To Prevent Three Deaths, COVID Jab Kills Two
- July 05, 2021
Story at-a-glance
- The reported rate of death from COVID-19 shots now exceeds the reported death rate of more than 70 vaccines combined over the past 30 years
- The COVID shots are also five times more dangerous than the pandemic H1N1 vaccine, which had a 25-per-million severe side effect rate
- A recent study calculated the number needed to vaccinate (NNTV) to prevent one COVID-19 death, finding that for every three people spared from COVID-19 death, the COVID gene therapy injections kill two. According to the authors, “This lack of clear benefit should cause governments to rethink their vaccination policy”
- There’s evidence that the U.S. Vaccine Adverse Event Reporting System (VAERS) is deleting reports of side effects, especially deaths related to COVID injection. So, not only does VAERS generally capture only 1% to 10% of side effects, but they also appear to be manually wiping reports
- A case report reviews two neurosurgical cases in which patients developed new onset of neurological symptoms shortly after their COVID shots. The two patients were found to have two different types of brain tumors. The authors hypothesize that the shots may trigger inflammation that contributes to neuro-oncologic diseases
If there were any reasonable safety standard in place, the COVID injection campaign would have been halted in early January 2021. The reported rate of death from COVID-19 shots now exceeds the reported death rate of more than 70 vaccines combined over the past 30 years, and it’s about 500 times deadlier than the seasonal flu vaccine,1 which historically has been the most hazardous.
The COVID shots are also five times more dangerous than the pandemic H1N1 vaccine, which had a 25-per-million severe side effect rate.2,3 In a June 24, 2021, peer-reviewed article4 in the medical journal Vaccines, titled, “The Safety of COVID-19 Vaccination — We Should Rethink the Policy,” an international team of scientists warns that we’re killing nearly as many with the shots as would die from COVID-19 itself.
UPDATE: This peer reviewed article was retracted. Please see twitter thread for details.
For Every Three COVID Deaths Spared, Two Die From the Jabs
To compare the risks and benefits, they calculated the number needed to vaccinate (NNTV) to prevent one COVID-19 death. The data came from a large Israeli field study and two adverse drug reactions databases, one with the European Medicines Agency (EMA) and one with the Dutch National Register.
To prevent one case of COVID-19 using the mRNA shot by Pfizer, the NNTV is between 200 and 700. The NNTV to prevent one death is between 9,000 and 50,000, with 16,000 as a point estimate.
Meanwhile, the number of people reporting adverse reactions from the shots is 700 per 100,000 vaccinations. For serious side effects, there are 16 reports per 100,000 vaccinations, and the number of fatal side effects is 4.11 per 100,000 vaccinations.
The final calculation suggests that for every three COVID-19 deaths prevented, two die from the shots. “This lack of clear benefit should cause governments to rethink their vaccination policy,” the authors state in conclusion.
Understand that doesn’t even factor in the anticipated far greater death toll from the COVID jab in the fall, as a result of paradoxical immune enhancement. These numbers will escalate to shocking ratios as the deaths start to increase in the fall.
Toxicologist Calls for End to COVID Vaccination Program
Janci Chunn Lindsay, Ph.D., a prominent toxicologist and molecular biologist who works with M.D. Anderson Cancer Center-Houston, says the current COVID-19 injection campaign is a “massive clinical trial” using the general population as subjects, and is calling for the program to end.
Lindsay, described by investigative journalist Jennifer Margulis as having “extensive experience in analyzing the molecular profile of pharmacologic responses,”5 told the U.S. Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices (ACIP) that Pfizer’s and Moderna’s gene therapy injections have multiple safety concerns and should not be given to children or women of childbearing age.
You can hear her comment in the video above. A transcript of her three-minute comment can be found on Algora.com.6
She pointed out “there is a credible reason to believe that the COVID vaccines will cross-react with the syncytin and reproductive proteins in sperm, ova and placenta, leading to impaired fertility and impaired reproductive and gestational outcomes,” and that there are enough pregnancy losses reported thus far to warrant stopping the vaccines. Lindsay should know, seeing how she worked on a vaccine back in the ‘90s that unexpectedly ended up causing permanent sterility.
Margulis contacted Lindsay after the meeting to see what additional information she had that she was not allowed to present due to the three-minute time restriction. In a written response, Lindsay said:7
“There is strong evidence for immune escape and that inoculation under pandemic pressure with these leaky vaccines is driving the creation of more lethal mutants that are both newly infecting a younger age demographic, and causing more COVID-related deaths across the population than would have occurred without intervention. That is, there is evidence that the vaccines are making the pandemic worse.”
