IgG4 Antibody Class Switch: End Of The Line
Tired of COVID? So is your immune system: innate, adaptive and complement are all out to lunch, and you're on your own.

Over the last few weeks, anybody scientifically inclined has been abuzz about the IgG4 class switch that has been observed post-vaccination. I think it’s safe to say this caught absolutely everybody by surprise: neither the mainstream liars nor the resistance seem to have seen this one coming. While there are a lot of brilliant scientists that have accurately predicted a lot of what we would see over time, I can’t think of a single one that saw this particular disaster coming. Please correct me if I’m mistaken, because they deserve some applause.
With that said - it is a disaster. I’ve been reluctant to join the chorus of doomsayers without gaining a crystal clear understanding of the mechanisms and the implications; having now done so, the only thing left to do is to share what I’ve learned with you, and hope that between us, we might be able to reach a few of these people before it’s too late.
If you took a COVID-19 vaccine, you need to read this. Myself, and many others, have been trying to save you from your own arrogant, self-righteous selves for years at this point.
Last chance.
If you’re here for the hard science, feel free to skip ahead to the “long” version. It’s essentially the same content, but much more technical, detailed, accurate, and thoroughly cited.
The short version
Immune reactions are violent, corrosive, and damaging to the body. This is by design; just as an army goes to war, the immune system physically fights invading pathogens, and the weapons it uses cause collateral damage. Sometimes, they cause a lot: immune overreaction is a hallmark of SARS-CoV-2, and among the primary causes of mortality for severe COVID. This is why we suffer inflammation: just as your skin will become inflamed if you spill acid on it, so too will your blood vessels and organs, as your immune system pours acid on them. Usually, that’s a good thing: infected cells often (although not always) need to be destroyed, and our immune systems are all too happy to oblige.
Of course, your immune system does not actually know whether any given foreign body warrants battle stations. This is among the reasons ordinary vaccines are injected alongside toxic adjuvants; they cause a bit of local mayhem to make sure your body knows that this is a bad one and you need to fight it. You may or may not be aware that the mRNA vaccines do not come with adjuvants. I suppose they figured that the spike alone is toxic enough - does it really need any? Partially due to that absence of adjuvants, it appears that the immune systems of people vaccinated with mRNA are deciding that the virus actually isn’t worth fighting at all.
When the body is repeatedly exposed to a harmless foreign body, such as pollen, dendritic cells make a judgment call, and they begin producing IgG4 antibodies*. These are effectively sleep signals: upon encountering the foreign body, the antibody binds to it, any immune cell it encounters will be instructed to leave it alone, and they oblige; these are not the droids you are looking for.
*I know. Skip to the hard science if you don’t want the simplified version.
That’s great for preventing the extensive, unnecessary damage that would occur if you were to be constantly fighting harmless, non-replicating foreign bodies. However, SARS-CoV-2 is emphatically not that: the spike alone is incredibly damaging, proteins produced by the virus cause a lesser level of inflammation in their own right, and uncontrolled replication of almost any pathogen inevitably leads to organ failure and death due to cell damage and dysfunction alone.
To borrow, and extend, a brilliant analogy from
, who said it best: consider a home invasion. The virus is a burglar, and that burglar is coming to take your stuff. Thus far, nobody has been home, but the alarms have still been working; the original antigenic sin caused by outdated mRNA has thus far precluded a fully effective antibody response, but the alarm is still on, and the cops are going to show up eventually. Their diseases have been more severe and lasted longer, but they've still been, for the vast majority, generally able to survive. That's about to change.The situation we now find ourselves in is much worse. Not only is nobody home anymore, but the cops are standing by the door, guarding the burglars. IgG4 antibodies act to suppress the innate immune system as well as the adaptive: they bind to FcγRIIB complexes on cell surfaces that variously deactivate and destroy immune responses and cells, they bind to the virions themselves, they bind to CD4 T-cells and dendritic cells, and and they even bind to the signal cascade transducers of the complement immune system; everywhere they go, the message is loud and clear. Nothing to see here. Please disperse.
