Shingles Activation Associated With COVID Jab
- January 04, 2023
Story at-a-glance
- According to a recent case study, persistent post-jab shingles was associated with the presence of COVID jab spike protein in the affected skin. The researchers speculate that the COVID jab may induce persistent shingles reactivation by perturbing the immune system
- Another study details the cases of six patients with autoimmune inflammatory rheumatic diseases who developed shingles shortly after their Pfizer jabs. None of the healthy controls developed shingles post-jab
- A systematic review also concluded that the COVID jab increases the risk of shingles reactivation if you’ve had it before or have known risk factors for it
- The COVID shots suppress your innate immune system by inhibiting the type-1 interferon pathway, which is the first-stage response to all viral infections. Type-1 interferon also keeps latent viruses in check, so if your interferon pathway is suppressed, latent viruses can start to emerge
- Type 1 interferon is suppressed by the jab because it responds to viral RNA, and viral RNA is not present in the COVID shot. The RNA is modified to look like human RNA, so the interferon pathway is not triggered
According to a recent case study1 published in the Journal of Cutaneous Immunology and Allergy, persistent post-jab shingles, aka herpes zoster, an infection caused by the varicella zoster virus, was associated with the presence of COVID jab spike protein in the affected skin. As explained by the authors:2
“Since the campaign of vaccination against COVID-19 was started, a wide variety of cutaneous adverse effects after vaccination has been documented worldwide. Varicella zoster virus (VZV) reactivation was reportedly the most frequent cutaneous reaction in men after administration of mRNA COVID-19 vaccines, especially BNT162b2.
A patient, who had persistent skin lesions after BNT162b2 vaccination for ... over 3 months, was investigated for VZV virus and any involvement of vaccine-derived spike protein ... Strikingly, the vaccine-encoded spike protein of the COVID-19 virus was expressed in the vesicular keratinocytes and endothelial cells in the dermis.”
COVID Jab Impairs Your Immune Function
The researchers speculate that the COVID jab may induce persistent shingles reactivation by “perturbing the immune system.” How your immune system is perturbed by the COVID shots is the topic of MIT researcher Stephanie Seneff’s paper3 “Innate Immune Suppression by SARS-CoV-2 mRNA Vaccinations: The Role of G-quadruplexes, Exosomes and MicroRNAs,” co-written with Drs. Peter McCullough, Greg Nigh and Anthony Kyriakopoulos.
In it, they describe how the COVID shots suppress your innate immune system by inhibiting the type-1 interferon pathway, which is the first-stage response to all viral infections.
When a cell is invaded by a virus, it releases type-1 interferon alpha and beta. Both of these molecules act as signaling molecules that tell the cell it’s been infected. That, in turn, launches the immune response and gets it going early in the viral infection.
Type-1 interferon also keeps latent viruses in check, so if your interferon pathway is suppressed, latent viruses can start to emerge. The U.S. Vaccine Adverse Event Reporting System (VAERS) database reveals many who have been jabbed report these kinds of infections. Regulators in the European Union are also warning that repeat COVID shots can weaken overall immunity.4
How is type-1 interferon suppressed by the jab? It’s suppressed because type-1 interferon responds to viral RNA, and viral RNA is not present in the COVID shot. The RNA is modified to look like human RNA, so the interferon pathway is not triggered. Worse, the interferon pathway is actively suppressed by the microRNA in the shot, which limits your ability to fight off all viruses. It also opens the door for latent viruses to reactivate.
In the case study above, the patient had received one dose of Pfizer’s mRNA shot 13 days before the shingles outbreak and a second dose eight days after, causing the researchers to suspect there was an association between the outbreak and the shots.
COVID Jab and Shingles in the Immunocompromised
Similarly, a study5,6 published in April 2021 detailed the cases of six patients with autoimmune inflammatory rheumatic diseases who developed shingles shortly after their Pfizer jabs.
“The safety profile of mRNA-based vaccines in patients with autoimmune inflammatory rheumatic diseases (AIIRD) is unknown,” the authors noted.7 “The objective of this report is to raise awareness of reactivation of herpes zoster (HZ) following the BNT16b2 mRNA vaccination in patients with AIIRD.”
The study found herpes infection occurred in 1.2% of AIIRD patients who got the shot (six out of 491), compared to none among controls. Five of them developed shingles for the first time in their life a short time after their first dose of Pfizer. One got it after her second dose.
As noted by the authors, immunosuppressed patients, including patients with AIIRD, have been prioritized for the COVID jab, even though immunosuppressed patients were excluded from the clinical trials. The fact that 1.2% of immunocompromised patients developed shingles, whereas none of the healthy controls suffered this fate, shows you just how important it is not to confine clinical trials to the healthiest among us.
Pathogenic Mechanisms
As for the mechanisms, the researchers offered the following:8
“Potential mechanisms that might explain the pathogenetic link between mRNA-COVID19 vaccination and HZ reactivation are related to stimulation of innate immunity through toll-like receptors (TLRs) 3,7 by mRNA-based vaccines. TLR signaling has been implicated during reactivation of herpesviruses, a process essential for these viruses to maintain themselves in the host.
Defects in TLR expression in patients suffering from diseases caused directly by herpesvirus infection highlight the importance of these signaling pathways during infection and eventual disease progression.
The vaccine stimulates induction of type I INFs [type 1 interferon] and potent inflammatory cytokines, which instigate T and B immune responses but may negatively affect antigen expression potentially contributing to HZ reactivation.”
