6 Big Differences Between Natural Vs. Vaccine-Induced Immunity
At the time the UK government and media were pumping out a narrative that most people who were becoming infected with COVID were unvaccinated, the prestigious Lancet journal quietly revealed that, in actual fact, 89% of cases were among the vaccinated.
Miss a day, miss a lot. Subscribe to The Defender's Top News of the Day. It's free.
“Humankind has never had a more urgent task than creating broad immunity for coronavirus. Realistically, if we’re going to return to normal, we need to develop a safe, effective vaccine. We need to make billions of doses, we need to get them out to every part of the world, and we need all of this to happen as quickly as possible. — Bill Gates, GatesNotes, April 30, 2020
There are three key elements to Gates’ perspective captured in his blog from April 2020 that we’re now in a position to evaluate retrospectively. These elements relate to his call for 1) the need for broad immunity, 2) a safe and effective vaccine and 3) mass and rapid deployment of these vaccines.
The top line evaluation looks something like this:
- The COVID-19 jabs have comprehensively failed to do deliver “broad immunity.” They deliver narrow and short-lived, non-durable immunity that is inferior to the more robust, durable and broader-based immunity acquired following infection by SARS-CoV-2. Please read on.
- The illusory claim of “safe and effective” COVID “vaccines” still perpetuated by health authorities, vaccine manufacturers and the mainstream media is now severely battered. There is now overwhelming evidence of the failure of the jabs to prevent transmission (the primary purpose of conventional vaccines), most notably the omicron variant, the highest infection rates are consistently found in the countries with the greatest jab coverage, rapidly waning effectiveness in reducing risk of hospitalization and death, and an emerging picture of significantly under-reported and widespread vaccine injuries and disruption of the immune response (here, here and here).
- While there’s no doubt “they” achieved “mass and rapid deployment” at least in some parts of the world, there are other parts, such as the vast continent of Africa, where presently only 11% of the population are “fully vaccinated against COVID-19” (i.e., two doses).
More than this, there was no scientific basis to indiscriminately expose such vast numbers of people to the experimental jabs, regardless of their infection status, health status, susceptibility or prior immunity from previous infection.
The notion of superhuman immunity by this new generation of genetic “vaccines” has thus been tarnished since Gates and others set the global public’s vision on a high risk proposition.
Comparing intramuscular COVID-19 injections and natural immunity
Before we take a look at what happens immunologically through these two routes — let’s just recap the process of what happens when someone becomes infected with SARS-CoV-2. Those who want to dive in deeper can find out more in this “Trends in Immunology” article.
Here’s the simplified explanation: Assuming the virus breaches the physical and chemical barriers of the respiratory mucosa, the virus attaches to the ACE2 receptors in the epithelial cells immediately beneath the mucosal layer.
It then penetrates the epithelial cell and after being uncoated, it takes over the replication machinery of the cell (in the ribosomes), starts replicating, new virus particles are then assembled (in the endoplasmic reticulum), recoated and when mature they are released from the cell.
They may then invade other cells in the body while some might be released back through the airways (so potentially infecting others) or into the gastrointestinal tract where they may be shed through the anus.
How much infection occurs is down to many factors, including how big the viral load is in the first place and how competent both the innate and the adaptive arms of the immune system are at clearing the infection.
A less well known fact is that a complex array of microtubules (actin filaments — a “cytoskeleton”) are involved in the transport and assembly of spike proteins into virions during the replication cycle — this being the reason some clinicians have used colchicine (derived from meadow saffron Colchicum autumnale) more well known for treating gout flares in early COVID treatment where there is evidence of microclotting in the lower lung.
Let’s now look a six big differences between natural versus jab-induced immunity:
1. Intramuscular jabs don’t induce sterilizing immunity in the upper airway
When the deltoid muscle of the upper arm is injected with either an mRNA (Pfizer or Moderna) or an adenoviral vector (AstraZeneca, Janssen, Sputnik) jab, there is a delay of a few days before the body starts to produce a modified form of the spike protein found in the original Wuhan strain of SARS-CoV-2.
Over another few days, this then triggers an elevation of anti-spike antibodies, initially IgM, soon replaced by IgG. This happens within the body, but doesn’t affect the anti-spike IgA that is produced in epithelial cells of the airway adjacent to the respiratory mucosa, the normal entry point for airborne SARS-CoV-2.