I had hoped that at least elements of the innate immune system would be spared. No dice. With even complement being shut down, vaccinees are in for a world of hurt. Consider the excess death statistics that have been steadily rising lately: while these are, thus far, very likely to have been attributable mostly to otherwise silent vaccine injuries, the next time the COVID numbers start rising, we should expect to see vaccinees dying in droves. They likely, mostly, won’t be dying in hospital, either: with the immune response so dramatically blunted, the typical signs and symptoms of infection will likely be all but absent. It would actually be funny, if it weren’t so horrific: uncontrolled replication will lead to trillions of virions tearing unchallenged through the tissues, exposing the victim to a similar quantity of bioactive, toxic spike protein as is created by the mRNA shots. Blood clots, myocarditis, autoimmunity, prion diseases; everything that the shots can cause in the short term, so too will the virus; and the very first clue that they’re even infected may well be their sudden and unceremonious death, perhaps preceded by some general feeling of being unwell if they’re lucky.
As of time of writing, there is no known way to reverse this process. If you are producing IgG4 antibodies in response to the virus, you will likely continue to do so forever, until and unless we find a way to reverse it. Maybe a real vaccine would do it. However, there is still (a great deal of) hope for you: prophylaxis and treatment.
This is the part where you apologize to the people you laughed at for eating horse paste, by the way. Hopefully you’ve already done that. If not - get started. You were wrong. Very, very, lethally wrong, and kind of an asshole about it, too.
The full protocol, and the explanation, is at the bottom of this article. Ivermectin is part of it, but it’s gonna take more than that to save you at this point. You’re lucky anybody’s even still trying. We know what you would’ve done to us in 1943, you rascally little order-follower.

The Long Version
I am very happy to announce … that I finally figured out how to use Substack’s editor properly. Woohoo! They really need to fix the amazing disappearing toolbar. Anyway - throughout this section, you will find that every single statement is very well sourced. If you take issue with something I’ve written, please take the time to read the provided citations before you flip back to Colbert’s Vax-Scene. If this can’t help you understand what’s been done to you, nothing can.
There is a lot to cover, and I am leaving no stone unturned. By the time you reach the end of this article, if you take the time to read the citations, you will have a greater understanding of the relevant aspects of immunology, microbiology, virology, pathology and proteomics than the vast majority of medical practitioners. Some of it you will already know; a lot will be new. What you do with this information is up to you, but I ask that you use it to help the people that need it. After they apologize, perhaps. Clott Adams, lead the way!
Without further ado, let’s get into it.
A Brief Expository Of Everything
The immune system is typically considered to be composed of two broad fields: innate and adaptive. For the purposes of this article, I am expanding it to four: innate, adaptive, complement, and cytosolic. In this manner, we can more accurately identify, compare, contrast, characterize and explore the relevant aspects of each. This will not be a full walkthrough; I could spend a lifetime trying to write that up. Rather, I will focus on and discuss only the relevant sections.
Adaptive Immunity: Antibodies
Adaptive immunity is, largely, centered around the recognition of antigenic peptides, the production of antibodies, the subsequent binding of those antibodies to pathogens, and the interaction of those bound antibodies with various immune cells to elicit various functions. There are several classes, and several subclasses. The ones we will be focusing on are the IgG antibody class.

Upon naïve exposure to any given pathogen, the first antibodies to be deployed will be those of the IgM class. These are very broad and non-specific, and constitute the first step towards building immunity to any given pathogen: once an infection has progressed, pathogen-specific IgG antibodies begin to form. IgG1, IgG2 and IgG3 all play crucial, and occasionally overlapping roles: subsequent to binding to the pathogen, their roles are activating the complement system, marking pathogens for phagocytosis by innate and adaptive immune cells, neutralizing viral entry proteins, ferrying bound proteins to lymph nodes for investigation, and more.