Spike Protein Linked to Heart Inflammation and Much More
The podcast, A Shot in the Dark, also interviewed Lindsay for nearly an hour about her concerns, June 24, 2021, which you can listen to above.8 Importantly, she points out that regulatory agencies and vaccine makers feigning surprise that the COVID shots are causing heart inflammation is completely absurd, as there are “hundreds of studies” linking coronavirus spike proteins to this effect.
She also dismisses the claim that heart inflammation is somehow only affecting younger people. Heart attacks in adults are also a clear sign of this effect, she says. Additionally, clinical evidence given to her by health care professionals who are treating patients injured by these shots suggest the spike protein your body produces in response to them have toxic effects on your bone marrow.
Disturbingly, like many others, Lindsay says there’s evidence that the U.S. Vaccine Adverse Event Reporting System (VAERS) is deleting reports of side effects, especially deaths, post-COVID injection. So, not only does VAERS generally capture only 1%9,10 to 10%11 of side effects, but they also appear to be manually wiping reports.
Brain Tumors Have Developed Post-COVID Jab
In related news, a peer-reviewed case report12 published June 15, 2021, reviews two neurosurgical cases in which patients developed new onset of neurological symptoms shortly after their COVID shots. The two patients were found to have two different types of brain tumors.
The authors point out that even though these processes are considered “unrelated to vaccination,” their hypothesis is that the COVID shots “may induce an inflammatory cascade with the ability to uncover underlying sinister pathology.”
For this reason, they strongly recommend “careful evaluation in the setting of new-onset neurologic symptoms after COVID-19 vaccination.” Of course, by then, it’s going to be too late, so in my view, people need to carefully consider these risks before they submit to these shots.
The first case was a 58-year-old woman who eight years previously had surgically removed melanoma on her right arm. Within two weeks of her second dose of a COVID-19 injection, she developed slurred speech, facial droop on the left side and left arm and leg weakness. Computed tomography (CT) of the head revealed a 3.4 centimeter intraparenchymal hemorrhage in her right lobe, causing a 3-millimeter shift in the midline of the two lobes.
No overt abnormalities were found in her bloodwork. Contrast-enhanced MRI of the woman’s brain further revealed a large hemorrhagic cavity in the right frontal lobe and a hemorrhagic mass. Surgical biopsy diagnosed it as a metastatic malignant melanoma.
The second case was a 52-year-old woman with a history of hypothyroidism and breast cancer. About four days after her first dose of COVID “vaccine,” she developed a severe headache, neck stiffness and intermittent high-grade fevers.
CT imaging and contrast-enhanced MRI of her head revealed a 5.8 cm mass in her corpus callosum. No obvious problems were detected in her blood work. Biopsy revealed the mass to be an IDH-wildtype Grade IV glioblastoma. According to the authors:13
“Administration of these vaccines was unrelated to the oncologic diagnoses themselves. However, these two independent processes both came to the clinical forefront following vaccination. We hypothesize that the inflammatory response to the COVID vaccine may have played a role in increasing clinical symptoms in these patients, potentially in relation to the COVID-19 spike protein …
Although the precise mechanism of post-vaccination inflammation is unknown, it is known that spike proteins can initiate inflammatory cascades and cross the blood-brain barrier (BBB) in COVID-19 infections.
It is possible that encoded spike proteins post-vaccination therefore cross the BBB and enhance inflammatory responses to nascent pathology within the brain following vaccine administration.
We believe that an augmented inflammatory response following vaccination called attention to these neuro-oncologic diseases by exacerbating peritumoral edema and worsening clinical symptoms.”
CDC Is Hiding Breakthrough COVID Infections
VAERS is not the only place where data are being manipulated to hide problems associated with the COVID shots. The CDC is also manipulating its data collection and reporting of breakthrough cases, meaning people who contract COVID-19 after being partially or fully “vaccinated,” to make the shots appear more effective than they really are. In a June 24, 2021, Trial Site News article, Joel Hirschhorn writes:14
“How well does the artificial immunity provided by experimental COVID vaccines really work to protect people from getting infected? The answer is revealed by how many ‘breakthrough’ infections develop two weeks or more after full vaccination. But can we trust the federal government to collect comprehensive data on them? Now, the answer is NO.”
Originally, the CDC recommended labs use a PCR cycle threshold (CT) of 4015 when testing for SARS-CoV-2 infection. This, despite CTs above 35 were known to create a false positive rate of 97% or more.16 By using an exaggerated CT, healthy people were deemed to have COVID-19. The pandemic fraud was further propped up by falsely claiming that asymptomatic carriers were responsible for a large portion of the spread.
Now, in what appears to be a clear effort to hide COVID-19 breakthrough cases, the CDC has lowered the CT considerably — from 40 to 28 or lower17 — when testing “vaccinated” individuals. So, as vaccinated individuals are contracting the illness, they’re now far less likely to register as positive cases.