This abnormal relationship between IgG and IgA titres that doesn’t occur following naturally-acquired infection is one of the reasons jabbed people who are subsequently infected can still shed (transmit) so much virus to others.
2. Intramuscular jabs induce immunity that wanes quickly while naturally acquired immunity is more robust and durable
This is undisputed, even for the delta variant. Waning has triggered health authorities to push boosters, but for omicron, even boosters have little or no impact on reducing transmission.
It was only just over a year ago that one of the most influential medical scientists in the world, Dr. Eric Topol of the Ragon Institute, Harvard and MIT, writing with Dennis Burton from Scripps, in the peer reviewed journal Nature Medicine tried to get us excited about “superhuman SARS-CoV-2 immunity” from the novel COVID-19 jabs.
The article ends with the scientists expressing their optimism that a vaccine (or vaccines) would deliver an immune response “superior to that achieved through natural infection.” Let’s now recalibrate, a year on.
Today, Burton and Topol’s view looks fantastical. Especially alongside the 146 research studies collated by Drs. Paul Alexander, Peter McCullough and others that are accessible via the Brownstone Institute website that provide overwhelming evidence of the superior robustness and durability of naturally-acquired versus jab-induced immunity.
3. Intramuscular jabs induce immunity to the spike protein of the original Wuhan strain of SARS-CoV-2, not the currently circulating forms such as omicron or delta
It is a technological reality that the manufacturers are trying to get around in the knowledge that existing jabs are based on a no longer circulating variant and omicron successfully evades the immune response. The answer? Apparently, it is an update of the antigen coded into the mRNA or DNA or delivered as spike protein in omicron-specific jabs. Pfizer is due to roll out one such updated jab as early as next month.
But hold on. Given the much lower risk of severe death posed by omicron, the now accepted tendency for regular, say six monthly, dosing with these novel genetic jabs and evidence of an ever greater spectrum of short- and long-term harms, shouldn’t the risk/benefit equation be re-assessed from the ground-up before they’re discharged into the bodies of healthy populations?
4. The payload of intramuscular jabs is not limited to the deltoid muscle as we were led to believe in the early days of roll-out
The view that antigen-presenting cells from lymph nodes are attracted to the deltoid muscle injection site where B cells go on to produce sterilizing antibodies surprised many of us when we heard it.
This is because it was already well known that a comprehensive immune response could only be mounted by at least engaging the lymphatic system of the body (including lymph nodes and spleen), a point clarified in the BMJ by a group of leading professors at St. George’s Hospital in London.
Canadian viral immunologist Dr. Byram Bridle became a target of the experimental jab protagonists when he was the first to publicly disclose a Japanese biodistribution study that was contained within Pfizer’s dossier that was in turn submitted to major drug regulators for their review prior to granting Emergency Use Authorizations (EUAs) for the company’s experimental COVID-19 jab.
This meant that drug regulators like the U.S. Food and Drug Administration and the UK Medicines and Healthcare Regulatory products Agency were fully aware prior to the EUAs being issued that the contents of the mRNA jabs got into circulation and entered organs like the spleen, ovaries, heart and brain.
A major contrast to the public health messaging that suggested the entire immune reaction occurred in the vicinity of the injection site in the deltoid muscle.
5. Intramuscular jabs rely heavily on inducing immunity through B cell IgG antibodies and not innate immunity or T cells
Whether a particular jab relies on the body producing the spike protein antigen (mRNA e.g., Pfizer, Moderna, or adenoviral vector types e.g., AstraZeneca, Janssen, CovidShield) or it delivers it directly to muscles (protein subunit type e.g., Novavax, or inactivated virus type e.g., Sinovac), the body’s immune system responds to the invasion.
Neglected in the narrative offered to the public is the role of the innate immune system — the system that responds immediately to the invasion. If we only allow nature to take its course, our bloodstream would very seldom be the first part of the body to be exposed to respiratory pathogens, or parts of them.
That’s what the sticky mucosal layer of our airways have learned to do over millennia (see point 1 above) where it tries to use a series of physical and chemical barriers to impede pathogen entry.
If these barriers are breached, the next line of defense is the gamut of natural killer cells, macrophages, monocytes, innate antibodies and other cells that try to inactivate the pathogen in the epithelial layer immediately adjacent to the mucosa.
These cells are somewhat less specific but they still have the capacity to learn something about the invader through pattern recognition receptors which sense diverse molecular patterns linked to the pathogen as well as to the damage it causes.