IgG4 is the anti-antibody. It does not neutralize pathogens, cause them to be targeted, or activate complement: rather, it signals to anything it meets that its quarry is harmless, and should not be attacked. IgG4 is expressed upon repeated exposure to a foreign body that dendritic cells, the masterminds of the immune response, have determined to be harmless. The primary example of their function is preventing an unnecessary immune response to pollen. While they have been implicated in autoimmune disease, that is not their relevance here. Going with the military analogy: IgG4 is a blinking IFF (Identification Friend or Foe) signal.
An IgG4 response to a replicating, dangerous pathogen is quite possibly the single worst response we could have induced, and as noted in the beginning, that is exactly what is happening. Serum levels of the different IgG subclasses normally vary somewhat in response to infection. What is not normal is the fact that within a few months of a booster - it is unclear how many, which may also be testament to the fact that a large majority of the shots being given are likely various degrees of inactive - serum levels of IgG1, IgG2 and IgG3 become severely diminished, and the response is dominated by IgG4.

There are several dangerous pitfalls that should have been accounted for in the process of testing these vaccines. The major point of alarm for immunologists has, thus far, been original antigenic sin: if the immune response is strongly trained to recognize only a specific peptide from a pathogen, then upon encountering a mutated version, the incorrectly shaped, non-binding and non-neutralizing antibodies will be produced, and the pathogen will have much greater freedom to replicate and cause disease until the rest of the immune system catches up. In animal trials, death very frequently occurs before that time. Coronaviruses in particular were thought to be particularly susceptible to this problem, due to numerous animal trials around the 2000s, with vaccines trialed against earlier incarnations of SARS, in which every vaccinated animal would consistently die.
Original antigenic sin has proven, over time, to be less of a concern than suspected, with most vaccinated people still able to mount an immune response despite the flawed and outdated mRNA proteins. That must be said, of course, with the major caveat that we don’t actually know what proportion of the vaccines are actually active and producing the spike as intended. Adverse event rates are very strongly correlated with specific batches, and so it is a very reasonable assumption that they are not all the same. Silver lining for those who did not get a “hot shot” - you just might not have to worry about any of this at all. Check your batch number here.
The real concern now is the unexpected shift towards IgG4, and thus immune tolerance. I will detail that after we have covered the other relevant aspects of the immune system.
Adaptive Immunity: T-cells
T-cells are the heavy hitters of the adaptive immune system. There are two primary classes: CD4 and CD8.
CD4 T-helper cells act as the colonels of the battlefield, activating, directing and deactivating the responses of other cells by releasing various cytokines, and receiving orders from HQ. Their depletion is a hallmark of advanced HIV/AIDS; with limited or absent CD4 activity, the immune response is heavily blunted, and lymphocyte recruitment to the site of infection is decreased. CD4 is already somewhat depleted even in the course of normal SARS-CoV-2 infection, due to HIV gp-120 homologous regions of the spike protein exerting a pyroptotic effect on CD4 due to interaction with the CD4/CCR5 receptors. It has also been observed to directly infect CD4 T-cells, much like - you guessed it - HIV.
Continuing the battlefield analogy: if CD4 are the colonels, then cytotoxic effector CD8 T-cells might be the air support. Upon activation by both CD4 cytokines, subsequent recognition of an antigen on the cell surface within the MHC-I complex, and CD28, CD80 and CD86 cytokines at the surface of an infected cell, CD8 will begin to attack an infected cell with perforin and granzymes to effect its destruction. CD8 is unique in that it is capable of targeting cells, such as neurons and gonadal cells, which are otherwise privileged against immune attack; given the wide variety of cells which SARS-CoV-2 is capable of infecting, this is a saving grace that enables us to clear what would otherwise become a very difficult, latent chronic infection. CD8 is one of our immune systems’ most powerful weapons, although it will also cause significant collateral damage to uninfected tissues.
Innate Immunity: Phagocytic cells
Innate immunity constitutes the immune cells which, very broadly, act based not upon recognition of any particular antigens, but upon immune signals, called cytokines, which are released by all manner of cells for widely varying purposes. In response to various cytokines, innate immune cells can become active or inactive, produced in greater or lesser number, utilize chemotaxis to migrate to a site of infection, and release cytokines of their own to coordinate with the wider immune system.
