The Tennessee SIDS Cluster
{kind=link}

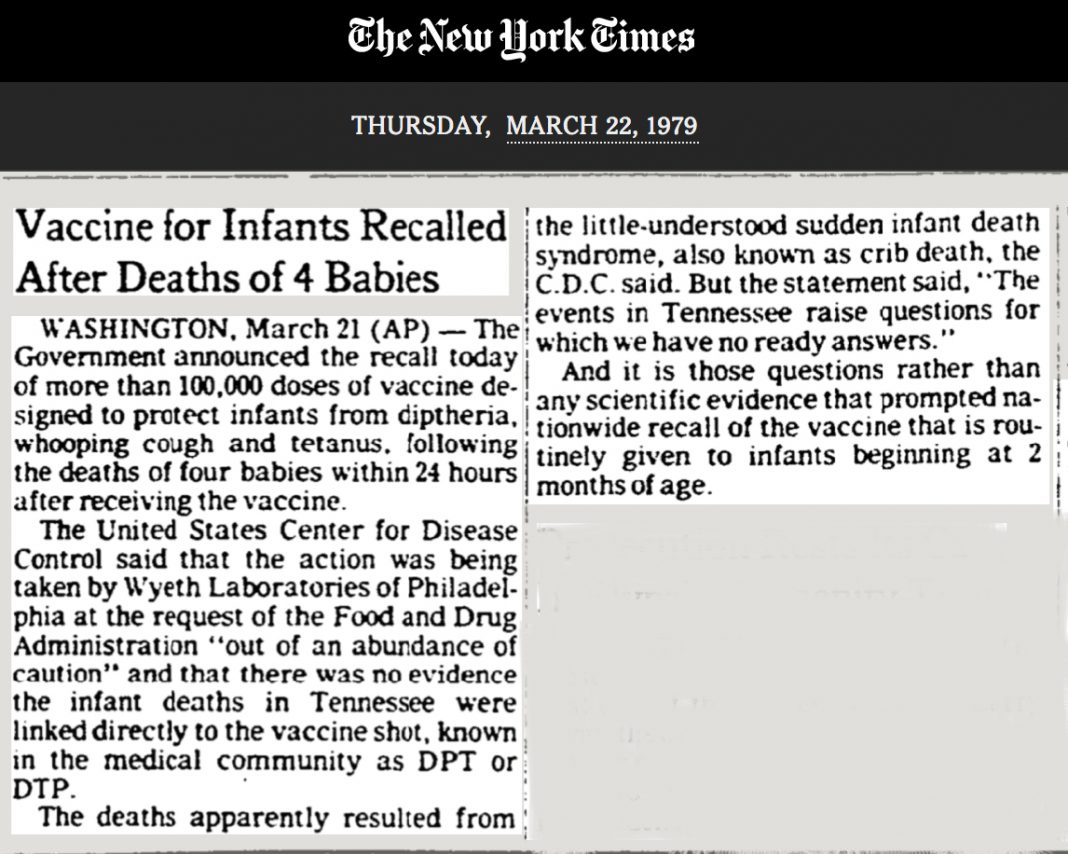
All of the deaths were classified as SIDS:
“Between August 1978 and March 1979, 77 infants in Tennessee died suddenly from unexpected causes – compared with 74 during the same period in 1977-78. These deaths were diagnosed as sudden infant death syndrome, or crib death. Of these 77 infants, eight died within a week of being vaccinated against diphtheria, tetanus and pertussis (whooping cough) using the same lot of DTP vaccine.
Of these eight infants, one died in November 1978 and one in January 1979, both within 24 hours of having been vaccinated with this lot of vaccine.
In early March, the CDC learned that two more infants had died within 24 hours of DTP vaccination, again from the same lot of vaccine produced by Wyeth Laboratories, Inc. That brought the total to four deaths within 24 hours of vaccination.”
On April 26, 1979, the US surgeon general called for a meeting with officials from CDC, FDA, top DPT researchers and drug manufacturers. The CDC reported on a survey of states that had received 7,500 or more doses of lot 64201.
The survey yielded 14 more infant deaths — half within 24 hours of a DPT shot. All were classified as crib deaths. However, the children had received vaccine from other lots.