People who develop transient or mild disease typically rely on effective innate immunity. People who suffer moderate or even severe disease experience failure of innate immunity and must rely on the last-chance-saloon, the adaptive arm of their immune system that relies on specialized T cells and B cells to drive highly specific, but delayed, immune responses.
The public has been made highly aware of B cell neutralizing antibodies but has been told little or nothing about the crucial role of innate immunity. Or that immune surveillance might be disrupted by the genetic jabs affecting the body’s ability to mop up the daily complement of cancer cells which is heavily reliant on CD4+ and CD8+ T cells.
Not only that, cancer patients typically don’t mount an effective T cells response to the jabs, and those with blood cancers, versus solid tumors, don’t even elicit a proper neutralizing antibody response (see here and here).
Part of the reason for a more robust immune response from naturally-acquired infection versus jab-induced immunity stems from the fact the immune system needs to respond to all 29 proteins when exposed to the actual virus, versus just the spike protein with the jabs.
T cells exposed to one or more antigenic proteins undergo transition from naïve to effector (killer) T cells and they leave behind a population of memory T cells that can do their thing if exposed again to a pathogen expressing the same antigen(s).
The fact that immunity typically drops off after a matter of weeks or months after jabs and many people get reinfected and suffer disease more than once is demonstration that T cell memory doesn’t develop significantly following COVID jabs or it’s too specific to cater for the new variants.
Also, what if the first exposure to spike protein is from the jab and not the currently circulating virus? The imprinting of immune memory from its first exposure means it will be less effective at stonewalling a different variant of a pathogen — a phenomenon known as “original antigenic sin.”
Now back to the much-championed, star performer of the immune system— neutralizing antibodies. They may be the most positively responsive part of the immune system when exposed to the jabs, yet they still fail to fully sterilize SARS-CoV-2 that enters the body within weeks after being jabbed.
Let’s also remember the presence of a given threshold of anti-spike antibodies doesn’t tell you much about how effective a person’s immunity is going to be as that will depend on such things as the variant of the pathogen to which a person is later exposed, the concentration of the antibodies at a given time, and whether those antibodies are of high or low affinity.
6. Might COVID-19 jabs awaken the sleeping dragon of autoimmunity?
I’ll keep this short as we devoted a whole campaign to it last year and collated much of the research in this troubling area. As is the way with the rapidly emerging science, it’s moved on rapidly — becoming an ever-greater concern.
Given the importance of environmental triggers in mediating autoimmune disease, it is highly probable that autoimmune risk will escalate in relation to frequency of exposure so should be a consideration for anyone with a predisposition or existing autoimmune disease who is considering subjecting themselves to regular, say 6 monthly, COVID-19 jabs.
You may be surprised, as I have been, that given the 140 COVID-19 vaccines currently in clinical development, only 8% of them are intranasal — by contrast, a whopping 84% are intra-muscular.
Intranasal vaccines share the same entry pathway as respiratory viruses and would more likely induce the same sequence of innate and adaptive immune responses as natural infection. It turns out that there are considerable technical challenges involved, not least nasal clearing associated with the sticky nasal mucous that serves as barrier to the nasal epithelium.
Nature did its own thing anyway
Now let’s take some of these principles and look at a real world situation, focusing on the UK primarily given the availability of more detailed data, courtesy of the Office for National Statistics (ONS), than in most other parts of the world.
The government of the UK is among several to have decided recently to lift all, or nearly all restrictions. The restrictions followed a now familiar pattern that started with lockdowns, social distancing and masks in an attempt to try to “flatten the curve.” It didn’t work.
Two waves hit hard, the way infection waves do when there is little or no prior natural immunity. Then the third wave hit just as the jabs were rolled out zealously at the end of 2021 to a British population that rolled its sleeves up eagerly, given the programming that enforced the idea this was the only route back to a normal life.
That failed too and another wave struck — but given it was omicron which is much less virulent than previous strains it left many fewer deaths in its wake.
Perversely, Boris Johnson continues to argue — with little in the way of supporting science — that the restrictions can be lifted largely down to the success of the extraordinary booster campaign.
As Figure 1 shows you – booster rates in the UK might be described as impressive by the standards of many other countries.