The innate immune cells of relevance to this discussion are neutrophils, monocytes, macrophages, and dendritic cells.

Neutrophils are the very first innate line of defense, and are perhaps the absolute most effective countermeasure to SARS-CoV-2 we possess - and in the face of the IgG4 class switch, are likely to be the only defense retaining any useful functionality. Neutrophils, uniquely, do not significantly interact with IgG4 at all: if they encounter an infected cell, or a free virion, they will destroy or consume it, respectively, and release cytokines to promote inflammation and further immune response. They are, however, a double edged sword: thanks to a quirk in our evolution, we lack a crucial component required for their proper functioning, which we can now only obtain in our diets; without sufficient amounts of it, which are never present without very deliberate and knowledgeable administration, neutrophils rapidly burn out upon deployment and undergo NETosis, a unique form of apoptosis whereby net-like proteins are released to ensnare any nearby pathogens, and strongly promote local inflammation. (Read to the end for a further exploration of this.) Their non-interaction with IgG4 is a saving grace that, properly applied, will be able to save lives, even in the face of an otherwise pretty thorough shutdown of the immune response.
Monocytes and macrophages are important for both directly destroying infected cells, phagocytosis of free virions, presenting viral peptides to dendritic cells for recognition and antibody production, and cytokine signaling to cause localized inflammation and further immune involvement. I am not going to cover them in too much detail here - you’ll find out why shortly - but each of these functions are vitally important for a successful immune response to SARS-CoV-2 infection.
Dendritic cells are the brains of the adaptive immune system. By capturing freely soluble antigenic peptides in serum, usually present due to CD8 destruction of an infected cell, they assess the antigen and determine the appropriate immune response. If CD4 T-cells are the colonels directing the battle, dendritic cells are the generals directing the war, and both CD4, CD8, B-cells and more receive their instructions from the dendritic cells. They are responsible for directing the class switch towards IgG4; precisely why and how are neither particularly well understood, nor at this time particularly relevant, as pertains to a vaccinee’s ability to survive an infection. I am also not covering these in all too much detail, for the same reason.
Complement: The Rube Goldberg Machine
If we’ve discussed the generals and the colonels of this war, then the complement system might best be characterized as roving gangs of hostile neighborhood kids: summoning the adults, leaving grenades in your boots, taking potshots at you, and occasionally starting a ruckus for absolutely no reason at all.
Complement is a fabulously complex system of interconnecting proteins, ubiquitous throughout bodily fluids. They operate via cascading signaling pathways and interactions; upon detection of a pathogen, or occasionally completely randomly, they begin what is called a complement cascade, progressively binding to each other, and to various immune cells’ receptors, to alert the immune system of a potential issue. The complement cascade is a vital component of every immune response, and assists in both activation of the immune system, and localization of immune cells to an area of infection. Their communication is two-way: the wider immune system can also inactivate the cascade, typically upon resolution of the infection, when an immune response is no longer required.
I will not go into much more detail about complement, either.
Are you starting to wonder why?
Cytosolic Immunity: The Other Rube Goldberg Machine
The cytosolic functions pertaining to the immune system are typically categorized under innate immunity. However, for the purposes of this article, I am referring to them as a class of their own, and generally referring to non-immune cells: endothelial, myocytes, parenchymal cells and neurons, to name a few. The cell cytosol is the interior of any given cell, excluding the interiors of the organelles such as mitochondria, within which most cell processes essential to life take place. There are numerous functions carried out inside the cell which pertain to the proper functioning of broader innate and adaptive immunity, within which are defensive mechanisms against infection that do not require any exterior involvement. Similarly to complement, they act in a cascading fashion dependent on numerous interactions. The most relevant functions are the NF-κB pathway, the Toll-like receptors, and the major histocompatibility complex I (MHC-I). There are, broadly, three distinct signaling cascades that will take place upon viral infection of a cell.