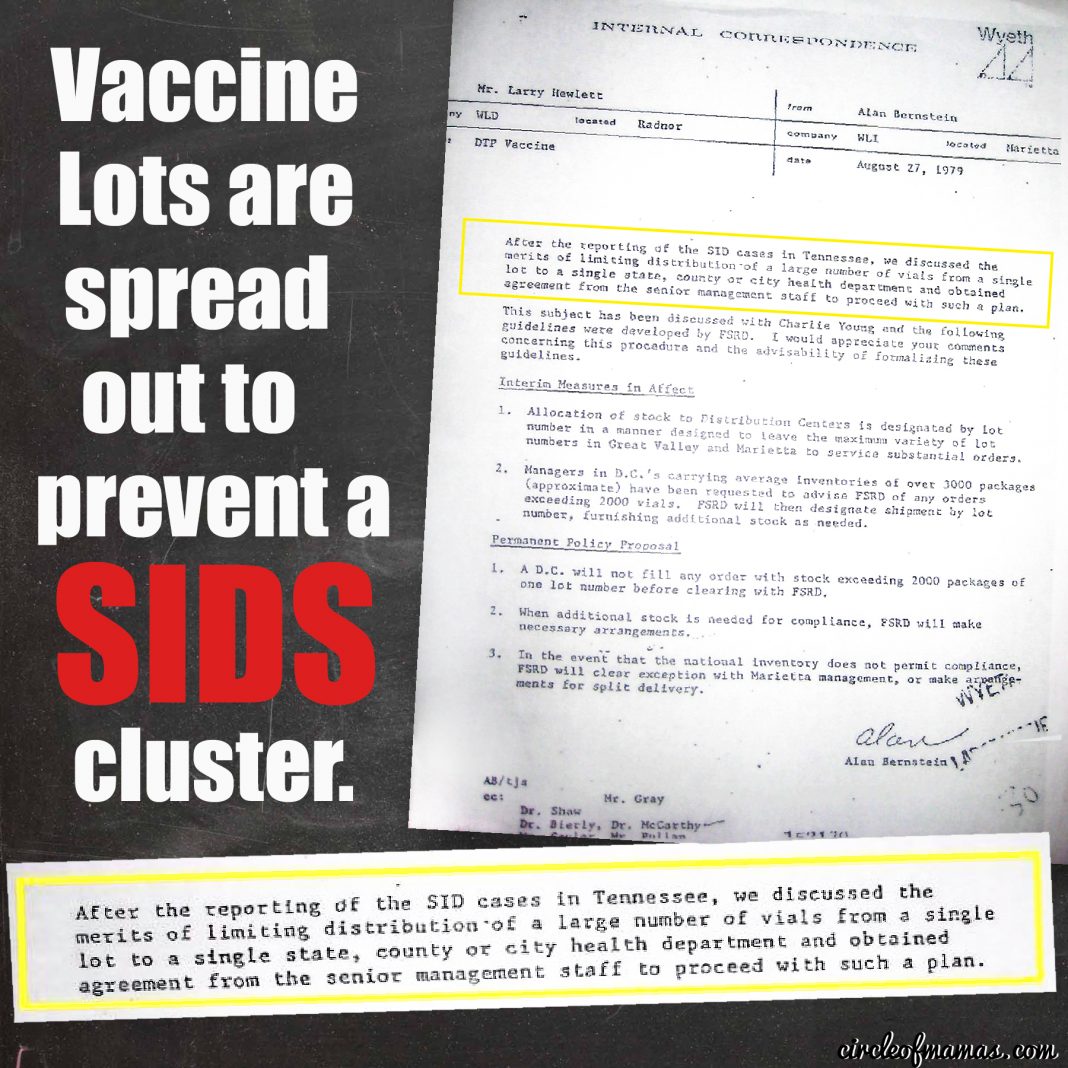
Intention To Separate Lots
Wyeth executives were concerned about the Tennessee Cluster, but their concern was more about splitting up the vaccine lots to promote “maximum variety of lot numbers”. Thus obscuring the potential to identify a “hot lot”.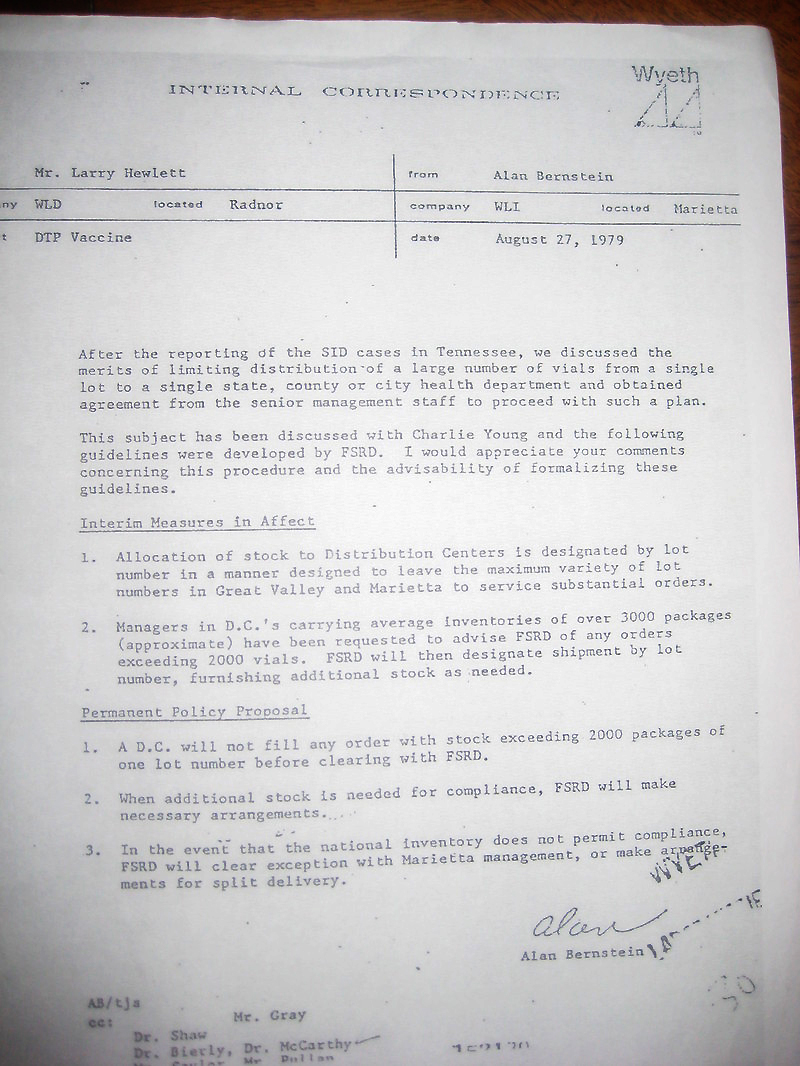
By maximizing the variety of the lot numbers, any negative reactions would be more evenly dispersed, thus breaking up a “SIDS cluster” before it could form. It doesn’t prevent SIDS from happening. It prevents us from seeing it as a cluster.
This is about protecting public perception of the DTP Vaccine, not protecting infants from harmful vaccine lots. They wanted to prevent the public awareness of a temporal association between the DTP vaccine and SIDS. Thus, apparent “hot lots” would be more evenly distributed across the United States, rather than in one geographic region.
Reports and Findings
Three years later, the first major article about the so-called Tennessee cluster appeared in the Journal of Pediatrics but the conclusions were not conclusive:“The panel could not find a causal relationship between lot 64201 and crib death although it could not exclude one, either.”