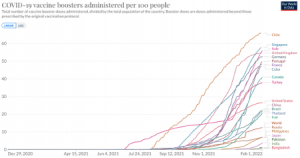
But booster roll-out in the UK, that started to flatline once omicron became evident towards the end of December 2021, pales by the standards of Chile, which has seen the largest escalation of cases it has yet experienced since its booster program has been rolled out (Fig 2).
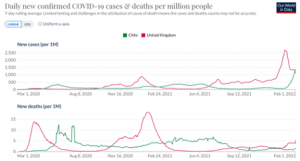
That’s a reminder that the boosters are not working as claimed. People are being lied to by governments, health authorities and the mainstream media. The waves in each of these countries are being generated largely by natural population dynamics and immunity.
At the time that the UK government and media were pumping out a narrative that most people who were becoming infected with COVID were unvaccinated, the prestigious Lancet journal quietly revealed that, in actual fact, 89% of cases were among the vaccinated.
And the science said what?
So what has the recent science been telling us? Short answer: nothing. Longer answer: the science has no capacity to speak or communicate; it’s the scientists who write, speak and communicate specific pieces of scientific information, often ones that please those who have funded their research.
In the case of emerging science, it may not be possible to draw a conclusion that represents consensus among all reasonable, relevantly qualified and experienced scientists. It also, of course, depends on when you ask the question.
Looking at blood tests that measure anti-spike antibodies (largely IgG type), the ONS provides some of the most transparent data anywhere in the world.
The most recent ONS snapshot from the populations of the 4 countries of the UK reveals the following status of anti-spike antibodies as of Jan. 3:
- 0% in England.
- 4% in Wales.
- 4% in Northern Ireland.
- 2% in Scotland.
This begs the question; what proportion of these very high rates of IgG antibodies in the UK population is down to jabs, and how much is from natural infection, nearly all of this now being the result of the omicron variant, which has almost completely displaced delta in the UK (and numerous other countries)?
Deception no. 1
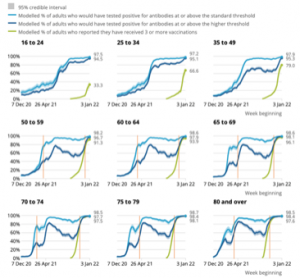
Looking at the modeling work based on actual serology (antibody) tests of blood in the chart below (Figure 3), we can see that the proportion of the under-40s especially (the first two graphs in the series representing age groups 16-24 and 25-34) who are triple jabbed, who in turn may benefit from short-term protection against hospitalization and death, is substantially lower than the near-100% who have elevated antibodies.
This shows just how important natural immunity is for these younger populations – something health authorities have been mute on at a time when there has been unprecedented coercion for this group to receive COVID-19 mRNA jabs. That’s deception no.1.
Deception no. 2
You’ve guessed it. There’s another big deception. Look again at figure 3 and note the vertical red lines we’ve inserted for all age groups 50 and older. The red line on the left of each of the lower 6 graphs intersects the horizontal axis on the date antibodies were found in 80% of the population.
The red line on the right side intersects the horizontal axis on the date boosters were administered to 80% of that same age group.
Note the many months that separate these two events. The take-home is that elevated antibodies were already widespread in the older age groups well before the booster campaign was even started — and even longer before coverage reached 80% of each of the age groups.
It’s also worth noting that antibody-mediated partial (non-sterilizing) immunity in heavily vaccinated populations is increasingly clouded by the fact that it is in essence “hybrid” immunity that, at least for a short period, includes naturally-acquired and jab-induced immunity.
For any population group that isn’t vulnerable to severe COVID-19 disease and COVID-19 death – which represents almost everyone since omicron has become dominant – the risk of serious adverse events almost certainly outweighs any benefits.
Deception no. 2 can therefore be summarized as follows: Boris Johnson deceived the public when he said boosters were the reason the UK was ready to lift restrictions. One wonders, rhetorically, who put those words in his mouth? I, cynically speaking, just can’t imagine.
Call to Action
When there’s so much double speak and deception around, we owe it to our fellow human beings to at least share articles like this that expose the deception through our highly constricted channels of communication.
We thank you, in anticipation that you will share this article as vociferously as Boris Johnson shared his main reason for lifting UK restrictions.
When all he really needed to do was owe his gratitude to nature. And turn his back on Gates’ defective vision that massive investment in novel vaccine technology would deliver a solution fit for humanity.
Originally published by Alliance for Natural Health International.
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the views of Children's Health Defense.