The first is the most optimal. If the cell has already been warned of potential infection by the release of interferons from neighboring cells, it will be prepared for the infection; TLR3, TLR7 and RIG-I will detect the viral particle in the endosome, endosomal maturation will occur and turn it into an endolysosome, which will proceed to destroy the viral protein; and the chopped-up peptides will be presented on the cell surface in an MHC-I protein complex, for presentation to the adaptive immune system. The cell will also release interferons to warn nearby cells again.
The second is the most common. If the cell is not prepared for infection, immune-evasive functions of SARS-CoV-2 enable it to prevent both endosomal maturation and detection, enabling endosomal escape of the viral protein in the cell, where it begins replicating; further immune evasive functions hamper the production of MHC-I and interferons, enabling the infection to go undetected by the broader immune system for some time, albeit not indefinitely, at which time the cell will release interferons to warn neighboring cells. This describes the initial stages of most naïve infections.
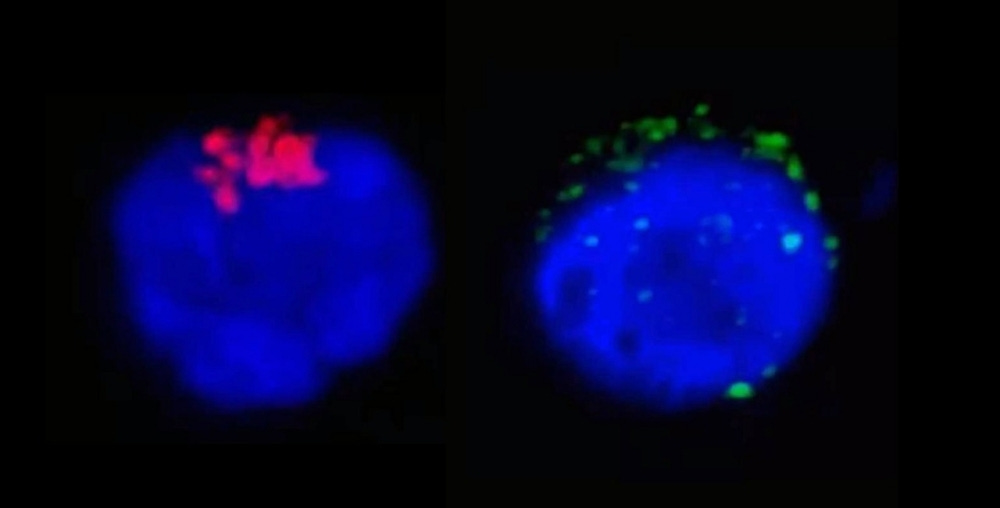
The third is what our unfortunate vaccinees will undergo. In a similar process to antibody-dependent enhancement, the binding of the IgG4 antibody permits viral endocytosis via Fc receptors on the cell surface, as opposed to the more common ACE2 receptor. The binding of the FcγRIIB receptor by the IgG4-virion complex causes PI3K to bind the nuclear localization signal of the NF-κB factor, inhibiting the production of cytokine signals and MHC-I surface presentation of viral peptides. In concert with the immune evasive functions of SARS-CoV-2, this allows the virus to replicate completely uncontested and undetected by the immune system.
Synthesis
If you’ve made it this far, congratulations! We have covered the relevant basics of immunology as it applies to SARS-CoV-2 infection. To summarize, the most relevant and necessary immunological functions to respond to an infection by SARS-CoV-2 are as follows:
Dendritic cells: Recognition of viral peptides, determination of immunoglobulin (antibody) class for production; cytokine signaling to activate immune responses. (Generals)
B-cells are armorers, but they are largely irrelevant to this discussion.