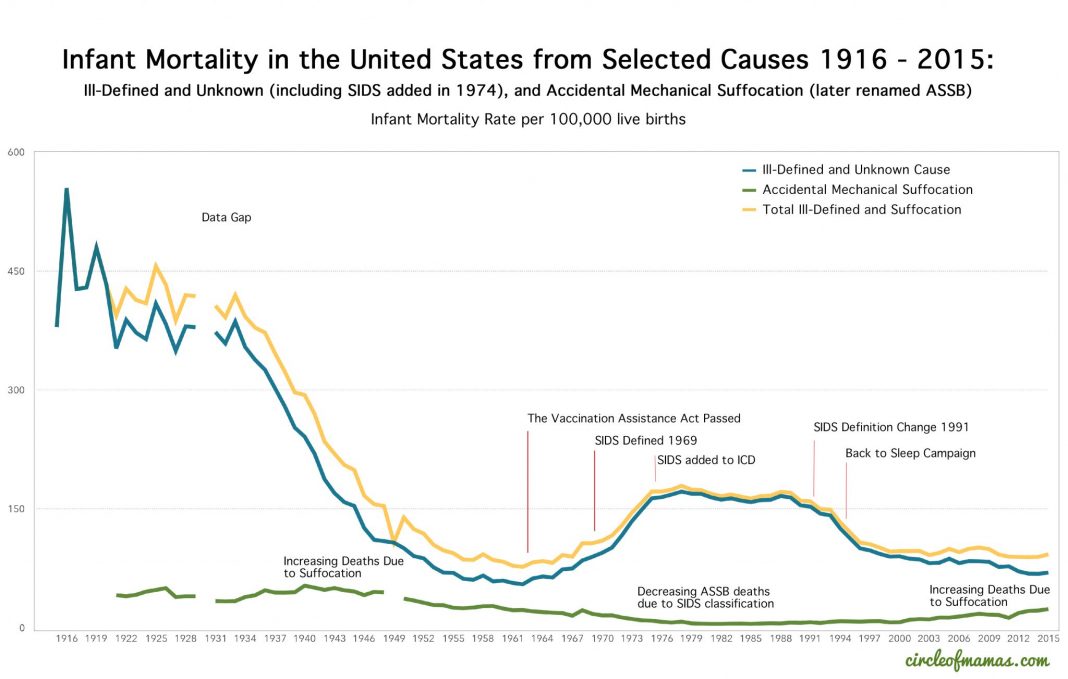
The DTP vaccine was phased out in the United States beginning in 1991 for doses 4 and 5, and completely phased out by 1996 for the first three doses. It is unknown if doctors had independently made the switch for the first three doses beginning in 1991, as an off-label use. I suspect they did because deaths due to SIDS began falling in 1991, several years before any “Back to Sleep” campaign would begin.
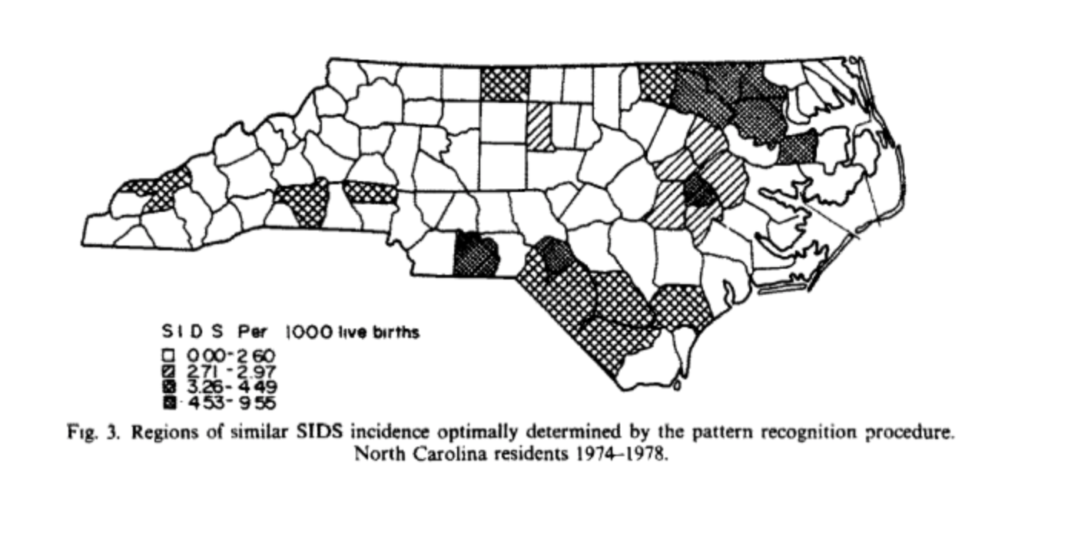
Other Clusters
Meanwhile, around the country other SIDS clusters had been identified:Right next door to Tennessee in North Carolina, researchers had already been looking to see if there was a geographical aspect to SIDS. An interesting spacial pattern was observed. Looking at SIDS deaths from 1974-1978, counties in North Carolina had a range from 0.0 to 9.6 SIDS deaths per 1,000 live births. Research continued and deaths from 1979-1984 were also tracked by location.