But that’s not all. To boost the appearance of vaccine efficacy even further, the CDC also will no longer record mild or asymptomatic infections in vaccinated individuals as “COVID cases.”
The only cases that now count as COVID cases — if the patient has been vaccinated against COVID-19 — are those that result in hospitalization or death.18 Meanwhile, if you’re unvaccinated and come down with a mild case, or if you test positive at a higher CT and have no symptoms, you still count as a COVID case.
As of April 30, 2021, the CDC had received a total of 10,262 reports of vaccine breakthrough infections,19 which it admitted was a “substantial undercount,” as they’re using a passive surveillance system that relies on voluntary reporting from state health departments.20 May 17, 2021, that number was slashed to 1,949, as the new guidance took effect.
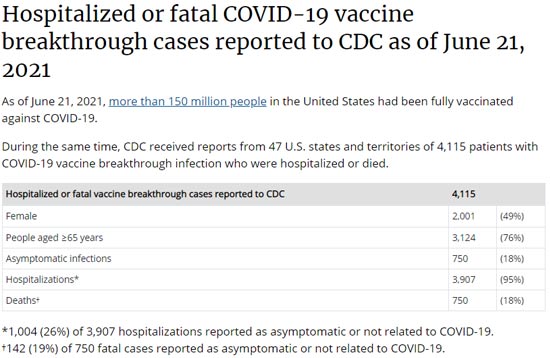
Alas, breakthrough cases continue to rapidly accumulate, even with the laxer reporting rules. By June 21, 2021, the CDC reported 4,115 breakthrough cases resulting in hospitalization and/or death.21
COVID Shot Increases Your Susceptibility to COVID Death
As noted by Hirschhorn,22 several doctors are now reporting that the majority of COVID-19 cases they see are fully vaccinated individuals. Dr. Harvey Risch of Yale, for example, claims the fully vaccinated account for 60% of his COVID caseload.23 This clinical observation stands in stark contrast to what you’ll read in the mainstream news. Lately, a slew of articles has been published declaring that most COVID deaths are now occurring in unvaccinated people.
U.K. data also show vaccinated people are at significantly increased risk of dying from the Delta variant of SARS-CoV-2 than unvaccinated ones, which suggests antibody-dependent enhancement (ADE) might be at play.
A June 11, 2021, report24 by Public Health England shows that as a hospital patient, you are nearly six times more likely to die of the COVID Delta variant if you are fully vaccinated, than if you got no COVID shots at all. The information shows up in Table 6 on page 15, which lists emergency care and deaths by vaccination status and confirmed Delta cases from February 1, 2021, to June 7, 2021.
Of 33,206 Delta variant cases admitted to the hospital, 19,573 were not vaccinated. Of those, 23 (0.1175%) died. But, of the 13,633 patients who were vaccinated with either one or two doses, 19 (0.1393%) died, which is an 18.6% higher death rate than for the unvaccinated patients.
Seven of the 5,393 patients who had received one dose 21 days or more before admission died (0.1297%). Of the 1,785 patients who had both vaccine doses 14 days or more before admission, 12 (0.6722%) died. This death rate is 5.72 times higher than that for unvaccinated patients. To put this into perspective, if all 33,206 patients had been fully vaccinated, there would have been 223 deaths instead of 42.
COVID Shots Are Clearly Far Riskier Than Advertised
As noted in a June 22, 2021, Wall Street Journal article,25 while VAERS cannot tell us whether the shots were causative in any given side effect report, when you see clusters of reports that form a trend, it’s time to investigate.
Four serious adverse effects that are currently trending are thrombocytopenia (low platelet count), noninfectious myocarditis (heart inflammation), especially in those under 30, deep-vein thrombosis and death.26
For such effects to be tolerable, even if rare, the vaccine (or drug) would need to be absolutely crucial for survival. That is not the case for COVID-19 however, which has a lethality rate on par with the seasonal flu for all but the elderly and those most frail. The vaccine would also need to be an actual vaccine — something that provides immunity. COVID-19 gene therapy injections don’t do that either.
Overall, it’s clear that deaths and injuries from these shots are being swept under the rug, and we cannot allow that to continue. We must keep pushing for transparency, honesty and accountability.
If you missed my interview with Dr. Vladimir Zelenko, I encourage you to listen to it now. In it, we review protocols you can use to protect yourself, your family or those that you love who now regret getting the COVID jab.
If you’ve gotten the shot and are suffering side effects, please report it to VAERS. In the video below, National Vaccine Information Center cofounder Barbara Loe Fisher discusses the importance of filing a report if your doctor won’t, and the information you’ll need to provide.
No comments:
Post a Comment