CD4 T-cells: Recognition of viral antigen, dendritic signaling, command and control (C&C) over the local immune response. (Colonels)
Neutrophils: Phagocytosis of free virions, attacking infected cells, and cytokine signaling: powerful, but under most circumstances, very limited, and a double-edged sword. (Heavy armor)
Monocytes and macrophages: As above, and presenting viral peptides to various C&C cells. (Light armor)
CD8 T-cells: Destruction of infected cells. (Air support)
Antibodies: Neutralizing viral entry proteins, and binding to virions to facilitate phagocytosis - or in the case of IgG4, shutting down almost the entire immune response. (Infantry)
Complement: Initial and ongoing detection and signaling of viral infection, and localization of the infection to facilitate chemotaxis of immune cells. (Civilians)
Cytosolic functions: Detection of viral infection, surface presentation of viral peptides to adaptive immune system, release of interferons and cytokines to activate immune response. (Civilian infrastructure)
Sounds great! Everything a well-balanced immune response needs to get you through a war with COVID, all in one tidy human-shaped package.
Here’s what you have when your adaptive immune response is heavily dominated by, or exclusively comprised of, IgG4 antibodies.
Neutrophils.

I hope that you now have an idea of just how incredibly bad this is.
Of course, you didn’t read any of the citations, so really, all the evidence I gave you for that statement was an old South Park meme. Why should you believe me? You shouldn’t, of course. I’m an extremist right-wing anti-vaxxer that thinks he’s a horse, and probably a racist, bigoted transphobe too, right? That’s why I’m going to walk you through the proteomics of every single interaction causing it. There needs to be absolutely no debate about this: this is real, this is how it is, and as surely as we can see that yin fits into yang, we can see that an IgG4-dominated response to SARS-CoV-2 is an unparalleled, utter disaster that is slowly brewing in billions of people across the planet.
Proteomics

As we have covered - and still, only in brief, at this point - the healthy operation of the immune system is an incredibly complex, cascading set of interactions between a vast array of different cells, proteins and signaling chemicals, comprising a system designed with equal imperatives to both defend the body against invading pathogens, and to prevent unnecessary, accidental damage to the body. Both of these mandates are vital and exist in a delicate, ever-shifting balance. If the defense fails, you have AIDS; if the defense is overactive, you have autoimmune disease. The systems in place to prevent unnecessary activation carry just as much weight as those which cause activation.
Unfortunately, the IgG4 class switch represents a full-throated shift towards deactivation of the entire response upon detection of SARS-CoV-2 antigens, affecting almost every step in the cascades. There are multiple means by which the cascades may begin. These cascade steps, and their sabotage by IgG4, are as follows. Specific receptors, receptor bindings, relevant domains, etc. are noted in [brackets].
Starting point: Viral infection of a cell
The SARS-CoV-2 virion, with an attached IgG4 antibody, infects a cell, setting off the cascade which leads to presentation of viral peptides within an MHC-I complex on the cell surface.
SARS-CoV-2 [RBD] infects cell [ACE2]. Proteasome degrades viral protein and causes surface presentation of antigenic peptides [MHC-I].
IgG4 [Fab] binds to SARS-CoV-2, infecting the cell [Fc] through a different receptor [FcγRIIB/CD32b] → This is also known as antibody-dependent enhancement (ADE)
CD8 [TCR] binds to infected cell [MHC-1-peptide complex] and destroys the cell.
Soluble peptide enters dendritic cell [TLR, CLR, endo/phago/pino-cytosis].