In Fresno County, California, Coroner Dr. David Hadden researched records from an unusual cluster of crib deaths in 1981. He said the question about DPT vaccination was not routinely asked of parents and that he would add a section for DPT vaccine receipt.
In El Cerrito, California, Dr. Kevin C. Geraghty independently researched 10 crib deaths in Contra Costa County in the first half of 1983. He found a possible association between DTP vaccine and SIDS. Hundreds of FOIA requests later, he had amassed:
“Hundreds of complaints from physicians to drug companies going back 30 years, microfilm containing thousands of adverse-reaction reports to the national Centers for Disease Control, copies of articles from medical journals on pertussis vaccine, and court depositions and documents obtained from the manufacturers and the Food and Drug Administration about laboratory tests on the vaccine.”
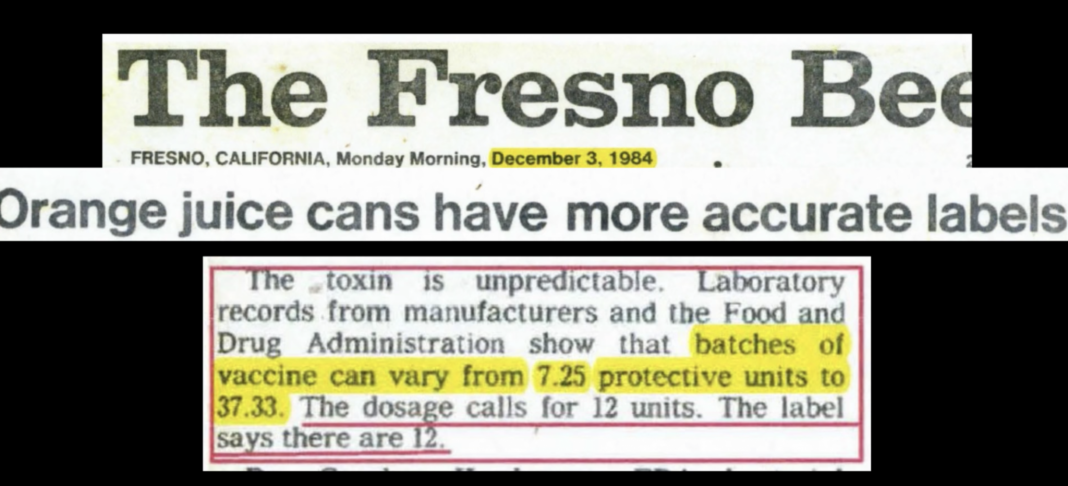
Dr. Geraghty found that the amount of endotoxin in the DPT vaccine varied from 7.25 protective units to 37.33, even though the label said there was 12.
He told the Fresno Bee:
“Let’s drop this nonsense about crib deaths,” Geraghty said. “We don’t think they are crib deaths. We think they are shock like deaths that out of incompetency the Centers for Disease Control began to call crib deaths with no proof and the coroners innocently have followed along with this practice.”
“These SIDS deaths were significantly more than expected were there no association between DTP immunization and SIDS.”
Studies Linking DPT to SIDS
Around the world, over the years, there have been many studies that see a higher incidence of SIDS in the days after a DPT vaccine:In 1946, Jacob Werne and Irene Garrow wrote about “Occurrence in Identical Twins Following Second Injection of Diphtheria Toxoid and Pertussis Antigen.”
“DPT Immunization and SIDS” by Kalyani Srinivas et al. found mortality with SIDS in the period zero to three days following DPT to be 6.9 times that in the period beginning 30 days after immunization. The DPT vaccine is still used in developing countries.
In West Africa, this study found that the DTP as the last vaccine received may be associated with slightly increased mortality.
In the Puget Sound in Washington, Walker et al. found that “SIDS mortality rate in the period zero to three days following DTP to be 7.3 times that in the period beginning 30 days after immunization.”
