse still, the viable and affordable treatments that address the root causes of those illnesses tend to be actively attacked by the medical establishment and frequently kept from seeing the light of day (e.g., consider what we saw throughout COVID-19). Fortunately, recent political winds (e.g., the rise of MAHA in response to COVID-19 and an administration that has prioritized eliminating wasteful spending) have provided a previously unimaginable opportunity to change this dysfunctional paradigm. As such, I am immensely hopeful our relationship to many widespread conditions like anxiety will change in the near future, and I am immensely grateful to each of you who has begun speaking out against our dysfunctional healthcare system so we can at last create a better path forward. Author’s Note: This is an abbreviated version of a full-length article that takes a deeper look into the causes of anxiety, the most natural and conventional treatments for anxiety (including those you can do at home), the immense dangers of benzodiazepines and guidelines for safely withdrawing from them. For the entire read with much more specific details and sources, please click here. You're currently a free subscriber to The Forgotten Side of Medicine. For the full experience, upgrade your subscription.
|

No comments:
Post a Comment