Immune signaling is disabled, cell is not destroyed, and no antigen is released
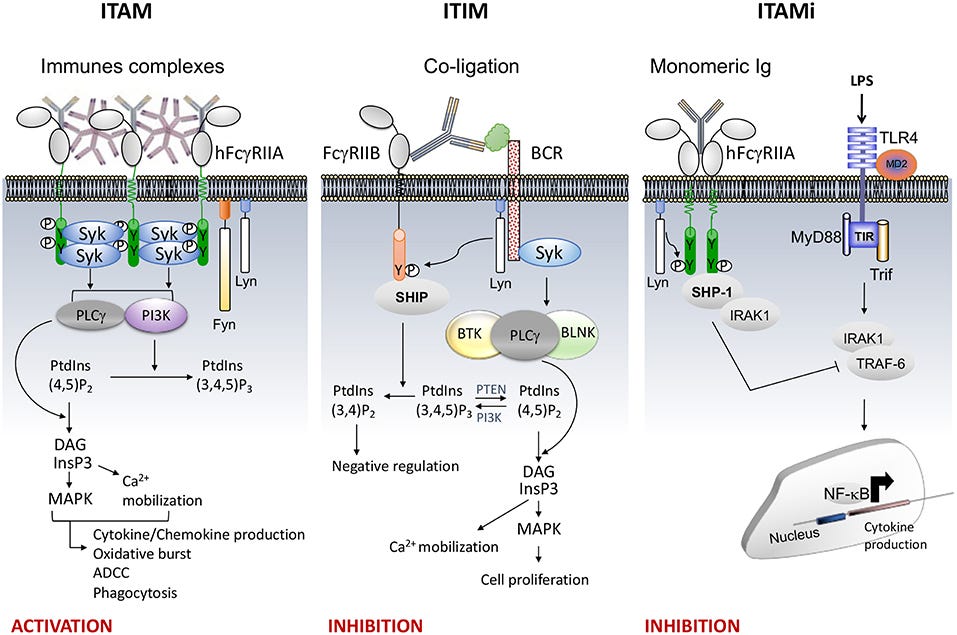
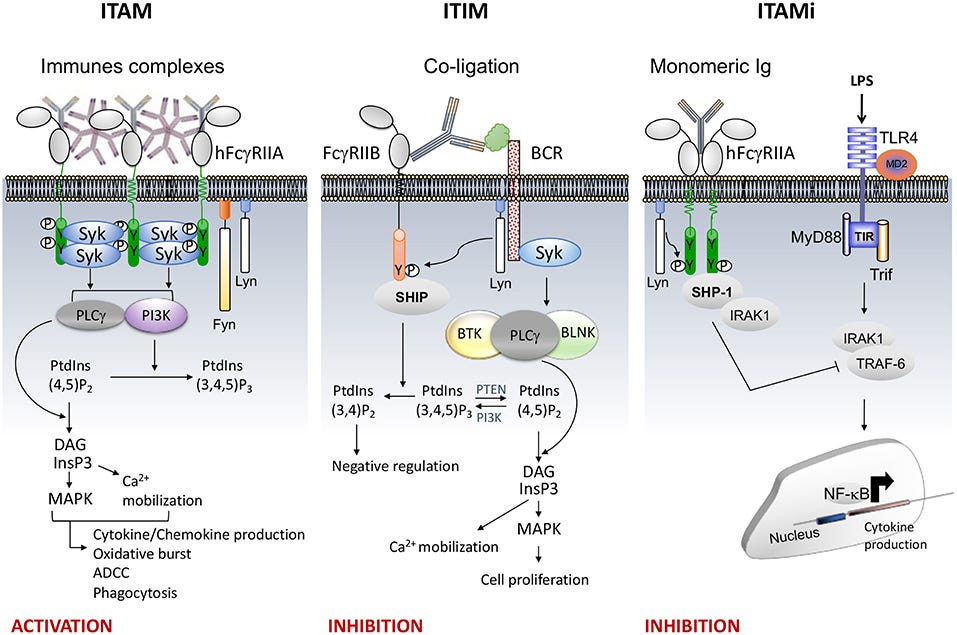
Ben Mkaddem, S., Benhamou, M., & Monteiro, R. C. (2019). Understanding FC receptor involvement in inflammatory diseases: From mechanisms to new therapeutic tools. Frontiers in Immunology, 10. https://doi.org/10.3389/fimmu.2019.00811
That is, quite simply, the end of the line for that pathway. Step 3 is where broader immune activation would otherwise take place. It does not, and can not, due to IgG4 inhibitory action. That is, of course, not the only relevant immunological pathway. Let’s explore another.
Starting point: Macrophage phagocytosis of a free virion
A SARS-CoV-2 virion in serum, with an attached IgG4 antibody, is captured by a patrolling macrophage, eventually setting off the cascade which leads to presentation of viral peptides within both MHC-I and MHC-II complexes on the cell surface.