Dr. William Torch of the University of Nevada School of Medicine at Reno found that:
“He found that two-thirds of the children had received DPT immunizations in the three weeks prior to their deaths. Many of them died within a day after getting a shot. He maintained that this was not a matter of mere coincidence and concluded that a “causal relationship is suggested” in at least some cases of crib death affecting young infants.”
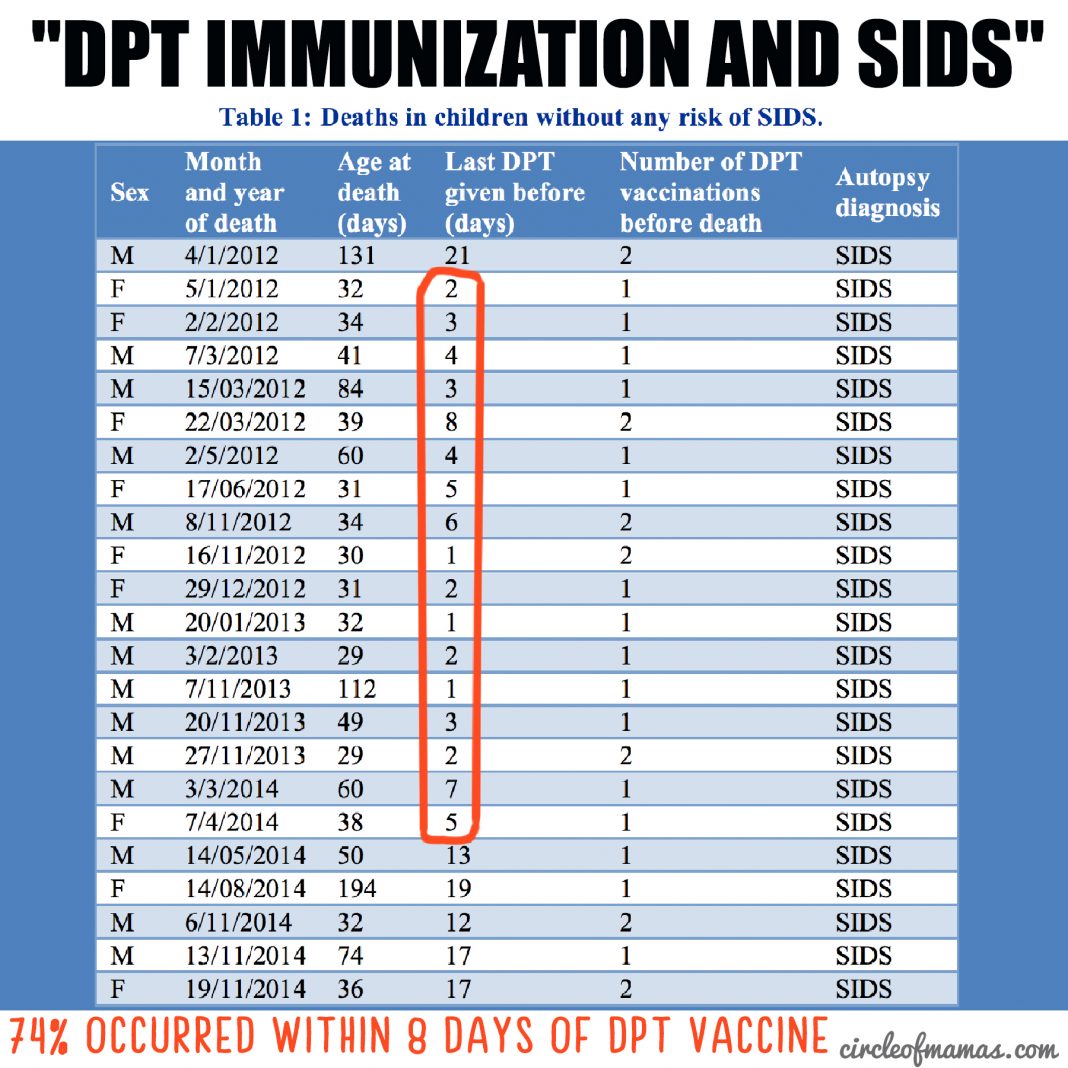
GlaxoSmithKline (GSK) disclosed in a confidential report to the Regulatory Authority about 72 babies died within 20 days of receiving Infanrix Hexavalent vaccine.