COVID Jab Raises Risk of Shingles Reactivation
A systematic review9 published in November 2021 also concluded that the COVID jab increases the risk of shingles reactivation if you’ve had it before or have known risk factors for it. Fifty-four cases involving 27 men and 27 women had been reported at the time and were included in the review. As noted by the authors:10
“There were cases with known risk factors for herpes zoster, which included age more than 50 years (n = 36), immunological disorders (n = 10), chronic disease (n = 25), metabolic disorder (n = 13), malignancy (n = 4), and psychiatric disorder (n = 2).
The mean (SD) period between development of herpes zoster and COVID-19 vaccination was 7.64 (6.92) days. Majority of the cases were from the high-income and/or middle-income countries. 86.27% of the cases of HZ were reported due to mRNA vaccine. Thirty-six patients 36/45 (80%) developed herpes zoster following the priming dose of COVID-19 vaccine among those who received mRNA vaccine.
We could not establish definite link but there may be possible association between COVID-19 vaccine and shingles. Large-scale studies may help to understand the cause-effect relationship.”
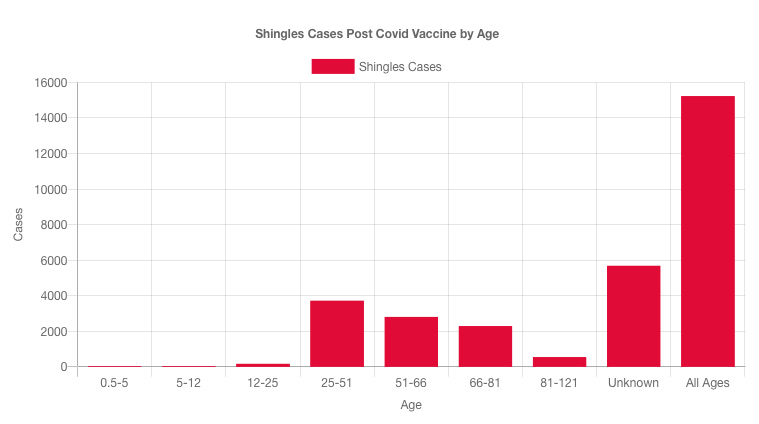
Shingles Reports in VAERS
Looking at VAERS, as of December 16, 2022, there were 15,225 reports of shingles after the COVID jab.11 Most cases (for which age are given) have occurred in younger individuals between the ages of 25 and 51, which is younger than normal. There are even 170 cases in 12- to 25-year-olds.
The Pfizer shot has more than double the number of shingles reports associated with it than Moderna, and there are more than twice the number of reports from women than men.
Can VAERS Data Demonstrate Causality?
One person who has taken a strong stance against the claim that VAERS data cannot tell us anything about causation is Steve Kirsch, executive director of the COVID-19 Early Treatment Fund. In the video “Vaccine Secrets: COVID Crisis,”12 he argues that VAERS can indeed be used to determine causality.
It’s important to realize that the idea that VAERS cannot show causality is part of how and why the CDC can claim none of the deaths is attributable to the COVID shot. Kirsch argues that this premise is in fact false, and that causation can be determined using VAERS’ data.
To prove his point, Kirsch gives the following analogy: Suppose you give a two-dose vaccine. After the first dose, nothing happens, but after the second dose, people die within 24 hours of a deep vein thrombosis (DVT).
When you look at the VAERS data, what you would find is no reports associated with the first dose, and a rash of deaths after the second dose, all within the same timeframe and with the same cause of death.
According to the CDC, you cannot ascribe any causality at all from that. To them, it’s just random chance that everyone died after the second dose, and from the same condition, and not the first dose or from another condition.
Kirsch argues that causality can indeed be identified from this kind of data. It’s very difficult to come up with another explanation for why people — many who are young, in perfect health with no predisposing conditions — die exactly 24 hours after their second dose. It’s even difficult to come up with another explanation for people who do have underlying conditions.
For example, is it reasonable to assume that people with, say, undiagnosed heart conditions, would die from DVT exactly 24 hours after getting a second dose of vaccine? Or that people with undiagnosed diabetes would die from DVT exactly 24 hours after their second dose?
Why not after the first dose, or two months after the second dose, or any other random number of hours or days, or for other random cause of death? Why would people randomly die of the same condition at the exact same time, repeatedly?
At bare minimum, as an early warning system, VAERS is designed to flag potential causation. It’s by looking for repeated patterns of side effects that you would begin to identify a potentially problematic vaccine.
Once a pattern is identified — and there’s no denying death within 24 hours to one week is a pattern seen for the COVID shots — an investigation should be launched. But no such investigation has been launched into the COVID jabs. Clear-cut patterns are simply ignored.
Ignoring Warning Signs Does Not Make the Shots Safe
As an early warning system, VAERS is performing as intended, despite severe underreporting (the CDC even published a paper in which they admitted COVID jab adverse effects in children are underreported by a factor of 6.513). It’s the follow-up that’s lacking.
But lack of investigation and follow-up is not evidence that the shots can’t cause problems, one of which is reactivation of latent viruses such as shingles. While I don’t believe these shots are beneficial for anyone, if you have a history of latent infection, be aware that the shot may cause a flare-up.
Also be aware that having a compromised immune system will render you more prone not only to COVID-19 but also any number of other viral and bacterial infections, plus chronic diseases such as cancer.
No comments:
Post a Comment