SARS-CoV-2 [S, E, M] binds to and enters macrophage [Fc, PRRs, TLRs, PAMPs, MARCO, and so on].
IgG4 [Fab] with attached virion binds [Fc] to macrophage [FcγRIIB/CD32b], causing the following effects:
Inhibition of phagocytosis → no MHC-I or MHC-II antigen presentation
Suppression of TNF-alpha, IL-12, CD80, CD86, and other inflammatory cytokine production via [SOCS] → [JAK/STAT] inactivation
Lack of cytokine production → reduction of dendritic cell maturation
Macrophage [MHC-I, MHC-II] presents viral antigen to CD4 and naïve CD8 respectively [TCR].
Virion is never phagocytosed, and/or macrophage is dead. No antigen is presented.
Macrophage releases various cytokines to activate other immune functions.
Oh, what could have been!

That’s the end of the line for that pathway! The macrophage is prohibited from creating and presenting viral antigen, and issuing cytokine signals, due to the IgG4 suppressive action, and/or possibly apoptosed. Steps 2 and 3 would have initiated a broader immune response. That’s alright though! Our immune system is incredibly expansive, and we have other options.
Starting point: Dendritic cell uptake of soluble peptides
CD8 has destroyed an infected cell, and the cell’s contents have been released into serum, where a dendritic cell (DC) encounters and binds a viral peptide, which has been bound by an IgG4 antibody.
Dendritic cell [TLR, CLR] binds and endo-cytoses the viral peptide.
Peptide-IgG4 complex [Fc] binds to the dendritic cell [FcγRIIb]
Dendritic cell [MHC-I, MHC-II] presents viral antigen to CD4 and naïve CD8 respectively [TCR].
Viral antigen is not phagocytosed, and no antigen is presented. CD4 and naïve CD8 remain inactive.
Dendritic cell [MHC-II] migrates to the lymph node to present viral antigen to B-cells for differentiation and increased antibody production.
Migration is inhibited. No further antibody differentiation or immune activation takes place.
And that’s the end of the line for that particular pathway. We are running rather low on methods by which our immune system is capable of initiating a response to the infection.

Starting point: Complement binding to virion
A serum SARS-CoV-2 virion’s spike, with an attached IgG4 antibody, is bound by the complement protein C1q, which initiates a complement cascade. This will happen constantly whilst virions are present, so this response will never quite be fully disabled. It’s only mostly dead.
Complement C1q binds a SARS-CoV-2 virion in serum.
IgG4 antibody [Fab] attached to the virion binds C1q and interrupts the initiation of the cascade.
C1q initiates the complement cascade, leading to the formation of the C3 convertase, and the subsequent activation of the complement system.
The complement cascade is blocked, due to the presence of the IgG4 antibody. The complement system is not activated.
The complement cascade leads to the formation of the membrane attack complex (MAC) and the lysis of the virion.
The MAC is not formed, and the virion is not lysed. The virion remains intact, and the complement cascade is not activated.

That is every major function of the immune system, almost entirely inactivated, by means of a natural immune response that is designed to do precisely what it is doing. If you feel that I have missed a few pathways - which I probably have - please feel free to do your own investigation and determine whether they are equally decimated by IgG4. A lot of people will be rather relieved to hear that Pfizer hasn’t managed to completely destroy their immune systems yet. Sure not for a lack of trying.
So, what can we do?
Thus far, there is no evidence to suggest this IgG4 class switch is occurring in non-vaccinated people. If you just happened to win your “coin flip,” by “pure chance” - congratulations! You probably don’t have to worry about any of this. Probably.
If you did take the shot, and you weren’t lucky enough to avoid a hot shot, then you’re probably in trouble. Nevertheless, even with so little immune function remaining, there is still a path - albeit, a rather narrow path - to near-complete protection from SARS-CoV-2, that is almost as good as still having a functional immune system…
No comments:
Post a Comment