Dr. Jacob Puliyel analyzed the data and found that:
“Among the infants, there was a clustering of deaths immediately following vaccination, with 42 deaths taking place in the first three days after vaccination, and only 8 in the next 3 days. Among those below one year of age, 54 deaths (93%) occurred in the first 10 days, and 4 (7%) in the next 10 days. Had the deaths been “coincidental SIDS deaths”, this disparity in the number of deaths in the two time periods would not have been observed. SIDS deaths would have been spread uniformly over the 20-day period. The fact that the rate of death decreases rapidly with the passage of time following immunisation suggests that the deaths could be related to vaccination.
Similarly, among children older than one year, 5 deaths (83.3%) occurred in the first 10 days and 1 death (17%) occurred in the next 10 days. “
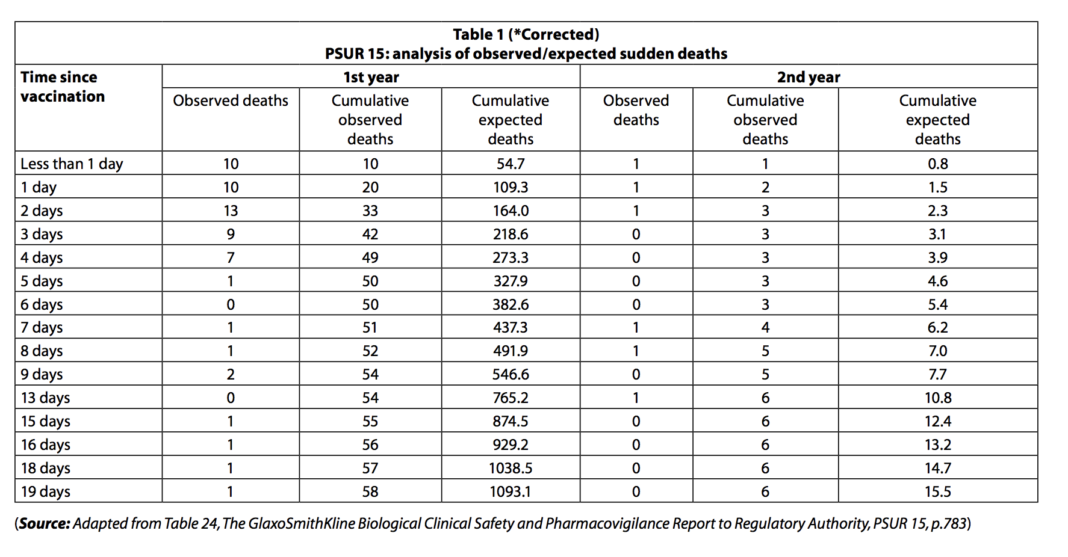
The GlaxoSmithKline “cumulative expected deaths” is set very high to make the deaths look low. But 93% of the infant deaths under 1 year occurred during the first 10 days, and only 7% of deaths occurred in the next 10 days.
If 93% of SIDS occurs in the 10 days after vaccination, it is being caused by vaccination.
Watch Dr. Suzanne Humphries discuss how various lots of Pertussis containing vaccines have over the years, had vastly different quantities of endotoxins, and also undisclosed types of aluminum adjuvants. One aluminum adjuvant is: amorphous aluminum hydroxyphosphate sulfate, which is currently in Gardasil9, and it turns out was in a lot more pediatric vaccines in the 1980s than we realized:
“Aluminum is in the vaccine in order to light a fire in the body, and trigger inflammation.”
Sources:
http://www.whale.to/vaccines/fresno3.html
http://epibulletins.dhss.alaska.gov/Document/Display?DocumentId=1340
http://www.whale.to/vaccines/fresno5.html
https://www.ncbi.nlm.nih.gov/pubmed/6835859
http://www.stat.ucla.edu/~nchristo/statistics13/stat13_lab3_w16.pdf
https://academic.oup.com/ije/article/33/2/374/715842
http://www.ijpediatrics.com/index.php/ijcp/article/viewFile/470/433
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1647245/pdf/amjph00259-0017.pdf
No comments:
Post a Comment